
Abstract
Keywords
Abbreviations
acoustic radiation force impulse
human epidermal growth factor receptor 2
estrogen receptor
progesterone receptors
hormone receptor
Breast Imaging Reporting and Data System
region of interest
shear wave velocity
ultrasound
virtual touch tissue imaging
virtual touch tissue quantification
Nottingham Histology Grade
the receiver operator curve
Introduction
Triple-negative breast cancer refers to the subtype of breast cancer that lacks the human epidermal growth factor receptor 2 [HER2], estrogen receptor(ER) negative and progesterone receptors (PR) negative [16]. Although triple-negative breast cancers account for only 15% – 20% of all breast cancers [27], they are currently receiving a large amount of research attention, which is appropriate given their disappointing prognosis, unique biology, aggressive and early metastasis, and poor chemotherapy response when compared with endocrine-sensitive and HER2-positive breast cancers. It has been reported that triple-negative breast cancer occurs more frequently in younger women with a family history of breast cancer [8].
Breast Ultrasonography (US) is the preferred imaging method for the identification of breast lesions. US features that can be used to predict biological behavior include tumor size, shape, margin, boundary, internal echo, the ratio between tall and wide and the internal blood flew signals. It is widely used to screen for breast lesions because of its simple approach, non-invasiveness and avoidance of radiation exposure. However, conventional US suffers from low specifity [11] and final results depend heavily on the operator’s experience [31].
Over the past 10 years, US elastography has been introduced to clinical practice for the diagnosis of breast cancer and many studies have investigated the use of elastrography. Some studies [12, 18] have shown that US elastography is highly reproducible for assessing the elastographic features of breast masses within and across observers compared with conventional US. It offers a new view to assess different aspects of the mass, because lesions that have an abnormal internal structure often show different elasticity characteristics.
Acoustic radiation force impulse (ARFI) elastography is one of the newly developed elastrography techniques [9, 24]. It is based on the principle that localized tissue displacement is less in harder tissues than in softer ones, and the tissue stiffness can be evaluated both qualitatively and quantitatively. The technique includes Virtual Touch tissue imaging (VTI; Siemens Medical Solutions, Mountain View, California, USA) and Virtual Touch tissue quantification (VTQ; Siemens Medical Solutions) [9]. VTI can evaluate tissue stiffness qualitatively, repeating the displacement process along multiple imaging lines [20]. VTQ on the other hand can evaluate tissue stiffness quantitatively and is performed by measuring the time peak displacement in a transverse direction at each lateral location and the corresponding shear-wave velocity (SWV) within the tissue [21]. Usually, stiffer tissues show a greater shear velocity [34]. The technique can overcome many limitations of previous techniques, such as high operator dependence and poor reproducibilit y [6]. It is an important complement to conventional US with studies having suggested that conventional US combined with shear wave elastography shows greater potential in the differentiation of malignant from benign breast lesions.
Triple-negative breast cancer deserves increasing attention giving to its unique biologic behaviors and the poor prognosis to women, then it would be meaningful if ARFI elastography combined with conventional US have some value in diagnosing triple-negative breast cancer. Our retrospective study aimed at evaluating the value of conventional US combined with ARFI in predicting the triple-negative breast cancer. We assumed that differences in the expression of immunological receptors might affect the internal structure of the tumor, and that would possibly be reflected in the US image.
Materials and methods
Patient selection
This research involved retrospectively reviewing the conventional US images and corresponding ARFI images of breast cancer patients. The study was approved by the institutional review board of our hospital and the requirement to obtain informed consent was waived, also the manuscript is in accordance with the ethical guidelines of Clinical Hemorheology and Microcirculation [3].
The study enrolled 236 patients with pathologically confirmed breast cancers who presented to our hospital between May 2014 and September 2015. There are 134 women who had more than one lesion, in which case we selected the largest lesion to be included in our research. The inclusion criteria were as follows: (1) all lesions were at least 5 mm in the maximal diameter; (2) patients had undergone conventional US and ARFI examinations, and imaging data were complete; (3) all breast cancers were pathologically confirmed and FISH analyses had been performed. The exclusion criteria were as follows: (1) patients who had received prior neoadjuvant chemotherapy (n = 5); (2) maximum diameter of the tumor <5 mm (n = 15); (3) obvious cystic lesions (n = 10); (4) less than five VTQ measurement results on the same lesion (n = 7); (5) incomplete or missing imaging information (n = 21).
Therefore, 58 lesions were excluded from our study, we ultimately analyzed 178 breast lesions, including 60 triple-negative breast cancers and 118 hormone receptor (HR)-positive/HER-2 negative breast cancers (Fig. 1). Of the 178 patients, the mean age for the women was 57.57±11.69 years (range, 26–88 years), and the diameter of the lesions ranged from 5 to 76 mm (mean, 22.32 mm ± 11.52).

Flowchart of the selection of the breast lesions.
The conventional US and ARFI were performed on every patient using the same S2000 US scanner (Siemens Medical Solutions) equipped with a linear 9L4 transducer (frequency range, 4–9 MHz). All the examinations were performed by a experienced radiologist in breast US and breast ARFI. Patients were examined in the supine position with their breast and armpit fully exposed. Conventional US was performed firstly including B mode US and color Doppler US and with the breast being scanned in a clockwise direction, then the supraclavicular lymph nodes and lastly the axillary lymph nodes.
Afterwards, ARFI elastography were applied. we chose the biggest and clearest section of the pathologically proven invasive cancer, keeping the probe still without compression, and switched to the elastography mode. The VTI button was pressed and a shear wave was excited with VTI images being generated [9, 16], which were then saved. Once the ARFI image was stable, the region of interest (ROI) was selected in the center of the lesion but avoiding areas of calcification (except for diffuse calcification in the lesion) and any cystic spaces. The SWV of the lesions were measured seven times without movement or compression. The VTQ images were then saved and the SWV value was objectively measured and recorded. An area of normal breast tissue with approximately the same depth of glandular layer was measured using the same principle. For each patient, the system automatically adjusted the depth, focal zone placement, and overall gain.
Image interpretation
The images obtained were reviewed independently in the same settings by two experienced radiologists with consensus.
We recorded the conventional US image characteristics with reference to the ACR-BI-RADS [19] lexicon and the lymph node status. For each lesion, we specified the size (5 mm ≤ diameter <10 mm, 10 mm ≤ diameter <20 mm, or 20 mm ≤ diameter), shape (regular or irregular), margin (smooth or rough), boundary (clear or unclear), internal echo (even or uneven), calcification (microcalcification [<1 mm in diameter], macrocalcification [≥ 1 mm in diameter with shadowing], or no calcification) and Doppler vascularity (detected or undetected).
On the VTI image we used the color gradient from bright (soft) to dark (hard) to represent the grayscale value that provided information on stiffness, so that the lesions could be visually confirmed. According to the grayscale value shown in the lesion and the surrounding normal tissue, VTI images were divided into five grades (1, 2, 3, 4a, or 4b), referencing the work of Mitsuhiro Tozaki et al. [25]. We then recorded the VTI score and the boundary definition of the mass (poorly defined or well-defined) on the VTI image, with higher grades normally indicating stiffer tissue.
In order to minimize the chance for error and bias in the VTQ results, we removed the highest and lowest measurements and the remaining measurements were averaged as the final SWV - results expressed in meters/second. The results for lesions that failed to produce an SWV, shown as “X.XX m/sec”, were replaced by 0 m/sec or 8.4 m/sec, with 0 m/sec corresponding to the cystic portion and 8.4 m/sec corresponding to the solid portion [32].
Clinicopathological data
The medical records of the patients were reviewed and data on age and distribution of lesions were compiled. Pathological reports from excisional biopsies, breast-conserving surgery or mastectomy specimens were also reviewed to determine the tumor type of the invasive tumor, its histological grade, whether the lymph node has transferred and the number of the transferred lymph node status.
The breast cancer histological grade was recorded as grade I, II or III as per the Nottingham Histology Grade (NHG) [13]. The histological diagnoses were made by one pathologist with 10 years of working experience in pathologic diagnosis. We used the routine paraffin sections as the reference standard and obtained immunohistochemical staining results by FISH analyses. The receptors we recorded included ER, PR, and HER2. The status of each receptor was considered to be negative if the expression was <10% and positive if the expression was ≥10%. The results for HER2 expression on immunohistochemical analysis were scored as negative, 1+, 2+ or 3+, according to the manufacturer’s recommendations. Specimens with a score of negative or 1+, were treated as HER2 negative [1]. We collected all the triple-negative tumors, and selected the HR-positive/HER2-negative breast cancers for comparison.
Statistical analysis
SPSS 17.0 (SPSS, version 17.0; SPSS, Chicago, Illinois, USA) was used for statistical analysis with P < 0.05 considered to indicate a significant difference. To compare the imaging findings between triple-negative breast cancer and ER-positive/PR-positive/HER2-negative breast cancer, we used the chi-squared and Fisher exact tests. The correlation of ARFI findings in patients with triple-negative breast cancer and lymphatic metastasis was analyzed with multivariate analysis. We determined the best cut-off value of the SWV for the prediction of the triple-negative histological subtype and for the risk of lymphatic metastasis in the patients with triple-negative breast cancer by analysis of the receiver operator curve (ROC). The Student t test was used to inspect that there was no tumor size-related bias or age-related bias between the two groups.
Results
In total 178 patients, all of whom were women, with a mean age 57.6±11.7 years (range 26–88) were involved in the study. The largest lesion only was studied in women who had multiple lesions resulting in 178 breast lesions being analyzed. All of lesions were invasive ductal breast carcinomas, among which there were 60 triple-negative breast cancers and 118 HR-positive/HER2-negative breast cancers.
Patient characteristics
The basic characteristics of the patients with breast cancer lesions are shown in Table 1. These indicate that women of a younger age (45.57±11.1 VS 56.42±11.8, P < 0.001) may have a higher risk of suffering from the triple-negative breast cancer. Triple-negative breast cancers were more likely to have a high histological tumor grade (50% [30 of 60] VS 22% [26 of 118], P < 0.001). The triple-negative breast cancer patients were more likely to have early lymph node metastasis (43% [26 of 60] VS 25% [29 of 118], P < 0.001) and to have more lymph nodes involved (4.46±0.783 VS 2.37±0.298, P = 0.001). In contrast, the distribution of lesions did not present a significantly association with triple-negative breast cancer compared with the non-triple-negative breast cancer (P = 0.216).
Basic characteristics of patients and their breast cancer lesions
Basic characteristics of patients and their breast cancer lesions
ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2. Numbers in parentheses are percentages. *Indicate a significant difference. # #Data are means±standard deviations.
The comparison of the conventional US findings for triple-negative and the ER-positive/PR-positive/HER2-negative breast cancer are listed in Table 2. On conventional US, significant differences were found in the tumor size (P = 0.008) and shape (P = 0.032), with tumors of larger size (67% [40 of 60] VS 44% [52 of 118]) and regular shape (58% [35 of 60] VS 16% [19 of 118]) being significantly associated with triple-negative breast cancer. In contrast, tumor boundary (P = 0.09), margins (P = 0.09), the ratio between depth and width (P = 0.170), internal echo (P = 0.069), calcification (P = 0.118) and blood flew signals (P = 0.382) showed no significant difference between the two subtypes.
The comparison of the lesion type on the conventional US between the triple-negative breast cancer and the ER-positive/PR-positive/HER2-negative breast cancer
The comparison of the lesion type on the conventional US between the triple-negative breast cancer and the ER-positive/PR-positive/HER2-negative breast cancer
ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2; d, the maximal diameter of the lesion. Numbers in parentheses are percentages. *Indicate a significant difference
The comparison of the ARFI findings between the triple-negative and ER-positive/PR-positive/HER2-negative breast cancer is shown in Table 3 and Fig. 4. It shows that the higher VTI score (27% [16 of 60] VS 14% [17 of 118], P = 0.006), a poorly defined VTI boundary (73% [44 of 60] VS 57% [67 of 118], P = 0.033) and SWV ≥3.51 m/s (63% [38 of 60] VS 43% [51 of 118], P < 0.01) are more common in triple-negative breast cancers (Figs. 2 and 3). The best cut-off value of SWV for the prediction of the triple-negative breast cancer was found to be 3.51 m/s by analysis of the ROC curve.
The comparison of the lesion type on ARFI between the triple-negative breast cancer and the ER-positive/PR-positive/HER2-negative breast cancer
The comparison of the lesion type on ARFI between the triple-negative breast cancer and the ER-positive/PR-positive/HER2-negative breast cancer
ARFI, acoustic radiation force impulse; ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2; VTI,Virtual Touch tissue imaging; SWV, shear-wave velocity. Numbers in parentheses are percentages. *Indicate a significant difference.
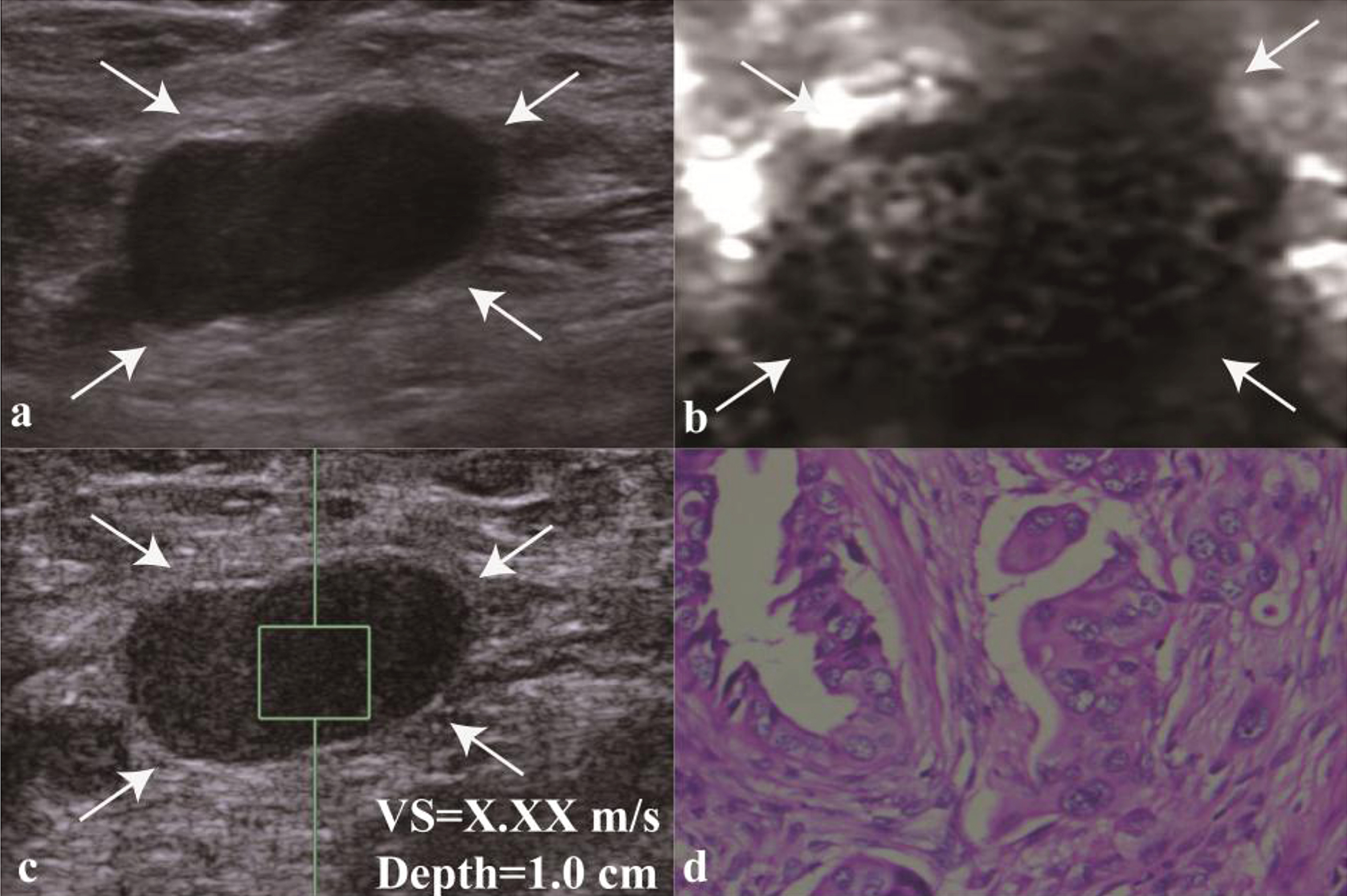
Images in a 45-year-old woman with triple-negative breast cancer. (a) At conventional US, a 21-mm lesion in the left breast (arrows in a) appears to have relatively regular shape, well defined boundary, smooth margin, no calcification. At elastography, (b) VTI grade of 4b (arrows), (c) SWV of “X.XX” m/sec (ie, 8.4 m/sec) at VTQ is assigned. (d) Histologic specimen (hematoxylin-eosin stain; original magnification, 400) shows that this lesion is finally confirmed to be a poorly differentiated breast invasive ducal carcinoma.
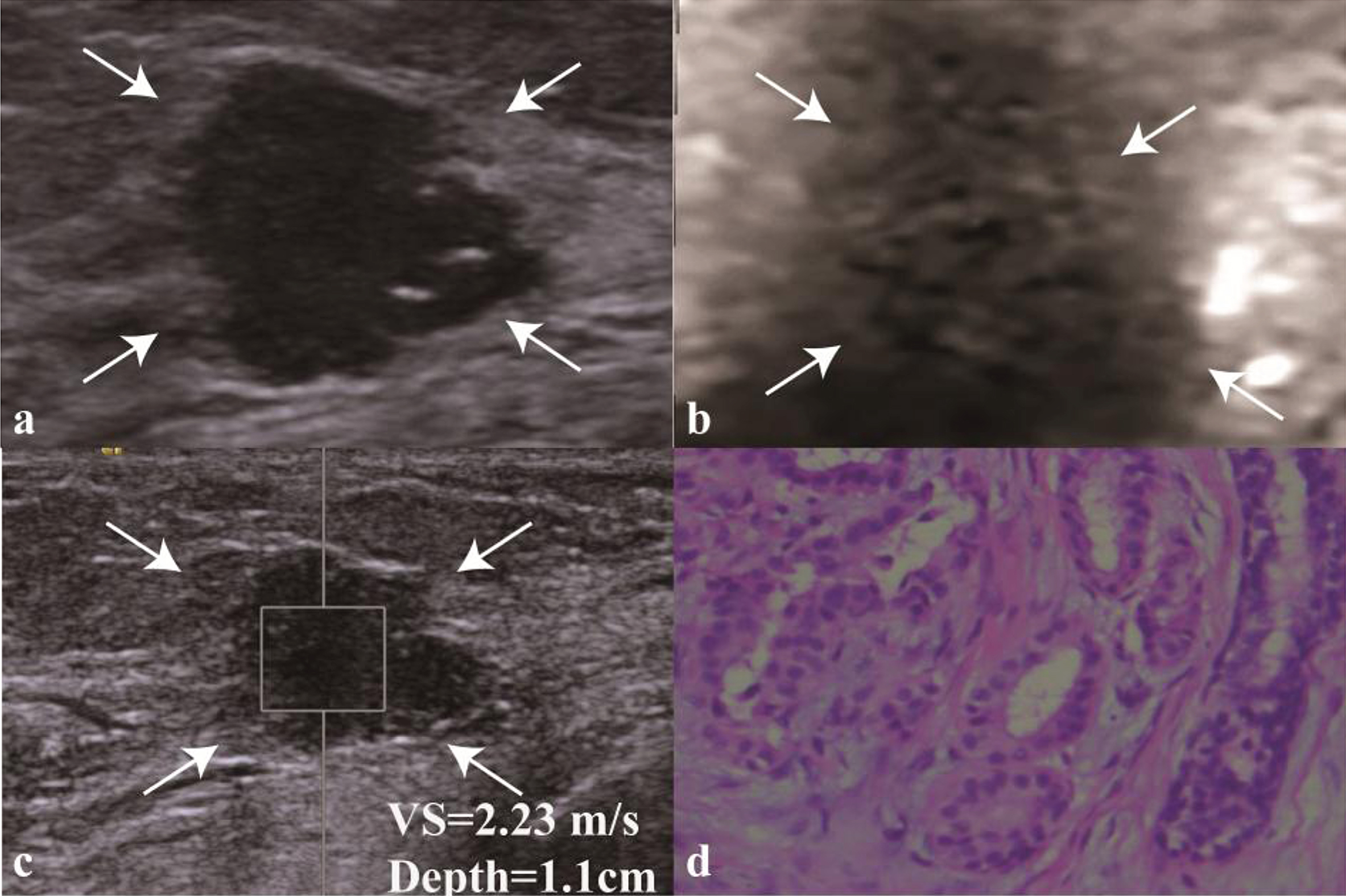
Images in a 57-year-old woman with ER-positive/PR-positive/HER2-negative breast cancer. (a) At conventional US, a 12-mm lesion in the right breast (arrows in a) appears to have relatively irregular shape, poorly defined boundary, rough margin, micro-calcification, poorly defined margin. At elastography, (b) VTI grade of 2 (arrows), (c) SWV of 2.49 m/sec (ie, 8.4 m/sec) at VTQ is assigned. (d) Histologic specimen (hematoxylin-eosin stain; original magnification, 400) shows that this lesion is finally confirmed to be a well differentiated breast invasive ducal carcinoma.

ARFI findings of the mass lesion corresponded to Table 3. The column diagram shows that (A) the higher VTI score, (B) a poorly defined VTI boundary, and (C) SWV ≥3.51 m/s are more common in triple-negative breast cancers.
Correlation of the ARFI findings in patients with triple-negative breast cancer and lymphatic metastasis is shown in Table 4 and Fig. 5. When the triple-negative breast cancers only were analyzed, significant differences were found for the highest VTI score (46% [12 of 26] VS 12% [4 of 34], P = 0.004) and an SWV ≥4.15 m/s (69% [18 of 26] VS 32% [11 of 34], P = 0.002), between patients with and without lymphatic metastasis, while the boundary on VTI was not found to be of significance (P = 0.227). The best cut-off value of SWV for the presence of lymphatic metastasis in patients with triple-negative breast cancer was found to be 4.15 m/s by analysis of the ROC curve.
Correlation of ARFI findings in patients with triple-negative breast cancer with the lymphatic metastasis
Correlation of ARFI findings in patients with triple-negative breast cancer with the lymphatic metastasis
Numbers in parentheses are percentages. *Indicate a significant difference.
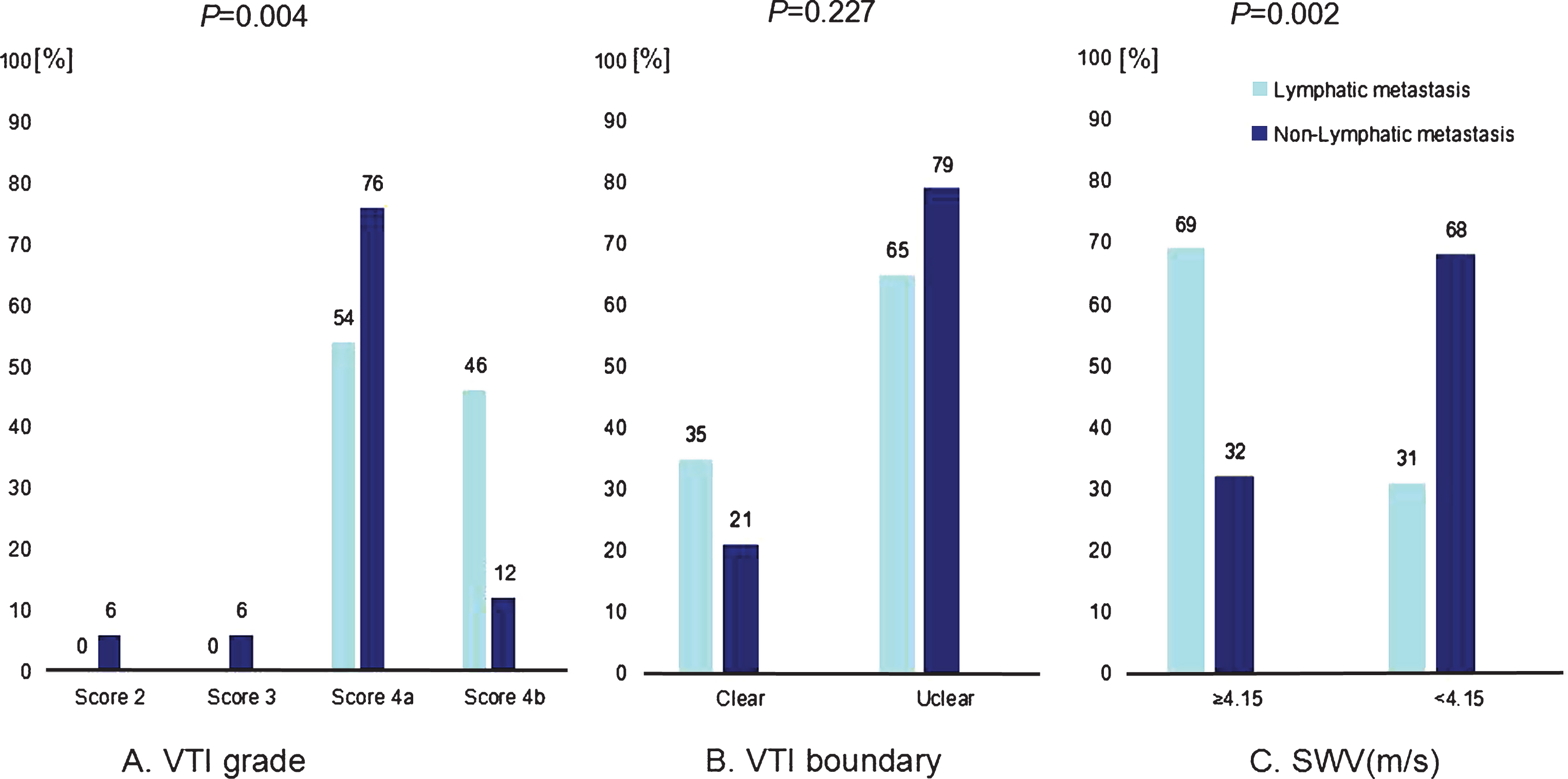
Correlation of ARFI findings in patients with triple-negative breast cancer and lymphatic metastasis corresponded to Table 4. The column diagram shows that patients with (A) the highest VTI score (i.e.grade 4b) and (C)SWV ≥ 4.15 m/s tend to have higher risk of lymphatic metastasis; but (B) the boundary on VTI was not found to be of significance.
Although accounting for only a relatively small proportion of breast cancers, triple-negative breast cancers are aggressive in nature and responsible for a large proportion of breast cancer deaths. From our study findings, it appears that younger patient, single nodule, higher histological tumor grade, earlier lymph node metastasis and more numbers of lymph nodes involved are significantly associated with triple-negative breast cancer. Previous studies [15, 28] have demonstrated that positive lymph node status, lymphovascular invasion and increasing stage (adjuvant vs neoadjuvant) were risk factors for triple-negative breast cancers. Bae et al. [5, 8] discovered that triple-negative invasive tumors affected younger women with a family history of breast cancer and that triple-negative invasive tumors were generally larger in size, of higher histological grade and had a worse prognosis than other breast cancers, owing to their aggressive nature and the absence of effective targeted therapy, which are consistent with ours.
Conventional US is an important method for the detection and characterization of breast masses in the routine examination of breast disease and is established as the first-line guidance process for percutaneous biopsy. Therefore accurate US diagnosis of breast lesions is important for the patients. The researches of Choi et al. [10] presented that triple-negative breast cancer has its unique biological behavior, many triple-negative breast cancers may simulate the benign lesions compared to the ER-positive/PR-positive/HER2-negative breast cancer and might be misinterpreted as the benign. Several additional studies [26, 29] had shown that triple-negative tumors often manifest as circumscribed, benign-looking lesions with an homogeneous internal echo, although the exact reason for this association is not yet fully understood. Our study finding indicates that among all the characteristics the increasing tumor size and the regular shape on conventional US are significantly associated with the triple-negative breast cancers. We also found the internal echo may have corresponding tendencies, but it did not reach a level of statistical significance, which were partly consistent with the previous study. Anders et al. [2, 22] have described factors such as the nuclear grade, tumor circumscription, inflammatory cell reaction, intraductal growth pattern and tubule formation, and have concluded that HR negativity implies an increased proliferation rate, which may explain the larger size of triple-negative breast cancers.
With the development of US techniques, as a noninvasive technology, ARFI allows quantitative and the semiquantitative measurement of the stiffness of lesions in the form of SWV values [11, 20]. Different disease subgroups may have different levels of stiffness, which can express different elasticity patterns. In our study, it has been shown that the highest VTI score, a poorly defined VTI boundary and an SWV ≥3.51 m/s are statistically significant in the differentiation of triple-negative breast cancer from ER-positive/PR-positive/HER2-negative breast cancer. Similar to our results, Kojima et al. [17] reported that 88% of triple-negative breast cancers appeared as hard masses, with elasticity scores of 4 or 5. Boisserie-Lacroix et al. [7] reported quantitative SWV results of 17 triple-negative cases that showed relatively high mean elasticity values ranging from 50 to 232 kPa in the perilesional area. Wojcinski et al. [30] considered that the lack of expression of ER, PR and HER2 results in a genetic mutation, which may tend to exert stronger desmoplastic effects on peritumoral tissues. The stiffness of the peritumoral tissues were affected, meaning that the VTI boundary appeared poorly defined. The numbers of mitoses increased, reflecting enhanced cellularity and an excessive desmoplastic reaction, therefore architectural distortions occurred and a higher mean stiffness showed on a macroscopic level.
Triple-negative breast cancer accompanied by lymphatic metastasis may indicate the poorer prognosis [4]. When we came to analyze the ARFI findings in patients with triple-negative breast cancer and lymphatic metastasis, we found that the VTI score and the SWV value were also related to metastasis in triple-negative tumors, although the boundary on VTI was not significant. It indicated that in triple-negative tumors with a higher VTI score and larger SWV value may be an indicator of a higher risk of lymphatic metastasis. We have learned from previous studies that increased stiffness is associated with nodal metastases [14, 33], but few large-scale investigations have looked at the which ARFI findings correlate with lymphatic metastasis in patients with triple-negative breast cancer. As shown in many studies, triple-negative breast cancers are highly vascular and show lymphatic invasion [2, 5], which may contribute to earlier and more lymphatic metastasis; Researches of Sarvazyan, Garra et al. also have made the assumption that cancer cells in the fibrous stroma infiltrate the lesion caused by nearby construction activity, thereby reducing adhesion between the cells and leading more readily to lymphatic metastasis [23]. however, these assumptions still need further validation.
There are also some limitations in our study. First, in our study, a result of X.XX was recorded as 8.4 m/sec in a solid portion and 0 m/sec in a cystic lesion, as in the previous study from Xu et al. [9, 32]. Handling the data in this manner can partly avoid selection bias, but may ultimately lead to a higher mean SWV value, meaning that an information bias appears. Second, we did not assess interobserver or intraobserver variability with regard to performing elastography and interpreting the data. Subjectivity may exist in the observers, particularly in the evaluation of the VTI and this will need to be evaluated in further studies. Finally, the performance of ARFI also has its limitations, as the findings can depend on many factors, including breast size, breast density, lesion depth, and the proximity of a lesion to the nipple, making it difficult to achieve a consistent optimal image quality in all cases. Furthermore, during performance of this test in our study, we noted that lesions in the different sections may show different elasticity characteristics and further research needs to be done to explain this phenomenon.
Conclusion
Conventional US combined with acoustic radiation force impulse (ARFI) elastography may be able to predict triple-negative breast cancer. The triple-negative breast cancer has a higher SWV value and a higher VTI score, which may indicate a high probability of lymph node metastasis and may indicate a poorer prognosis for the patient. Thus, the tecnique can provide much useful information for the clinical treatment. It would be meaningful for the patients with triple-negative breast cancer to improve the long-term survival rate by earlier clinical intervention.
Footnotes
Acknowledgments
This work was supported by National Natural Science Foundation of China (81471673) and the Research Project of Science and Technology Committee of Shanghai Municipality (124119a3201).