
Abstract
There is scarcity of information about the hemorheological pattern in subjects with Monoclonal Gammopathy of Undetermined Significance (MGUS). This preliminary research is focused on the behaviour of whole-blood and plasma viscosity, haematocrit and erythrocyte deformability in the above clinical condition. We enrolled 21 MGUS subjects (10 women and 11 men; mean age 66.4 ± 11.6 years). In fasting venous blood we examined whole-blood and plasma viscosity at high and low shear rates, haematocrit, the ratios between whole-blood viscosity (at high and low shear rate) and haematocrit × 100, the ratio between plasma viscosity at low and high shear rate, and the erythrocyte deformability expressed as elongation index. By comparing normal controls to MGUS subjects a significant increase in whole-blood viscosity at high shear rate and in plasma viscosity at low shear rate were observed. In MGUS subjects the ratios between the high and low shear rate blood viscosity and haematocrit × 100, as well as the ratio between the low and high shear rate plasma viscosity were significantly higher. In MGUS subjects a marked decrease in erythrocyte deformability was also observed. The alteration of the hemorheological profile found in these subjects might be involved in the pathogenesis of thromboembolic events, which occur with a high frequency in MGUS.
Introduction
Monoclonal Gammopathy of Undetermined Significance (MGUS) is defined as the presence of a monoclonal protein (M-protein) at a serum concentration <30 g/L, clonal plasma cells in bone marrow <10%, no end-organ damage and no evidence of B-cell lymphoma or other disease known to produce an M-protein. This process is not considered neoplastic since it does not always progress to overt malignancy.
IgG-MGUS and IgA-MGUS are associated with the presence of clonal plasma cells, and may progress to multiple myeloma (MM), while the presence of a small IgM paraprotein (IgM-MGUS) is associated with a clone of lymphoplasmacytic cells that may progress to a lymphoplasmacytic lymphoma, and/or Waldenstrom’s macroglobulinemia (WM).
MGUS is found in approximately 3% of subjects aged over 50 and in more than 5% of individuals older than 70 years, and is more common in men than women (∼1.5 : 1). No specific cause of MGUS has been identified. It may be associated with connective tissue diseases, peripheral neuropathies, dermatological, endocrine and liver diseases. Obesity and personal history of autoimmune diseases, inflammatory conditions and infections are associated with increased risk of MGUS. Furthermore, occupational studies have demonstrated that exposure to radiation or pesticide seems to be associated with the development of MGUS [4, 41].
Subjects exhibit no symptoms or physical evidences related to MGUS. The typical laboratory and radiographic abnormalities associated with MM are absent. The M-protein is usually discovered unexpectedly on serum protein electrophoresis. Approximately 70% are IgG, 15% IgM, 12% IgA and 3% are biclonal. Up to 20% of MGUS may consist only of an Ig light chain (LC-MGUS) that must be detected with the serum free light chain assay. A reduction of uninvolved Ig is observed in 30–40% of MGUS subjects and monoclonal light chain in urine is near to a third; abnormal karyotypes are rarely detected in MGUS.
The clinical course in most MGUS patients is stable, with no increase in M-protein or other evidence of progression. However, there may be an escalation to an overt MM, amyloidosis (in non-IgM MGUS), WM or other lymphoproliferative disorders (in IgM MGUS). The risk is about 1% per year and persists even after 30 years; thus, MGUS should be considered a pre-neoplastic condition [23, 44].
There are certain characteristics useful to predict the escalation from MGUS to a symptomatic disease: the size of the MGUS clone as determined by bone marrow plasma cell percentage, the M-protein level, the heavy-chain isotype (IgA/IgM >IgG), the light-chain production as determined by abnormal serum free light chain ratio, the presence of Bence Jones proteinuria or the detection of circulating plasma cells or clonal B cells. Furthermore, suppression of non-clonal bone marrow plasma cells, detected by multiparameter flow cytometric analysis, has been identified as a risk factor for the escalation.
Based on available clinical markers, the Mayo Clinic and the Spanish study group established predictive risk models for the escalation from MGUS to MM. The Mayo Clinic model emphasizes the clonal plasma cell burden with monoclonal protein values and skewed free light-chain ratios, whereas the Spanish study group uses multiparametric flow cytometry techniques to identify aberrant plasma cell populations [19].
Outside of clinical trials, there are no current standardized treatment options for MGUS, although since 2010, the International Myeloma Working Group guidelines have suggested risk-stratifying of all subjects with MGUS and differential monitoring of subjects based on their risk category as well as on their life expectancy depending on age and presence of comorbidities [22].
Considering the above data, and according to Castillo [6], MGUS may be considered a benign plasma cell disorder characterized by the presence of monoclonal paraprotein in serum or urine. However, the presence of the paraprotein may alter the whole-blood viscosity (WBV), as it is the case for MM and WM [11, 36]. The alteration of WBV plays a more prominent role in microcirculation than in large vessel hemodynamics. Physiologically, blood flow is influenced by blood velocity, vessel diameter and WBV; the latter is determined by haematocrit (Ht), plasma viscosity (PV), red cell aggregation and deformability. WBV varies in relation with shear rate and several clinical and experimental data have clearly demonstrated that red cell deformability and PV are the main determinants of flow at high shear rate, while red cell aggregation rises to prominence during flow at low shear rate.
To date, only two papers examined the behaviour of the hemorheological pattern in subjects with MGUS. A study [40] was carried out on a group of 87 patients who were affected by plasma cell dyscrasias (PCD), including MM (n = 52), MGUS (n = 30), WM (n = 5). The study examined WBV and PV: 71% of the PCD patients showed PV above the reference limit, and 40% had WBV above the reference limit. Another research paper [7] focused on the erythrocyte aggregation, red cell deformability and microcirculation (Periflux tests) in a group of 8 patients with active MM, 9 MM patients in remission and 7 MGUS subjects. In this study MGUS subjects differed from the two groups of MM patients in erythrocyte aggregation and microcirculatory tests but not in erythrocyte deformability.
The aim of this preliminary study was the evaluation of WBV, PV, Ht and erythrocyte deformability in a group of MGUS subjects.
Subjects
A group of 21 subjects (10 women and 11 men; mean age 66.4 ± 11.6 years) with MGUS were examined. The M-protein was IgG in 18 subjects and IgM in 2; in a subject both monoclonal IgG and IgA were observed. The time interval from the first detection of the M-protein was 41.3 ± 50.2 months. The principal laboratory findings in these MGUS subjects were: Hb (g/dl) 12.94 ± 1.80 (range 10.1–17.1), Red-cell Distribution Width (RDW – %) 13.78 ± 1.26 (range 12.4–17.1), creatinine (mg/dl) 0.95 ± 0.23 (range 0.7–1.4), beta2-microglobulin (μg/ml) 2.954 ± 1.311 (range 0.75–5.68), calcium (mg/dl) 9.409 ± 0.425 (range 8.8–10.1), albumin (g/L) 41.53 ± 3.53 (range 36.8–48.2), IgG (mg/dl) 1656 ± 737.4 (range 771–2872), IgA (mg/dl) 201 ± 205.3 (range 40–805), IgM (mg/dl) 333.7 ± 743.2 (range 21.6–2668), fibrinogen (mg/dl) 267.4 ± 36.12 (range 215–340), M-protein (g/dl) 0.922 ± 0.439 (range 0.150–1.800). The control group included 21 subjects (8 women and 13 men; age range 23–63 years), whose health was assessed through clinical history, physical examination, electrocardiography, routine blood and urine analyses.
Methods
Venous blood samples were collected in the morning by venous puncture from the antecubital vein of fasting subjects and immediately transferred to anticoagulated glass tubes for the evaluation of the following parameters: WBV at the shear rate of 450 sec–1, by using the cone-on-plate viscometer Well-Brookfield 1/2 LVT (Middleboro, MA, USA), at 37°C; WBV at the shear rate of 0.51 sec–1 employing the viscometer Contraves LS30 (proRheo GmbH, Althengstett,Germany), at 37°C; PV at the shear rate of 450 sec–1, by using the cone-on-plate viscosimeter Wells-Brookfield 1/2 LVT, at 37°C; PV at the shear rate of 0.51 sec–1 employing the viscometer Contraves LS30, at 37°C; Ht, obtained by using a micromethod; WBV at 450 sec–1/Ht×100; WBV at 0.51 sec–1/Ht×100; PV at 0.51 sec–1/PV at 450 sec–1; Erythrocyte deformability: to evaluate this parameter, a sample of 30μl of anticoagulated blood was mixed with 2 ml of dextran solution with a viscosity of 24 mPa·s. The measurement was obtained by using the diffractometer Rheodyn SSD of Myrenne, which measures the diffraction pattern of a laser beam passing through erythrocytes suspended in a viscous medium and deformed by a force with defined shear stress. The shear stress employed was 6, 12, 30 and 60 Pa. The erythrocyte deformation was expressed as elongation index (EI) = (l – w/l + w) x100, where l = length and w = width of the erythrocytes.
Statistical analysis
Data were expressed as means ± S.D. The Student’s t test for unpaired data was used to compare normal controls to MGUS subjects. The correlation between WBV and Ht, WBV and PV, WBV and EI in normal controls and MGUS subjects, and between PV and the concentrations of fibrinogen, Ig and M-protein in MGUS subjects was examined using the linear regression.
Results
By comparing normal controls to MGUS subjects, a significant increase in WBV at high shear rate and a marked increase in PV at low shear rate were found (Table 1). Subsequently we studied the correlations between WBV (at high and low shear rates) and Ht in normal controls and in MGUS subjects, which resulted statistically significant (Fig. 1). PV (at high and low shear rate) was not correlated with the concentrations of Ig, M-protein and fibrinogen in MGUS subjects (data not shown). We also evaluated the correlations between high shear rate WBV and high shear rate PV, and between low shear rate WBV and low shear rate PV, both in normal controls and MGUS subjects (Fig. 2). A significant correlation was found, in both groups, only between high shear rate WBV and high shear rate PV. The ratios between high and low shear rate WBV/Ht ×100 and the ratio between PV at low and high shear rate were considered (Table 2). All the three ratios were significantly higher in MGUS subjects in comparison with normal controls. The erythrocyte deformability, expressed as EI, was markedly decreased in MGUS subjects (Table 3). WBV at high and low shear rates was not correlated with EI (data not shown).
Means ± S.D. of the hemorheological determinants in control subjects and MGUS patients
Means ± S.D. of the hemorheological determinants in control subjects and MGUS patients
**p < 0.01; ***p < 0.001 vs Control subjects (student’s t test for unpaired data). WBV = Whole-Blood Viscosity; PV = Plasma Viscosity; Ht = Haematocrit; mPa = milliPascal.
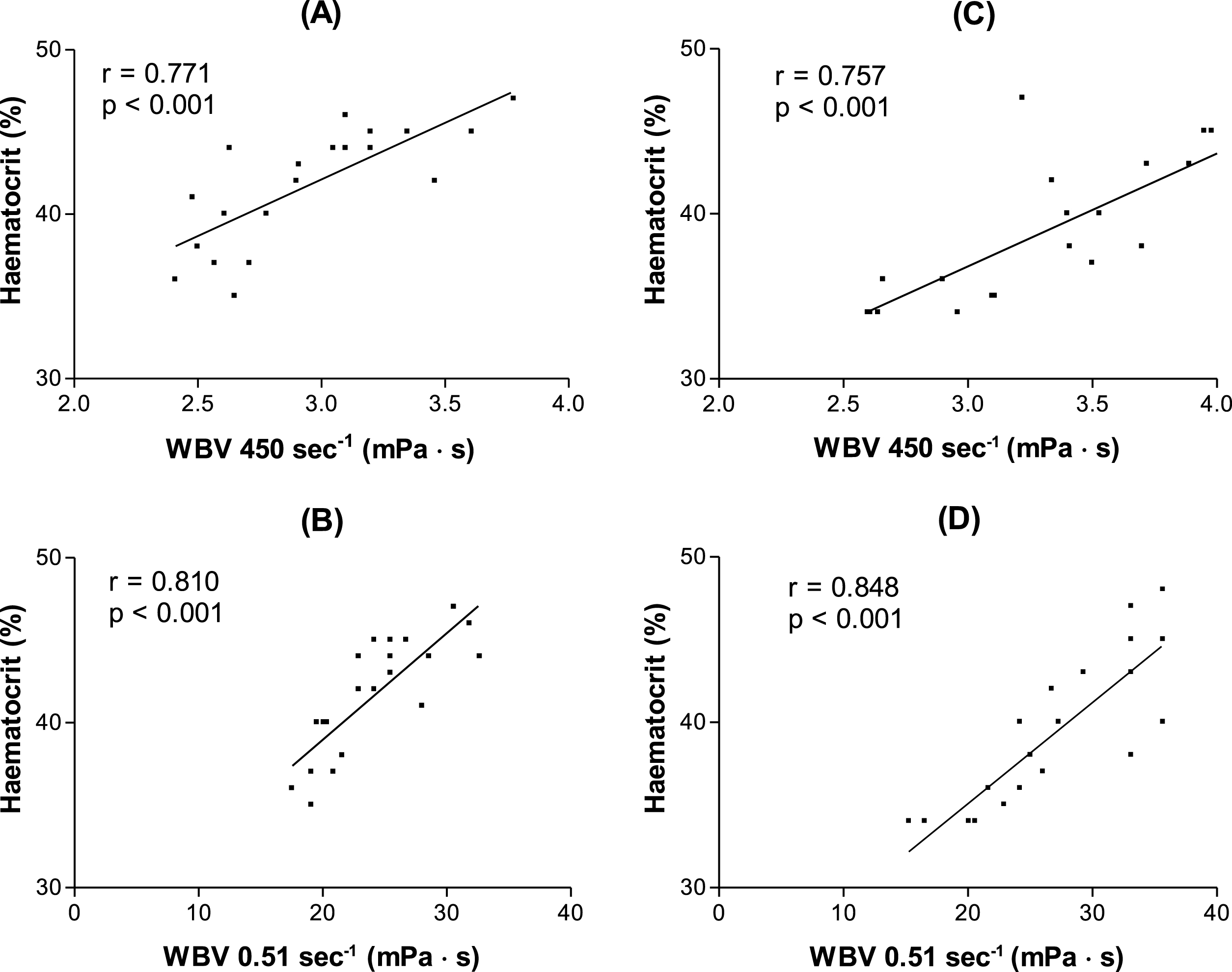
Correlations between whole-blood viscosity (WBV) and haematocrit in control subjects (A-B) and in MGUS patients (C-D).
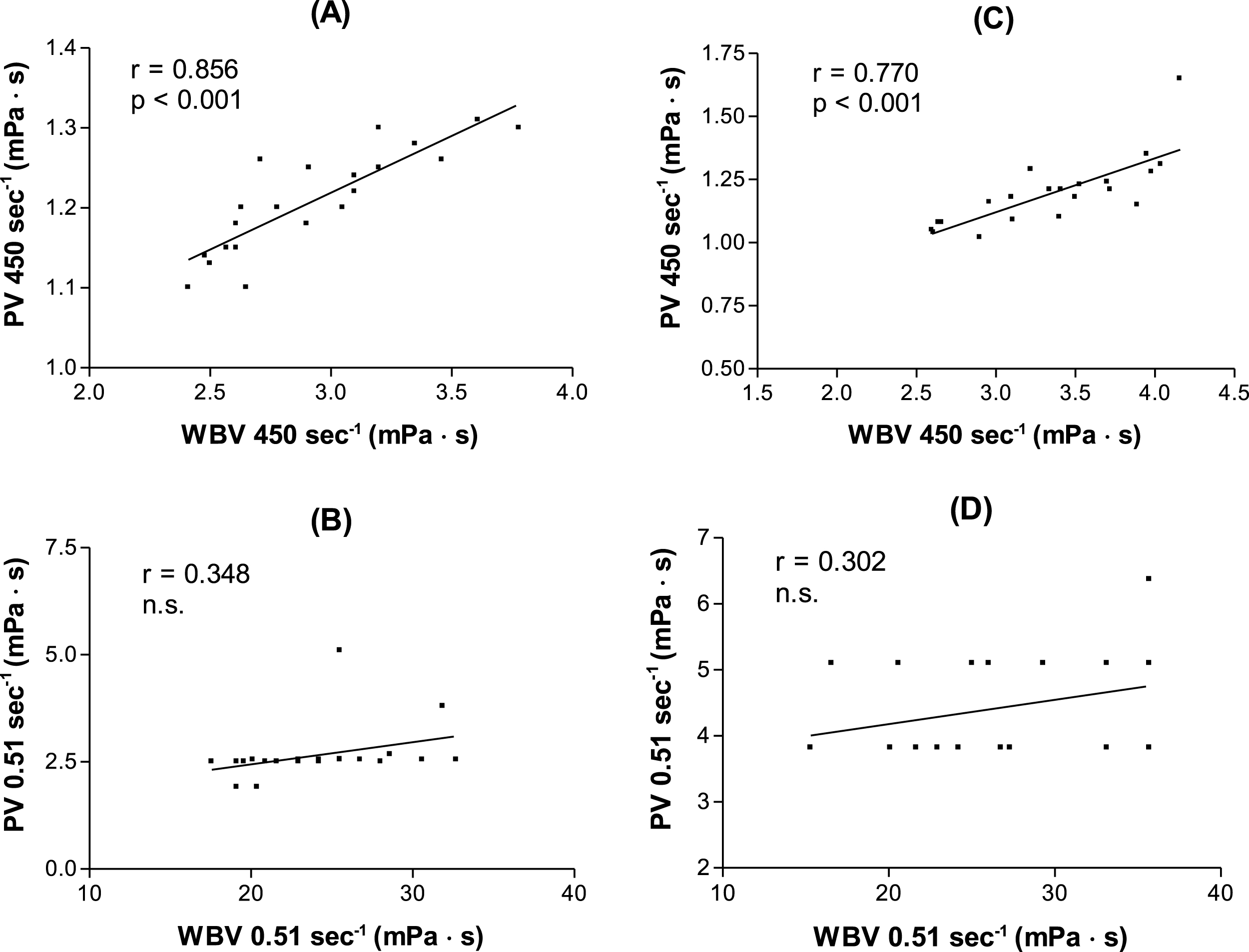
Correlations between whole-blood viscosity (WBV) and plasma viscosity (PV) in control subjects (A-B) and in MGUS patients (C-D).
Means ± S.D. of the hemorheological indexes in control subjects and MGUS patients
**p < 0.01; ***p < 0.001 vs Control subjects (student’s t test for unpaired data). WBV = Whole-Blood Viscosity; PV = Plasma Viscosity; Ht = Haematocrit.
Means ± S.D. of erythrocyte deformability in control subjects and MGUS patients
***p < 0.001 vs Control subjects (student’s t test for unpaired data). EI = Elongation Index.
Our results show an increase of high shear rate WBV and low shear rate PV in MGUS subjects. These findings are different from those observed in MM by our research group (data submitted); in MM patients, in fact, a marked decrease in Ht prevented WBV from being elevated. In MGUS subjects we observed a significant increase in PV at low shear rate, as well as a higher low shear rate PV/high shear rate PV ratio. Since plasma is generally considered a newtonian fluid, its viscosity should not vary at different shear rates. However, the use of rotational viscometers elicits a different behaviour of PV at high and low shear rate respectively; this effect was probably amplified in our study by the use of two different devices. Taking into account the technical conditions in which we performed the measurement, a different behaviour was evident between MGUS patients and control subjects, and the properties of the M-protein are likely to be responsible for that.
PV seems to be an independent risk factor especially for cardiovascular diseases [5, 34], and in MGUS the risk of venous thromboembolic events is increased [14, 45]. Some studies focused on the coagulation profile present in this clinical condition [9, 10], but the possibility that the alteration of the hemorheological profile contributes to the pathogenesis of venous thromboembolic events in MGUS subjects cannot be ruled out. In fact, there has been much research on the role of hemorheological alterations in arterial and venous thrombosis [2, 42]. An unexpected finding of this preliminary study was the behaviour of the erythrocyte deformability in the MGUS subjects. The factors able to reduce this hemorheological parameter are an alteration of the surface/volume ratio, an increased cytosolic viscosity and an impairment of the red cell membrane dynamic properties, referable especially to an alteration of membrane lipids and proteins. In MGUS subjects no abnormalities in the erythrocyte membrane lipid profile, plasma lipid composition or fatty acid metabolism are known, whereas such alterations have been observed in patients with MM [16, 43].
The only abnormality of the erythrocyte membrane noted in MGUS regards the membrane proteins and consists in the presence of a paroxysmal nocturnal hemoglobinuria-like (PNH-like) defect in some MGUS subjects [12, 33]. This defect is characterized by an altered synthesis of glycosilphosphatidylinositol, which is essential for the binding of some surface proteins, such as CD55 and CD59, able to protect the red blood cells from intravascular lysis. To date PNH-like clones have been observed in several haematological disorders such as aplastic anaemia, myelodysplastic syndromes and myeloproliferative disorders [30], but also in lymphoproliferative syndrome [31] and in acute leukemia [32]. In the last years, the PNH-like defect was observed in a large group of patients with rheumatic diseases [3]. It was also demonstrated that in endothelial cells incubated with high concentration of glucose the expression of CD55 and CD59 decreased, and could be normalized by co-incubation with the calcium channel-blocking agent verapamil [1].
There are some differences between IgM-MGUS and non-IgM-MGUS [13, 28], in particular in the risk of progression and transformation, but in our study the number of MGUS subjects was too small to allow a comparison between the hemorheological profile of IgM-MGUS and that of non-IgM-MGUS.
In conclusion, even though MGUS is an asymptomatic, premalignant disorder, it is associated with hemorheological abnormalities including not only the expected increase in PV but also a decrease in erythrocyte deformability; both alterations can be involved in the thromboembolic manifestations of the condition.
This research complies with the requirement for ethical publication in Clinical Hemorheology and Microcirculation as published in Clin Hemorheol Microcirc. 2010;44(1):1-2.