
Abstract
Introduction
Coverage of extensive tissue defects and recovery of both body shape and function often requires sophisticated surgical treatment. Ongoing technical ameliorations as well as improvements in perioperative management and treatment options have enabled today’s plastic surgeon to put a new spin on established concepts in reconstructive surgery [1]. Free surgical flaps have evolved as a reliable and safe tool in the armamentarium of plastic surgery and offer a cornucopia of reconstructive possibilities [2, 3]. However, there are still unsolved problems like partial tissue necrosis or even complete flap loss that impose a serious burden on both patients and physicians [4].
In the literature, complete flap loss is reported to occur in up to 25 percent, or even 36 percent for partial flap loss, especially in presence of comorbidities [5, 6]. Intraoperatively and during the postoperative period flaps are exposed to several risks particularly concerning perfusion. Besides problems affecting the “macro”-vasculature (e.g. thrombosis of the pedicle) with impendence for total flap necrosis, impaired microcirculation may represent a key mechanism in the etiology of partial flap loss [7, 8]. During free flap transfer, transplanted tissues are separated from their original vascular bed and exposed to a phase of complete ischemia after dissection of the pedicle. Lasting ischemia causes the accumulation of metabolic products, which triggers an inflammatory response with consecutive necrosis and disorders in microcirculation. Inflammation is even more potentiated by the restoration of blood flow, resulting in a phenomenon known as ischemia/reperfusion-injury (IR), further deteriorating perfusion and increasing the resulting tissue damage [7, 9–12].
In the past decades different groups have focused on the implementation of strategies against tissue damage caused by prolonged ischemia and IR in the field of plastic surgery. Despite encouraging approaches these techniques did not find their way into broad clinical application. This might be due to several limitations like invasiveness, the need for expensive additional devices or the application of drugs [13–17].
Remote Ischemic Conditioning (RIC) is the application of short, non-damaging periods of ischemia to an isolated vascular territory resulting in a systemic response. This response renders tissues more resilient against hypoxia and IR by anti-inflammatory modes of action and an increase in microcirculation [18–21]. RIC has been shown to protect free surgical flaps in rodent models and was just recently successfully applied in patients undergoing pedicled and free surgical flaps transfer [22]. Application of RIC in the postoperative period resulted in significantly higher blood flow and an improved tissue oxygen saturation of the flaps [23].
The beneficial effect of RIC on human cutaneous microcirculation was first described by Kraemer et al. in 2011 [24]. For the RIC stimulus, three cycles of five minutes ischemia of the upper arm each followed by a phase of ten minutes of reperfusion were applied. In a previous study we were able to confirm their findings and also examined the influence of the chosen extremity, respectively the amount of ischemic tissue, on the conditioning stimulus and its effect on microcirculation [25]. In absence of an evidence based conditioning algorithm we used a RIC protocol as published by Kraemer et al. in our former studies. In fact only a very small number of available studies concerning RIC address this essential requirement, neither with regard to microcirculation nor in human subjects [18, 26]. For this reason the aim of this study was to compare differently configured RIC protocols with respect to their effect on cutaneous microcirculation in humans.
Material and methods
Our study was approved by the local ethics committee of the Ruhr-University Bochum (registration number 15–5223, 25.02.2015) and carried out in accordance to the Declaration of Helsinki. All actions were conducted at the BG University Hospital Bergmannsheil Bochum.
All 60 recruited young healthy volunteers were non-smokers, without a history of chronic illnesses or current medication. After written informed consent was obtained, general characteristics were documented and participants were randomized into one of the four study groups (Fig. 1). In each group the conditioning protocol consists of three cycles of ischemia-intervals with different duration (group I: 1 sec, group II: 1 min, group III: 5 min and group IV: 10 min) followed by consistent reperfusion-intervals for a period of ten minutes. Subjects were placed in a supine position in a temperature controlled room (22° Celcius) without direct light exposure. Participants were instructed to restrict all unnecessary movements during the phase of examination. To avoid any interference withthe conditioning protocols blood pressure measurements were performed at the end of the examination. All measurements were conducted by the same investigator.

Tested RIC protocols. BL = Baseline measurement, I = Ischemia, R = Re-perfusion.
Microcirculatory parameters (blood flow, postcapillary tissue oxygen saturation and relative hemoglobin content) were acquired at the anterior lateral thigh (the donor site for the ALT flap) via laser doppler combined spectroscopy (O2C-Device). Two probes with a different penetration depth (1-2 mm, 7-8 mm) were used for continuous assessment of local cutaneous perfusion dynamics. For assessment of the individual baseline, measurements began 15 minutes before RIC was started.
The RIC stimulus was applied with an inflatable surgical tourniquet, placed on the proximal upper extremity. Inflation pressures of 250 mmHg were used to achieve complete ischemia of the arm. Sufficient ischemia was verified by palpation and obliteration of signals from a pencil doppler probe over the radial artery. Reperfusion was achieved by deflation of the tourniquet.
Statistical analysis was carried out using Microsoft Excel 2007 and IBM SPSS 22. Confidence interval analysis was performed to check for significant variance of general characteristics between groups. For correction of short-term artifacts of continuous microcirculation measurements (one data point per second) these data were separated into corresponding intervals (baseline, ischemia, reperfusion) and regression analysis was performed to create a corrected slope for either the complete or partial interval (not more than five minutes). Relative increase versus baseline measurements was calculated for all parameters. Statistical significance was determined by the confidence interval method and Welch’s t-test was used for comparison between groups. Data is shown as mean and 95 percent confidence interval.
In general characteristics there were no significant differences between groups (p > 0.05). The mean age of all participants was 25.38 years (22–31 years) and mean BMI was 22.9 kg/m2 (16.87–36.23 kg/m2). 27 female and 33 male subjects were examined. See Table 1 for a complete overview.
General characteristics of tested groups, CI = Confidence Interval, m/f = male/female
General characteristics of tested groups, CI = Confidence Interval, m/f = male/female
Blood flow (BF) vs. baseline was significantly (p < 0.05) improved in superficial as well as in deep layers in all groups. In group I there was an increase of +14% (CI: 1.03–1.28) for the superficial (sf) and +25% (CI: 1.09–1.42) deep (dp) measurements. Group II showed an increase of +41% (CI: 1.10–1.72) sf and +30% (CI: 1.17–1.44) dp. In group III increase was +38% (CI: 1.09–1.67) sf and +22% (CI: 1.08–1.36) dp. In group IV there was an increase of +102% (CI: 1.59–2.46) sp and +88% (CI: 1.58–2.18) dp. Comparison between groups confirmed that improvement of BF was significantly more distinct in group IV vs. group I, II and III for superficial as well as deep measurements (p < 0.05) (Fig. 2).

Relative changes of superficial and deep blood flow (-fold increase), BL = Baseline, *marks significant increase against baseline (p < 0.05), †marks significant difference between groups (p < 0.05).
Postcapillary tissue oxygen saturation (StO2) in superficial layers was significantly (p < 0.05) increased in groups III and IV (+8% CI: 1.04–1.12 and +21% CI: 1.14–1.29) as well as in deep layers in groups I and 4 (+7% CI: 1.03–1.12 and +12% CI: 1.04–1.20).
Increase of StO2 was significantly higher in group IV vs. group I, II and III for superficial measurements (p < 0.05) (Fig. 3).
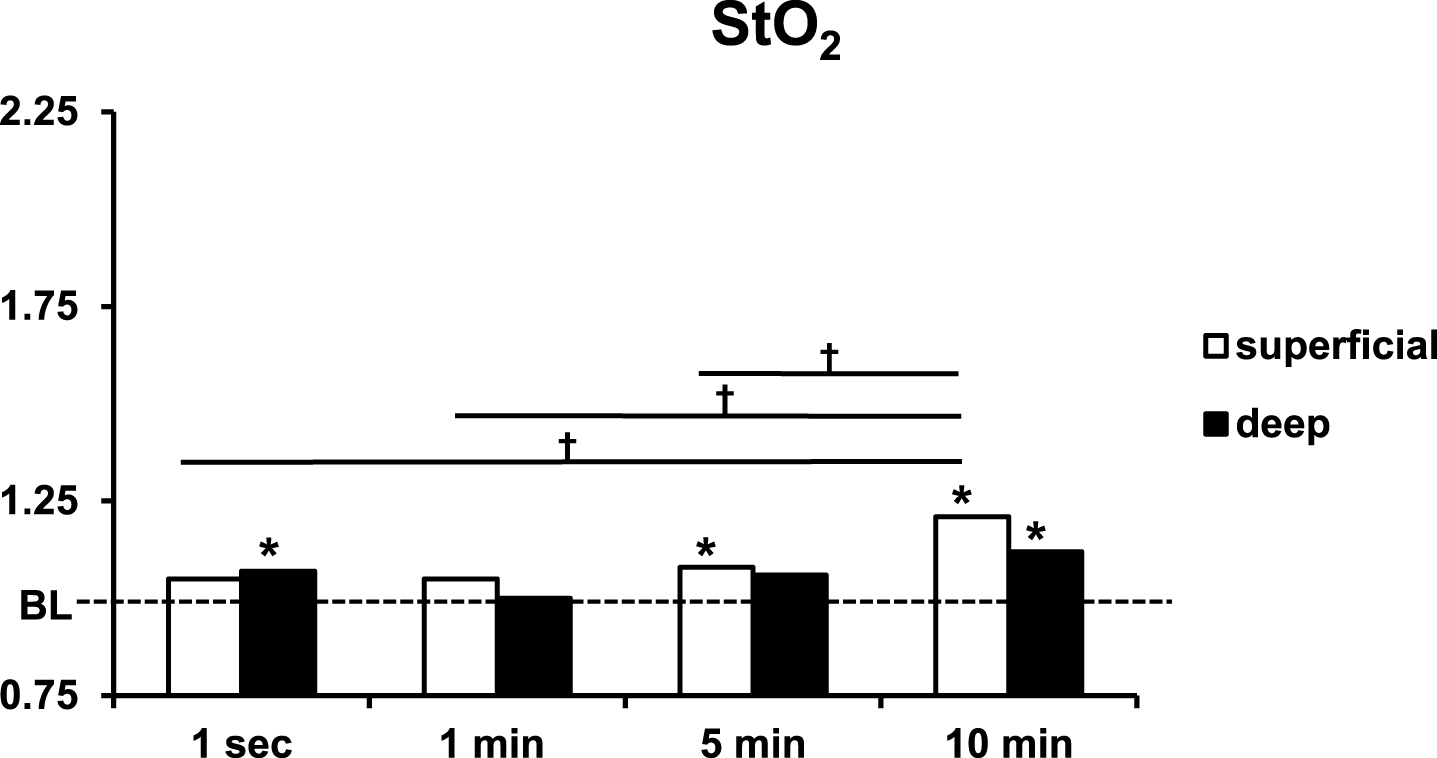
Relative changes of superficial and deep tissue oxygen saturation (-fold increase), BL = Baseline, *marks significant increase against baseline (p < 0.05), †marks significant difference between groups (p < 0.05).
Superficial relative hemoglobin content increased significantly in all groups (+4% CI: 1.03–1.06, +6% 1.03–1.09, +9% 1.05–1.12 and +9% CI: 1.07–1.11). In addition there was a significant increase for the deep measurement in group IV (+19% CI: 1.03–1.35). Comparison between groups showed a significantly more pronounced increase in superficial relative hemoglobin content for group IV vs. group I (Fig. 4).
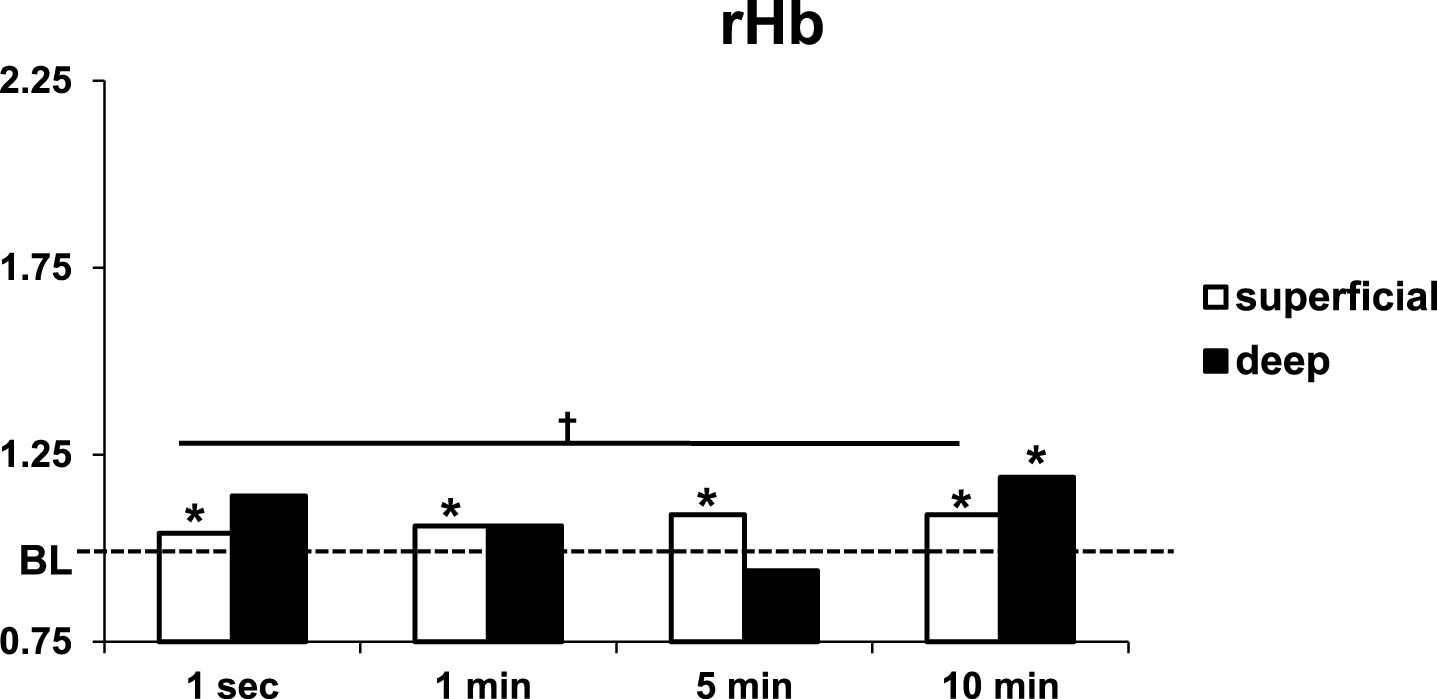
Relative changes of superficial and deep relative hemoglobin content (-fold increase), BL = Baseline, *marks significant increase against baseline (p < 0.05), †marks significant difference between groups (p < 0.05).
Table 2 gives a complete overview of all measured changes.
Complete overview of microcirculatory changes, BL = Baseline measurement, Δ vs. BL = relative changes againstbaseline measurements, CI = Confidence Interval, n.s. = not significant
Protection of compromised tissues against the consequences of ischemia and IR is the designated target of RIC strategies [18, 27]. Although in past years there has been great effort in developing the capabilities of RIC in many fields, particularly concerning cardioprotection, little attention has been paid for the promising opportunities that RIC offers to plastic surgeons [18, 28–30] It has been shown that RIC was capable of protecting surgical flaps against ischemia and IR in rodent models, but todays clinical transfer is still pending [4, 29]. Besides those findings, Kraemer et al. were the first to describe the beneficial effect of RIC on microcirculation in human subjects when they reported significantly increased cutaneous blood flow and tissue oxygen saturation at the ALT donor site after application of a RIC protocol [24].
In a clinical trial Kneser et al. recently showed the importance of sufficient blood flow for flap vitality, especially in the boundary zones. Using the same device as used in our studies, they reported that reduced blood flow over the tip of surgical flaps was associated with local necrosis [8]. This is of great interest in the context of tissue conditioning and RIC, especially RIC was just recently transferred into clinical application in patients with surgical flaps and significantly increased blood flow [23].
Currently, there is no comprehensive explanation for the mechanistic background of RIC and no evidence-based consent on the optimal RIC protocol. The triggering and transmission of the stimulus as well as target effects are objects of ongoing research [18, 31–34]. For a more profound understanding of RIC and its influencing variables, our present study aimed for the determination of the optimal ischemia length for RIC of cutaneous microcirculation.
In their rodent models Küntscher et al. found that protection of surgical flaps trough RIC most likely depends on the higher availability of NO through activation of NO-synthesis enzyme complexes [35–37]. Specific blocking of those endogenous enzyme complexes by L-NAME resulted in abrogation of protective effect of RIC on the examined tissues [36, 37]. Through interaction with the vascular endothelium, higher NO values can lead to increased blood flow, thus higher hemoglobin content and therefore higher oxygen availability with consecutive increase of tissue oxygen saturation [38]. Okorie et al. reported a significant increase of flow mediated dilatation in the radial artery as a response to the application of RIC in healthy human subjects [39]. That is in line with our measured data, which show a significant increase of perfusion in the examined area. Higher values of superficial measurements most likely depend on technical measurements properties and therefore our way of statistical analysis. We suppose that perfusion is generally higher in deeper than in superficial dermal layers under normal conditions [40]. Thus changes of perfusion versus baseline values through RIC would appear more pronounced in the superficial measurements. Furthermore, latest research by Lambert et al. confirms that RIC improves the NO availability during IR in human subjects. Beyond that, the authors stated that besides prevention of reduced NO availability and decrease of erythrocytic oxidative stress, RIC attenuates ischemia induced sympathetic activation [41]. In addition to numerous studies from the field of cardio- or renal protection, this illustrates todays view of mediation of the protective RIC effects: a multidimensional interaction of humoral as well as neuronal pathways and even changes in gene expression [31, 42]. Although signaling cascades in the target organ may depend on exclusive mechanisms which are not generally applicable between different tissues, signal transmission from the conditioning site to the target organ is basically equivalent [43]. Beneath a systemic response to RIC which involves gene alterations that are quite likely the cause of a second phase of protection, initiating 24 hours after the stimulus there is on the one hand a humoral and on the other hand a neuronal transmission of the triggered signal which are responsible for the acute effects of RIC [18, 27]. Loss of the protective effects after complete dissection of nerval connections between the conditioning site and the target organ clearly indicates the involvement of intact nerve fibers [44, 45]. RIC proteome analysis revealed numerous alterations in plasma composition as potentially contributing factors in the mechanism of signal transmission and execution [46]. With that said it seems comprehensible that protection from RIC was shown to be transferable among organisms via plasma donation, thus indicating the importance of humoral mediators [47, 48]. In a current study concerning cardioprotection through RIC Pickard et al. stated that interaction between blood-borne humoral factors and the nervous system belongs on activation of the vagus nerve, which therefore may act as an important mediator [49, 50]. In the context of RIC induced improvement of human cutaneous microcirculation none of those profound mechanistic studies has yet been performed. According to the work of Küntscher et al. and including our former results we hypothesise that improved microcirculation via RIC depends on humoral factors, most likely NO, at least in the terminal signaling cascade and also target effects. In contrast, triggering of the signal seems to involve a greater amount of sensory nerve activation than release of humoral factors. In a previous study, the effects on cutaneous microcirculation were significantly lower in subjects who received the conditioning on the lower extremity instead of the upper extremity although the amount of ischemic tissue was three times greater [25]. Then, we supposed this was due to the greater amount of activation of sensory or autonomous nerve fibers, instead of higher concentrations of humoral factors released by a greater mass of ischemic tissue, for triggering of the signal. Our present findings are in line with those considerations, since even a conditioning protocol with only three cycles of one second of ischemia caused a significant increase of both superficial and deep perfusion in the examined area. This is suitable to the results of a study by Redington et al. who illustrated that a similar degree of tissue protection as enabled through RIC can be achieved by direct activation of remote sensory nerves via either electric stimulation or topical application of capsaicin [44]. However our current measurements clearly show much more pronounced effects in the groups with longer ischemia intervals during the conditioning. Especially group four with three cycles of ten minutes of ischemia provides significant better results in all measured parameters when compared to the other groups. These findings match the published data from Zahir et al. who demonstrated that ischemic conditioning with ten minutes cycles of ischemia is superior to five minutes cycles [51]. Despite instead of RIC they performed local ischemic conditioning in a rodent flap model and attributed the advantages to an also longer phase of re-perfusion which they thought to be necessary to develop protection between the ischemic cycles. Including their conclusion we hypothesize that beneath a certain proportion of initial sensory nerve activation, as represented by study group one, the triggering of changes in cutaneous microcirculation via RIC is exponentiated by the length of ischemia cycles in a dose dependent manner. Whether this depends on the continuous excitation of local sensory nerves through the pressure of the inflated tourniquet or the co-stimulation of mediators released through the ischemic period remains uncertain. In our opinion the second explanation is more likely, since there is a habitation process during repetitive nerve stimulation that may diminish the signal [52].
To our knowledge this is the first study addressing the influence of differently configured protocols of RIC on microcirculation in humans. All of our subjects were young healthy non-smokers without any history of chronic or acute diseases or intake of medication as such our study excludes main influencing factors that are supposed to compound clinical transfer of RIC in recent studies [53–55]. Our findings could have been influenced by the relatively small size of the examined groups. Furthermore the proceeded way of statistical analysis with emphasis on changes versus baseline values may limit the potential of the collected data. However we used this approach as a result of the fact that blood flow and relative hemoglobin content are collected as arbitrary units and therefore their lack of direct comparability. Although not absolutely necessary for tissue oxygen saturation values, we decided to proceed as same as with the two other parameters for homogeneity of the presented results. Due to the lack of a feasible number of publications concerning effects of RIC on cutaneous microcirculation, classification of our results with regard to several details is highly hypothetical. Further research is warranted to examine the influence of the number of applied cycles as well as the duration of measured changes. This will allow for a better understanding of RIC induced improvements of cutaneous microcirculation in humans, thus providing a solid basis for broad clinical employment.
Conclusion
RIC is a safe, non-invasive technique to improve BF and StO2 of superficial and deep dermal layers in healthy subjects. A conditioning protocol containing three cycles of ten minutes of ischemia followed by ten minutes of reperfusion is superior to conditioning protocols consisting of shorter ischemia-intervals. Further research is required to reveal the impact of the number of applied cycles and the duration of assessed changes in microcirculation. In combination with our current findings this will back up the transfer of RIC strategies into clinical application.
Disclaimer
None of the authors has a financial interest in any of the products, devices, or drugs mentioned in this manuscript.
Footnotes
Acknowledgments
We thank the Georgius Agricola Foundation Ruhr for supporting J.K. via a grant. J.K. also received a grant from the Ruhr-University Bochum via the FoRUM-program. Both grants did not influence the design or execution of this study in any way.