
Abstract
Introduction
Cryotherapy makes use of the stimulating effect of an extremely low temperature (–100°C) that is applied externally to the body for a period of around three minutes [1, 2]. According to the methodology for using this treatment on persons with illnesses, cryotherapy should be followed immediately by kinesitherapy. The indications for applying cryotherapy include, first and foremost, a chronic illness of the musculoskeletal system, which is accompanied by pain and reduced physical fitness, i.e. conditions that commonly occur in elderly persons. Due to the serious illnesses that seniors frequently suffer, especially those of the cardiovascular system, an elderly age is indicated as a relative contraindication for whole-body cryotherapy [3, 4]. It has been observed that plasma viscosity and blood viscosity increase with age, which is directly related to a decrease in the erythrocyte deformability, an increase in the erythrocyte aggregation and a decrease in the blood flow speed [5–11]. The above changes are also risk factors for cardiovascular diseases in older persons. A decrease in the temperature of the lower limbs and the face, as well as the dehydration which may occur after physical effort, increases the viscosity and the production of red blood cell aggregates [12]. However, this is not identical to whole-body cryotherapy. In the available literature, no publications investigating the changes in the rheological properties of older people who underwent whole-body cryotherapy were found. Therefore, it is not known whether this is a safe rehabilitation method.
Objective
The aim of this study was to evaluate the changes in the rheological parameters of blood in older women with spondyloarthrosis, who underwent a series of 10 whole-body cryotherapy sessions.
Methods
Participants
The study encompassed 69 women from an urban environment (with a mean age of 66.6 years), who lived in Krakow and who were being treated on an outpatient basis due to chronic lower back pain caused by spondyloarthrosis. The length of the treatment of the patients was 12 days. The inclusion criteria for the study were as follows: age between 65 and 70 years; baseline intensity of pain no greater than 5 points on a 10-point Visual Analogue Scale (VAS) for pain (where 0 denotes the lack of pain and 10 denotes unbearable pain); diagnosis of lumbar spondyloarthrosis confirmed by imaging documentation (an X-ray, CT or MRI) made by a physician specialising in medical rehabilitation; and a voluntary agreement to participate in the study. The criteria for exclusion from the study were as follows: exacerbation of the illness (acute pain exceeding 5 points on the VAS); other serious illnesses of the musculoskeletal system; chronic inflammatory diseases; and illnesses constituting a contraindication for whole-body cryotherapy. Due to the methodology of the procedure, which involved combining whole-body cryotherapy and kinesitherapy, the experimental group was randomly divided into three sub-groups that underwent different physiotherapeutic procedures: only whole-body cryotherapy (the ‘Cryo’ group, n = 22 female study participants,
Study protocol
The physiotherapy was applied every day, five days a week (Monday to Friday), for a period of two weeks. The whole-body cryotherapy treatments were performed in an open cryochamber, Model 0401 (Juka, Poland). The temperature in the cryochamber was –120°C, and the temperature in the pre-chamber was –60°C. First, the participants entered the pre-chamber for a period of 30 seconds, and then they entered the proper chamber for a period of three minutes. The women participating in the therapy wore appropriate clothing, and the treatments were applied according to the methodology described by Brojek and Warzocha [13]. Kinesitherapy, in the form of active exercises performed on a mattress, was conducted in groups comprising between 5 to 12 people. It involved active exercises to strengthen the muscles of the back, abdomen and limbs. Additionally, the participants performed balance and breathing exercises (diaphragmatic breathing). Each session began with a 5-minute warm-up, followed by a 25-minute main part and a 10-minute cool down. The aim of these exercises was to strengthen and increase the flexibility of the muscles of the trunk, as well as the muscles of the lower and upper limbs. The intensiveness of the exercises was chosen according to the guidelines of the US Centers for Disease Control and Prevention. 1
The evaluation of the properties of the blood encompassed a complete blood count, measurements of the plasma viscosity, and measurements of the erythrocyte elongation and aggregation indices. Moreover, the amount of fibrinogen was measured during the study. Venous blood that was collected one day before and one day after the therapy was used for the analysis.
Complete blood count parameters were determined with the ABX Micros 60 Analyser and included the following measurements: white blood cell count (WBC), red blood cell count (RBC), platelet count (PLT), hematocrit (HCT) and haemoglobin concentration (Hgb).
The plasma viscosity was measured with a D-52159 Roetgen viscometer (Myrenne, Germany).
The measurement of the erythrocyte deformability involved a calculation of the elongation and aggregation indices according to the Hardeman method [14]. The tests were conducted with a Laser-assisted Optical Rotational Cell Analyser (LORCA) (RR Mechatronics B.V., Netherlands). The erythrocyte deformability was expressed through the elongation index (EI) with respect to the various values of shear stress (SS). In order to measure the elongation index, blood was subjected to shear stress ranging from 0.30 to 59.97 Pa at 37°C. Next, based on the measurements, the elongation index (EI) was determined using a computer. The obtained measurements indicated the level of elasticity of the red blood cells. The erythrocyte aggregation was determined after centrifugation was performed in the cylinder of a LORCA analyser (shear rate >400s–1). The kinetic parameters of the red blood cell aggregation, i.e. the aggregation index (AI, in %), as well as the amplitude and total extent of the aggregation (AMP, in arbitrary units) and the half-life (T½, in s) were calculated using a computer [14].
The level of fibrinogen was measured with a Chrom 7 coagulation analyser (Bio-Ksel, Poland). The measurement was based on the optical changes in viscosity that occurred during the formation of a clot, and on the kinetic analysis of this reaction. For the purpose of determining the concentration of fibrinogen, 25μl of plasma was added to 50μl of thromboplastin with calcium chloride.
Statistics
The continuous variables are presented as the mean value±standard deviation (SD), or as the median and an interquartile range, depending on the normality of distribution. The normality of distribution was tested using the Shapiro-Wilk test. The differences between the sub-groups that existed before the intervention were evaluated with the analysis of variance (ANOVA). Changes between the baseline parameters and the end-of-treatment parameters were assessed by using either the t-test for dependent samples, or the Wilcoxon signed-rank test, depending on the normality of distribution.
The SS1/2 and EImax parameters were calculated using Prism 6.2 software (GraphPad Software Inc., La Jolla, CA), by applying the algorithm of a nonlinear elongation curve fitting to the three-parameter Streekstra-Bronkhorst model. The abovementioned method has been described in detail in the literature [14, 15].
The calculations were performed using Statistica 10 software (StatSoft®, USA). All p-values were two-tailed, and the statistical significance was assumed at p≤0.05.
The research project was carried out with the permission of the Bioethics Committee at the Regional Medical Chamber in Krakow (No. 60/KBL/OIL/2011).
Results
The analysis of the blood properties, such as the complete blood count parameters, plasma viscosity (MPV), elongation parameters, aggregation parameters and the amount of fibrinogen, did not reveal any statistically significant differences between the research groups and the control group.
Participation in the different therapeutic sessions also did not have a statistically significant effect on the complete blood count parameters (Table 1).
Mean values±standard deviations of selected complete blood count parameters before and after the treatment
Mean values±standard deviations of selected complete blood count parameters before and after the treatment
WBC - white blood cell count, RBC - red blood cell count, HGB - hemoglobin, HCT - hematoctit, MCV - mean cell volume, PLT - platelet count, RET - reticulocyte percent. KT - kiniesitherapy group, Cryo - whole-body cryotherapy group, KT + Cryo - combined kinesitherapy and cryotherapy group.
The mean values of the parameters related to elongation (SS1/2 and SS1/2/EImax) indicated a statistically significant decrease in erythrocyte deformability after the rehabilitation treatments in the group of women that attended both cryotherapy and kinesitherapy. The above mentioned decrease was characterised by a significant increase in SS1/2 and SS1/2/EImax, which were initially at the same level as in the control group (Figs. 1 and 2). The discussed parameters displayed the same tendency in the group of women who attended only cryotherapy; whereas the tendency was the opposite in the group of women that underwent only kinesitherapy. The changes observed in these groups were not statistically significant.
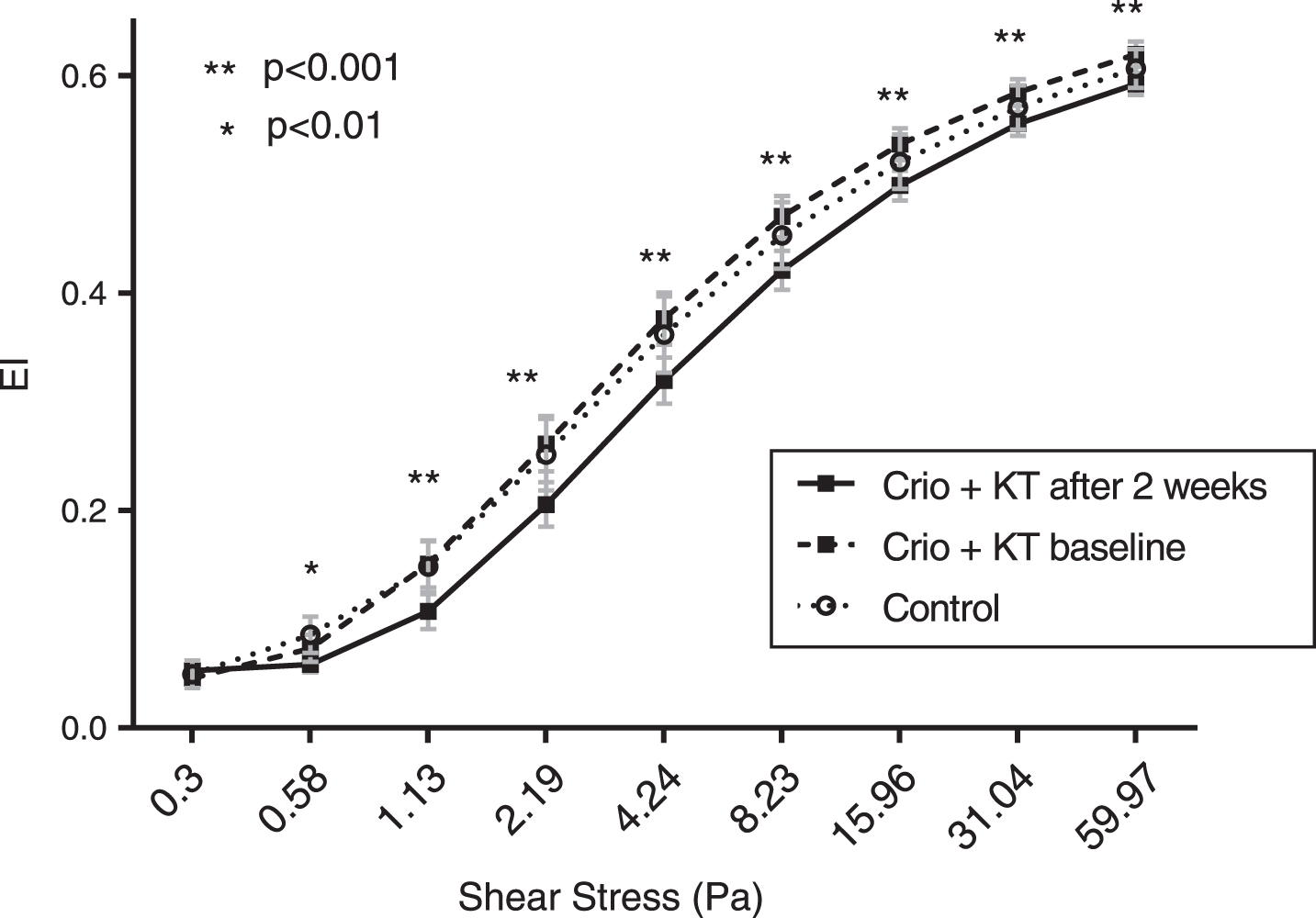
Elongation index (EI) - shear stress curves in the beginning and after 2 weeks of the combined cryotherapy + kinesiotherapy (Cryo + KT). Statistically significant differences between the baseline and end-point measurements in Cryo - KT group are marked with appropriate asterisks.

Changes of the SS1/2, EImax and SS1/2/EImax elongation indices. Statistically significant differences are marked on graphs. KT - kiniesitherapy group, Cryo - whole-body cryotherapy group, KT + Cryo - combined kinesitherapy and cryotherapy group.
The study revealed a statistically insignificant decrease in the mean values of the plasma viscosity. Moreover, a statistically insignificant decrease in the level of fibrinogen in the blood was observed in all groups; however, the greatest decrease was noted in the group of women that participated only in cryotherapy, in which the baseline mean value of the discussed parameter was the highest (Fig. 3).
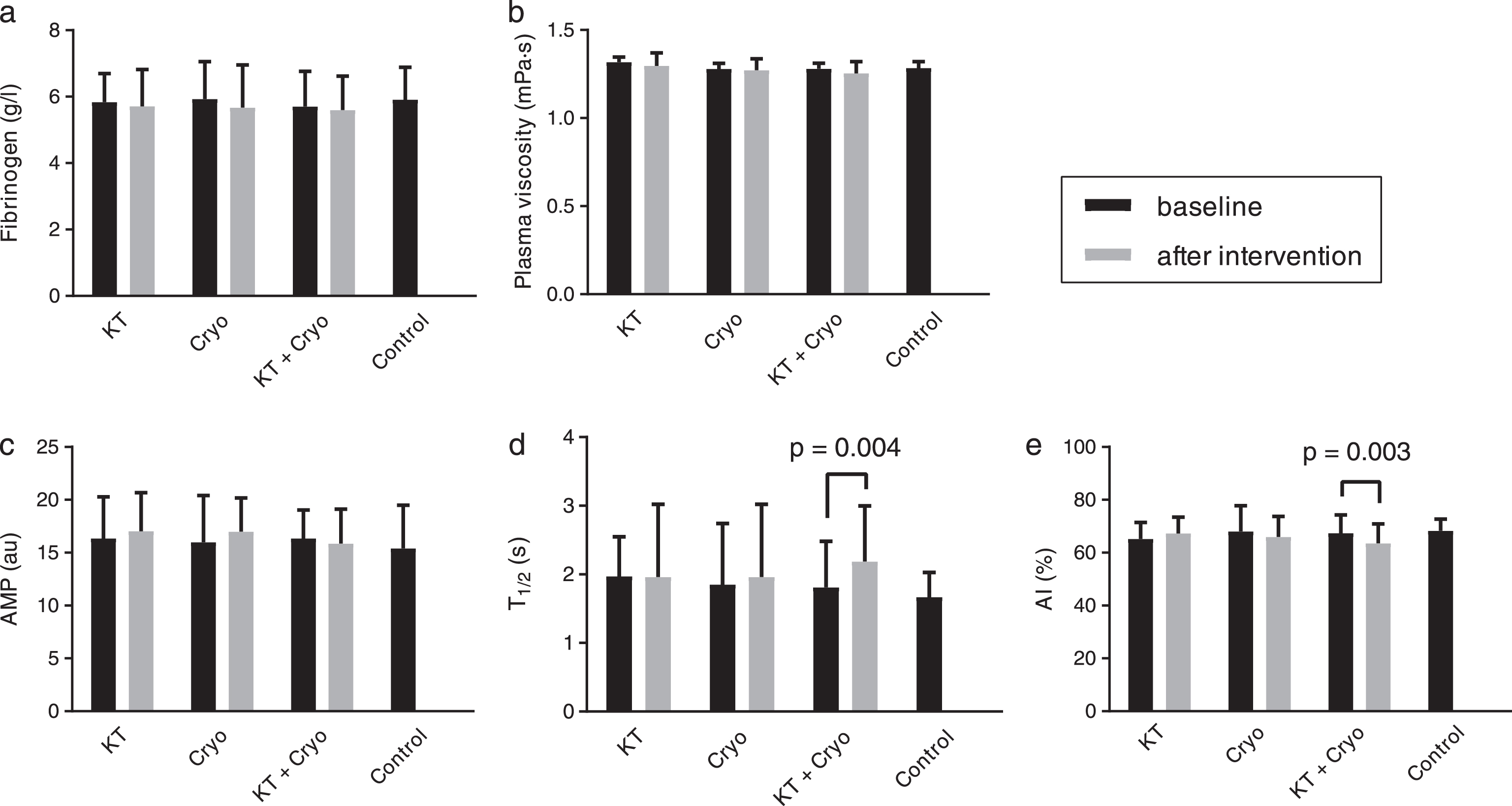
Grouped bar charts of fibrinogen, plasma viscosity and aggregation parameters. Statistically significant values are marked on graphs. AMP - total extent of aggregation, T1/2 - half time of total aggregation AI - aggregation index. KT - kiniesitherapy group, Cryo - whole-body cryotherapy group, KT + Cryo - combined kinesitherapy and cryotherapy group.
The analysis of the mean values of the parameters connected with aggregation revealed a statistically significant change in the aggregation index (AI), which decreased after the rehabilitation treatment in the group of women that participated in both cryotherapy and kinesitherapy. Furthermore, the study observed an increase of T1/2 in the KT+Cryo group. In the other groups, no statistically significant changes were observed (Fig. 3).
Whole-body cryotherapy is a popular therapeutic method among the elderly with illnesses of the musculoskeletal system, including those with spondyloarthrosis. It is believed that applying extremely low temperatures to a human body causes a completely different reaction than the application of temperatures that decrease the body temperature. Cryotherapy is believed to not only alleviate pain, but also to increase the perfusion of tissues after the treatment through the compensatory expansion of vessels. The authors’ interest in the subject resulted from the fact that a series of cryotherapy treatments may also cause changes in the rheological parameters, and especially since there are currently no related reports from studies carried out among older persons.
An efficient blood flow, and thus the correct functioning of the body, requires an appropriate erythrocyte deformability, [16] which may decrease with age [17]. This reduced elasticity leads to a decrease in the blood flow and an increase of blood viscosity. In such conditions, red blood cell aggregates form more quickly. Some authors have confirmed the increased aggregation of red blood cells in persons of an advanced age [7, 18]. As a result of the abovementioned changes, the level of tissue oxygenation decreases over the years [16]. The increased aggregation of red blood cells also decreases the cerebral blood flow, [6] and the increase of blood viscosity with age [16] may cause cardiovascular and cerebrovascular diseases [5]. Furthermore, it has been observed that mortality related to cardiovascular disorders increases in the winter period. Although the causes of this phenomenon are unclear, it seems to be related to an increased blood viscosity [19]. Blood viscosity is directly influenced by plasma viscosity; whereby an increase in plasma viscosity alone causes an increase in blood viscosity [20]. In another study, there were no apparent changes of plasma viscosity in the subjects with increasing age [21].
It has been proven that a short-term (90 minute) exposure of older persons to a temperature of 16°C, in comparison with thermoneutral conditions (28°C), causes haemoconcentration and increases the t-PA fibrinolytic parameter, which leads to the hypothesis that a short-term exposure to a slightly low temperature starts an inflammatory reaction and tends to cause a state of increased blood viscosity. These changes are highly unfavourable, particularly in older persons. Studies have indicated that death due to hypothermia, or due to causes connected with hypothermia, generally occurs after more than 10 hours or more than 10 days following the event, which suggests the appearance of haematologically unfavourable changes that result in death [22]. However, Cabrales and Intaglietta showed that moderate increases in viscosity factors may trigger vasodilation, and thus improve blood flow [23].
Some authors have observed an increase in the level of fibrinogen in older people [24, 25]. This phenomenon may lead to damage to the endothelium and a frequent activation of the processes of coagulation with a delayed fibrinolysis [16]. Istrati et al. [26] observed that whole-body cryotherapy caused significant disorders in the regulation of the fibrinolytic system, indicating the possibility of the occurrence of thrombosis and other cardiovascular complications. Stanek, [27] on the other hand, indicated a statistically significant decrease in the amount of fibrinogen after a series of 10 2-minute cryotherapy treatments combined with 60-minutes of kinesitherapy. Conversely, in the current study, no significant effect of the applied methods on the amount of fibrinogen was observed; and in fact, all of the groups showed an insignificant and favourable decrease in this parameter.
Yalcin, [28] in her study of rats that were subjected to swimming noted that, a day after the effort, the aggregation of erythrocytes increased in the untrained rats, while the level of elasticity of the erythrocytes decreased. It seems interesting that the level of TBARS (Thiobarbituric Acid Reactive Substances) increased after 24 hours. This indicator is considered to be a measure of oxidative stress. It is therefore very probable that this delayed effect reflects the initiated inflammatory process, which may impair the rheological properties of blood. The connection of cryotherapy with the activation of the immunological system and its effect on oxygen free radicals is fairly well described in the available literature [29–32].
In the present study, the second blood measurement was performed 16 hours after the last physiotherapeutic treatment. The results of this study indicate a considerable impairment in erythrocyte deformability in the group of persons that underwent both cryotherapy and kinesitherapy. This, in turn, suggests that the physical stimuli led to a considerable strain on the participants’ unaccustomed bodies. This also suggests the activation of the immunological system and an increase in the production of oxygen free radicals. In the group of persons that underwent only cryotherapy, the direction of this change in erythrocyte elasticity was the same; and in the group of persons that underwent only kinesitherapy, the elasticity increased slightly. Therefore, it can be concluded that cryotherapy is a method that leads to a greater strain on the body than kinesitherapy and leads to unfavourable changes in erythrocyte deformability.
During cryotherapy treatment, the precapillary sphincters in the skin contract, which stops the precapillary flow; as a result, the oxygenated blood returns to the large venous vessels and the right side of the heart through the open arteriovenous fistulas. During the phase called reactive hyperaemia, the arteriovenous fistulas close down, which causes an increase in the blood supply to the tissues. Reactive hyperaemia continues for up to a few hours after the treatment [33]. If the rheological changes in the blood occur during the phase of reactive hyperaemia, they should not affect the efficiency of perfusion, i.e. even with a decreased deformability, the red blood cells should ‘go through’ the extended blood vessels. However, 16 hours after the treatment, the blood vessels should return to the same state as before the treatment; and therefore, a disturbance in the hemorheological parameters may affect the blood supply to the tissues. If such a tissue has sufficient autoregulatory abilities (e.g. there is a lack of atherosclerotic changes), disorders in the rheological parameters should not be an obstacle for maintaining the correct perfusion; however, if these abilities of the tissues are insufficient, as is often the case in the elderly, an additional strain in the form of an impairment of the ability of the erythrocytes to change their shape may result in an inappropriate blood flow through the tissues [28].
In the present research study, in the group with confirmed considerable disorders of erythrocyte deformability, the tendency of red blood cells to form aggregates decreased (a decrease of the AI), and the red blood cell aggregates formed more slowly (an increase of T1/2). In the other groups, the studied erythrocyte aggregation indices did not change significantly. It was also observed that in each group, the decrease in the elasticity of the erythrocytes was accompanied by an increase of their aggregation; and the increase of the elasticity was accompanied by a decrease in the ability to form aggregates. The abovementioned phenomenon may indicate a series of interrelated processes that are occurring in the blood to ensure an optimal flow.
Conclusions
The safety of using cryotherapy in older people is an open issue. Due to the worsening of the elasticity of the erythrocytes, despite the favourable changes in their aggregation parameters, the occurrence of problems with perfusion cannot be completely excluded. For this reason, the safety of using whole-body cryotherapy in these persons is debatable.
Limitations of the adopted research methodology
In order to fully evaluate the effect of cryotherapy on the rheological parameters of blood, additional measurements should be conducted in order to investigate the changes in the studied blood parameters after a longer period of time following the applied rehabilitation methods. The level of oxidative stress and the reaction of the immunological system should also be measured. This would provide information about the duration of the unfavourable changes in the blood and what causes them, and would thus confirm or invalidate the thesis that cryotherapy has a negative effect on the rheological parameters of blood, and may be harmful to older persons.