
Abstract
The aim of the present study was to test the effects of hydroxyurea (HU) therapy on clinical, hematological and hemorheological parameters in adult patients with sickle cell anemia (SCA). Hematological and hemorheological parameters were measured in 28 SCA patients before HU therapy (i.e., baseline) and at 6, 12 and 24 months of treatment. RBC deformability was determined by ektacytometry at 30 Pa. RBC aggregation properties were investigated by light-backscatter method. Blood viscosity was measured at 225 s–1 by a cone-plate viscometer. The rates of vaso-occlusive crises and acute chest syndrome were lower at 1 and 2 years of HU therapy compared to baseline. The proportion of patients with leg ulcers tended to decrease after 2 years of treatment. Hemoglobin oxygen saturation improved with HU therapy. HU therapy induced a decrease of platelet and white blood cell counts and a rise in fetal hemoglobin level and mean cell volume. While hemoglobin concentrations increased under HU, blood viscosity remained unchanged all along the study. RBC deformability increased over baseline values at 6 months of HU therapy and continued to rise until the end of the follow-up period. In conclusion, the improvement in RBC deformability probably compensates the increase of hemoglobin on blood viscosity and participates to the improvement of the clinical status of patients.
Introduction
The presence of sickle hemoglobin (HbS) in red blood cells (RBC) of patients with sickle cell anemia (SCA) is at the origin of their rheological abnormalities. When oxygen is delivered to tissues, HbS polymerization causes the mechanical distortion of RBC. Sickled RBC are rigid, fragile and do not easily flow through the microcirculation, leading to frequent vaso-occlusive crises (VOC) in affected patients [3, 9]. Recurrent HbS polymerization is responsible for numerous RBC and systemic physiological abnormalities with variable phenotypic severity [13]. Abnormal blood rheology has been shown to modulate clinical severity and to be involved in several complications of SCA [3, 25]. It has been clearly established that SCA children and adults with increased blood viscosity are at risk for frequent VOC [8, 21].
Hydroxyurea (HU) therapy improves the clinical course of both children and adults with SCA, by reducing the frequency of VOC and acute chest syndrome (ACS) and the number of hospitalizations per year [7, 30]. Beneficial effects of HU on biological parameters include increase of fetal hemoglobin (HbF) and hemoglobin (Hb) levels, RBC deformability and mean cell volume (MCV) [2, 30]. In addition, HU therapy decreases white blood cell (WBC), reticulocyte (RET) and platelet (PLT) counts, hemolytic rate, as well as RET and neutrophils adhesiveness [4, 30]. Nevertheless, because HU therapy increases Hb levels, it has sometimes been postulated that some patients could develop blood hyperviscosity which could slightly attenuate the clinical benefits of this therapy [30]. We recently reported that 1 year of HU therapy did not change blood viscosity despite a rise in Hb in SCA patients [17]. However, it is unknown whether blood viscosity still remained unchanged after prolonged use of HU. The aim of the present study was to evaluate the blood rheological changes that could occur after 2 years of HU therapy in SCA patients. Evaluating the long term effects of HU therapy on blood viscosity is of particular importance, before its use can be extended more widely to patients with cerebral vasculopathy or other genotypes, such as sickle cell hemoglobin-C disease (SC), a sickle cell syndrome marked by higher blood viscosity than SCA patients at steady-state [22, 28].
Material and methods
Patients
Twenty-eight adult SCA patients (37.0±11.6 yrs, 60.2±10.7 kg, 171.5±11.0 cm; 15 males/13 females; 50% with α-thalassemia) regularly followed by the Sickle Cell Center of Pointe-á-Pitre (Academic Hospital, Guadeloupe) were included in this study. At the beginning of the HU therapy all patients were at steady state, i.e., no blood transfusions in the previous three months and absence of acute episodes (infection, VOC, ACS, stroke, priapism) at least one month before inclusion into the study. Frequent hospitalized VOC (n = 14) and/or at least one ACS (n = 10) event in the preceding year were the main reasons to propose HU therapy to these patients. ACS and VOC were defined as previously described [11, 16]. For the other patients, HU therapy has been recommended because of frequent ambulatory sub-clinical VOC and persistent low hemoglobin levels. None of the participants had renal insufficiency, hepatic insufficiency or human immunodeficiency virus infection. Routine examination before starting HU therapy included the measurements of blood pressures (BP), mean hemoglobin saturation (by pulse oxymetry, SpO2), heart rate (HR), collection of information regarding the presence of leg ulcers and frequencies of priapism. Patients were also questioned about chronic asthenia and the incidence of dyspnea during daily activities. The same parameters, as well as occurrence of the above complications (VOC, ACS), were prospectively recorded for 1 year and 2 years after the initiation of HU therapy. Before HU therapy (i.e., baseline) and at 6, 12 and 24 months of treatment, blood was collected for biochemical, hematological and hemorheological measurements. The study was performed in accordance with the Declaration of Helsinki, was approved by the IRB of the Academic Hospital of Pointe á Pitre (DRCI-CHUPAP 230514, Guadeloupe) and written informed consent was obtained from all patients.
Laboratory methods
Diagnosis of SCA was made by isoelectrofocusing (Multiphor II™ System, GE HEALTH CARE, Buck, UK), and cation-exchange high performance liquid chromatography (VARIANT™, Bio-Rad Laboratories, Hercules, CA, USA). Solubility test was also performed to confirm the presence of HbS. Genomic DNA was isolated from peripheral blood using standard desalting methods. Polymerase Chain Reaction technology (Gap-PCR) was used to detect 7 common α-thalassemia deletions including -α3.7 and - α4.2 alleles and triplication defects of the α-globin genes [26, 27].
Hematological and biochemical parameters
Hb concentration, hematocrit (Hct), MCV, mean corpuscular hemoglobin concentration (MCHC), RET, RBC, PLT, WBC and neutrophils counts were determined using a hematology analyzer (Max M-Retic, Coulter, USA). Lactate dehydrogenase (LDH) level was measured by standard biochemical methods at baseline, 1 year and 2 years of treatment.
Hemorheological parameters
All hemorheological measurements were carried out within 4 hours of the venipuncture to avoid blood rheological alterations, and after complete oxygenation of the blood [5]. Blood viscosity was determined at native Hct, at 25°C, and at a shear rate of 225 s–1 using a cone/plate viscometer (Brookfield DVII+ with CPE40 spindle, Brookfield Engineering Labs, Natick, MA). RBC deformability was measured at 37°C and 30 Pa by laser diffraction analysis (ecktacytometry), using the Laser-assisted Optical Rotational Cell Analyzer (LORCA, RR Mechatronics, Hoorn, The Netherlands). The system has been described elsewhere in detail [5]. Briefly, 25 μl of prepared blood suspension was mixed with 5 ml polyvinylpyrrolidone (PVP; viscosity = 30 cP) and sheared into a Couette system made of glass. The diffraction pattern was analysed by the computer to calculate an elongation index reflecting RBC deformability [5]. RBC aggregation was determined at 37°C via syllectometry, (i.e., laser backscatter versus time, using the LORCA) after adjustment of the Hct to 40%. In addition, the RBC disaggregation threshold (i.e., RBC aggregates strength) was determined using a re-iteration procedure [5]. Seven pre-defined shear rates ranging between 7.5 s–1 and 800 s–1 were applied on the RBC suspension to locate the minimal shear rate needed to prevent RBC aggregation.
Statistical analysis
Values are expressed as means±SD. A One-Way Analysis of Variance (ANOVA) with repeated measurement was used to study the physiological, clinical and biological changes occurring with HU therapy. Post-hoc Tukey test was performed to locate the differences. McNemar test was used to test the effects of HU on different clinical parameters after 2 years of treatment. Pearson correlation was performed to test the associations between different variables. Significance level was defined as p < 0.05. Analyses were conducted using SPSS (v. 20, IBM SPSS Statistics, Chicago, IL).
Results
Clinical data
Regarding the clinical course of the disease, HU was effective in 25 of the 28 patients after 1 year of treatment (two patients had ACS and one had VOC) and in 27 of the 28 patients after 2 years therapy (only one patient experienced a VOC episode). The number of VOC and ACS events decreased (p < 0.01 and p < 0.05, respectively) from 0.81±1.09 and 0.56±0.98 before treatment, respectively, to 0.16±0.52 and 0 after 1 year treatment and 0.04±0.20 and 0 after 2 years treatment. SpO2 was improved compared to baseline values after 1 year and 2 years of HU therapy. HR was decreased after 2 years of HU therapy compared to baseline (Table 1). Blood pressures did not change with HU (Table 1). HU treatment decreased the proportion of patients with chronic asthenia and dyspnea from 64% and 93% to 0% and 21%, respectively (p < 0.001 for both). The frequency of patients with frequent priapism did not significantly change with HU (18% vs 4% before and after 2 years of therapy, respectively, p = 0.25) but the proportion of patients with leg ulcers tended to decrease (27% vs 13% before and after 2 years of therapy, respectively, p = 0.06).
Routine clinical parameters before, 1 year after and 2 years after HU therapy
Routine clinical parameters before, 1 year after and 2 years after HU therapy
SpO2, hemoglobin saturation; HR, heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure. Different from before treatment: *p < 0.05; **p < 0.01; ***p < 0.001.
Doses of HU were increased progressively and adjusted for each patient, based on the hematological parameters [30]. The mean doses of HU prescribed to the patients in this study are relatively low because some patients had early sign of hemato-toxicity leading physicians to decrease the doses. At 2 years of therapy, patients received 15.7±5.4 mg/kg/days of HU. HbF (Fig. 1A), Hb (Fig. 1B), MCV (Fig. 1C) and RBC deformability (Fig. 1I) increased at 6 months of HU treatment and remained elevated at 1 and 2 years after the beginning of therapy. RBC deformability at 2 years was also higher than at 6 months of HU therapy (Fig. 1I). WBC (Fig. 1D) and PLT (Fig. 1E) counts, LDH level (Fig. 1F) and RET count (data not shown; p < 0.001) were decreased at 6 months, 1 year and 2 years of HU therapy in comparison with baseline. MCHC was decreased after 2 years of HU therapy compared to baseline (data not shown, p < 0.05). RBC aggregates strength decreased below baseline values at 6 months but then the difference between baseline and 1 year/2 years of treatments was not significant (Fig. 1H). Blood viscosity (Fig. 1G) and RBC aggregation (data not shown) did not change with HU therapy.
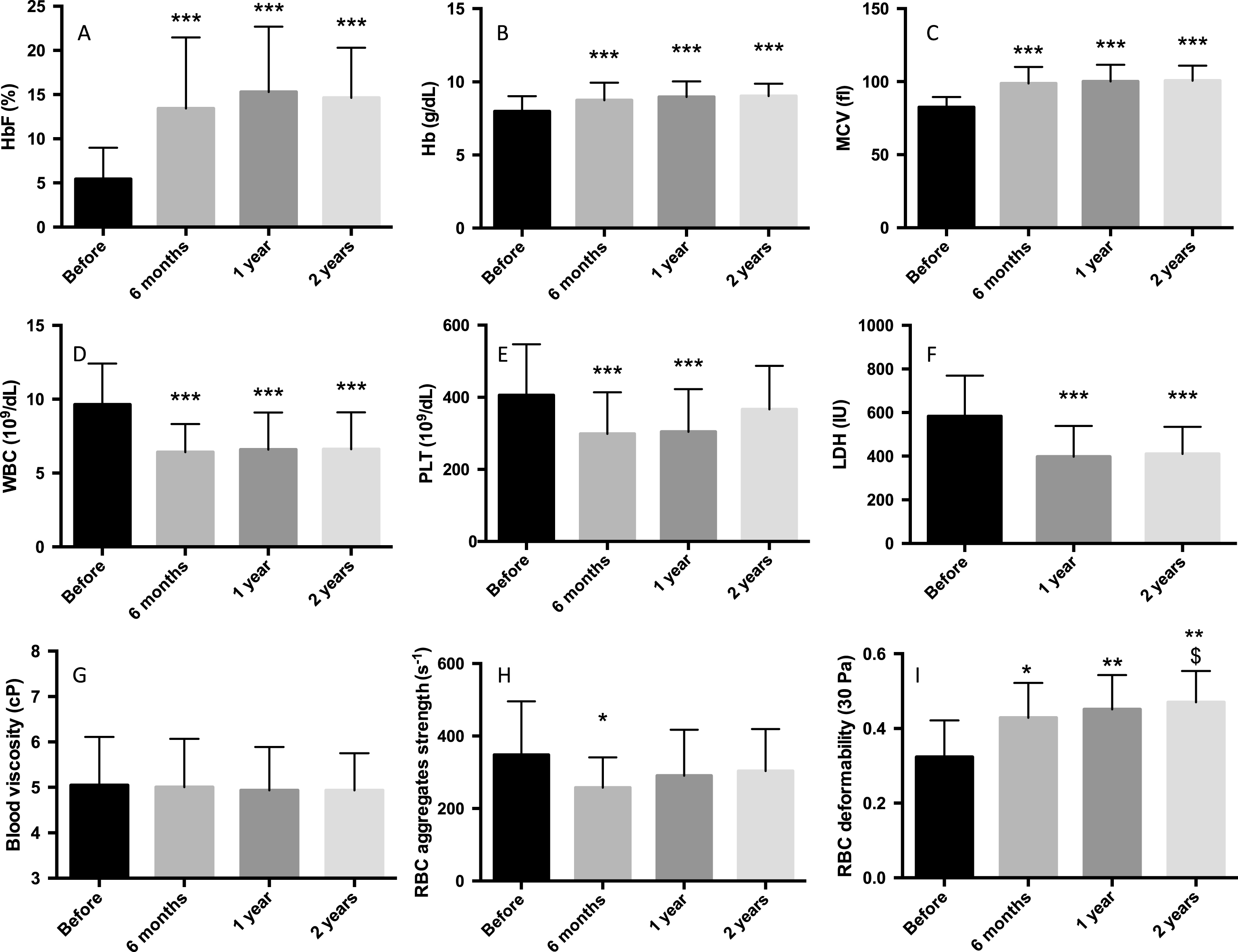
Effects of HU therapy on HbF level (1A), Hb level (1B), MCV (1C), WBC (1D) and PLT (1E) counts, LDH level (1F), blood viscosity (1G), RBC aggregates strength (1H) and RBC deformability (1I). HbF, Fetal hemoglobin; Hb, hemoglobin; MCV, mean cell volume; WBC, white blood cells; PLT, platelet; LDH, lactate dehydrogenase; RBC, red blood cell. Different from before treatment: *p < 0.05; **p < 0.01; ***p < 0.001. Different from 6 months: $p < 0.05.
Since the highest changes in the biological values occurred at 6 months of HU therapy, we calculated the percentages of changes between baseline (i.e., before treatment) and 6 months of treatment. Subsequently, correlations were used to test associations between variables using these percentages of changes. Our results showed positive correlation between the changes in HbF level and RBC deformability (r = 0.46; p < 0.05) and MCV and RBC deformability (r = 0.56; p < 0.01). In addition, the changes in Hb level positively correlated with the changes in RBC deformability (r = 0.55; p < 0.01).
Discussion
Our study demonstrated that 2 years of HU therapy decreases the severity of anemia in SCA patients without any increase in blood viscosity. Enhanced RBC deformability probably limits the consequences of elevation of hemoglobin level on blood viscosity and participates to the clinical improvements observed in the present study.
In agreement with previous studies, HU significantly decreased the rates of hospitalized VOC and ACS in SCA patients who frequently exhibited these complications [7, 30]. In addition, the proportion of patients with leg ulcers tended to decline. High level of white blood cell and platelet counts increase the risk for vaso-occlusive crises, acute chest syndrome and stroke in SCA [1, 20]. In addition, patients with increased hemolytic rate (as indicated by a high lactate dehydrogenase level) would be prone to develop several complications such as leg ulcers [10] or stroke [12]. Reduced hemoglobin oxygen saturation is clearly a significant risk factor for several complications such as stroke [15] and vaso-occlusive crises [14] because it may promote the activation of platelet and endothelial cells [24]. Indeed, the decrease of reticulocyte, white blood cell and platelet counts, as well as the decrease of hemolysis and the increase of Hb level under HU treatment, have most likely participated to the clinical improvements observed in our study [30]. The decrease of anemia severity and the improvement of hemoglobin oxygen saturation have also probably participated to the reduction of the proportion of patients complaining for chronic asthenia (i.e. fatigue) and dyspnea. HU clearly improved patients’ quality of life. Anecdotally, clinical interviews revealed that all patients were able to perform daily activities, such as physical activity or house cleaning, more easily after two years of HU medication than before.
It is now widely recognized that increasing blood viscosity in SCA patients is a significant risk factor of frequent VOC, both in adults [18] and children [8, 21]. Although previous studies suggested that the rise in hemoglobin level under HU therapy could increase blood viscosity in SCA patients [30], our findings clearly demonstrate that blood viscosity remains unchanged over 2 years of HU therapy. This observation confirms preliminary published data showing that blood viscosity did not change after 1 year of HU therapy compared to baseline values [17]. The absence of rise in blood viscosity in SCA patients receiving HU, may be explained by the large improvement of RBC deformability, the decrease of white blood cell count and the slight decrease of the RBC aggregates strength, which compensate for the increase in hemoglobin. The increase in hemoglobin/hematocrit level without any change in blood viscosity probably improved the oxygen transport and delivery to tissues [29]. Improvement of RBC deformability in HU-treated patients is likely due to 1) the increase in HbF level, which decreases the proportion of abnormal HbS inside the RBCs and its ability to polymerize, 2) the decrease of internal viscosity (MCHC) and 3) high hydration status of RBCs, as noted by the increase in MCV (and the decrease in MCHC). As a consequence, RBCs are less fragile and survive longer in the circulation, leading to a reduction of anemia.
In conclusion, we demonstrated that HU therapy improves the hematological profile and RBC rheology in SCA patients, without any deleterious effects on blood viscosity, which may explain why this treatment provides large clinical benefits especially for SCA patients suffering from frequent vaso-occlusive like episodes. Moreover, our findings suggest that the biological effects of HU are at their maximum at 6 months of treatment and then remain stable.
Conflict-of-interest disclosure
No conflict of interest.
Footnotes
Acknowledgments
K.C., X.W. and Y.L. were funded by the Region of Guadeloupe.