
Abstract
BACKGROUND:
Extracorporeal perfusion (EP) is moving into focus of research in reconstructive and transplantation medicine for the preservation of amputates and free tissue transplants. The idea behind EP is the reduction of ischemia-related cell damage between separation from blood circulation and reanastomosis of the transplant. Most experimental approaches are based on a complex system that moves the perfusate in a circular course.
OBJECTIVE AND METHODS:
In this study, we aimed to evaluate if a simple perfusion by an infusion bag filled with an electrolyte solution can provide acceptable results in terms of flow stability, oxygen supply and viability conservation for EP of a muscle transplant. The results are compared to muscles perfused with a pump system as well as muscles stored under ischemic conditions after a one-time intravasal flushing with Jonosteril.
RESULTS:
With this simple method a sufficient oxygen supply could be achieved and functionality could be maintained between 3.35 times and 4.60 times longer compared to the control group. Annexin V positive nuclei, indicating apoptosis, increased by 9.7% in the perfused group compared to 24.4% in the control group.
CONCLUSIONS:
Overall, by decreasing the complexity of the system, EP by one-way infusion can become more feasible in clinical situations.
Keywords
Introduction
The success of free flap transfer, organ transplantation or replantation of amputated extremities is challenged by ischemia-related cell damage [1]. This especially applies to transplants that contain muscle tissue as used in many plastic reconstructive procedures or major amputates, because the muscle‘s tolerance regarding ischemia is very limited [2, 3].
In former studies, we established an extracorporeal perfusion (EP) system using a porcine skeletal muscle as transplant model (musculus rectus abdominis). In these studies, we were able to demonstrate the superiority of EP compared to standard storage protocols [4–9].
However, there are still some major drawbacks of the EP system. One is that there is still a significant oedema formation after six hours of EP [7, 9] and a propagating oedema markedly impairs perfusion [10]. To decrease oedema formation, in this study we intend to evaluate if reducing the arterial pressure and as a consequence perfusion flow rate is possible without causing an oxygen deficiency for the muscle. In all former studies a high amount of residual oxygen leaves the venous branch [4–9]. Thus, we hypothesized that the oxygen supply of the muscle will be sufficient even with reduced flow rates and thus longer perfusion solution residence times. With this, another problem of EP can be addressed. EP as it is currently implemented, has no relevance in daily clinical routine. Most EP systems require some form of recycling in order to save perfusate, which often consists of blood components or expensive perfusion solutions [11–14]. This demands a closed sterile perfusion setup with pumps, oxygenators and other devices for perfusate regeneration, especially for a long term conservation of tissue [4–9, 11–18]. In this study, we simplified the EP system to a one-way hydrostatic setup using an infusion bag filled with electrolyte solution attached to the artery of the muscle flap with an intravenous line and a cannula without recirculation of the perfusate. If the amount of oxygen in the infusion bag proves to be enough for the demand of a free muscle transplants [6, 19], this reduced setup could become a simple and feasible tool to reduce ischemia-related cell damage of free transplants or amputates.
Methods
Animals and surgical protocol
Animals (male mature pigs, n = 5; Erzeugergemeinschaft Franken Schwaben, Tierische Veredelung, Wertingen-Geratshofen, Germany) were treated identically to previous studies [7, 9]. Both rectus abdominis muscles with the caudal vascular pedicle (inferior epigastric arteries and veins) were harvested under general anesthesia. Please check our previous publications for detailed harvesting techniques and anaesthetic procedures [7, 9].
All experiments were approved by the Government of Mittelfranken, Germany No. 65- 2532.2-1/10 and the animal care committee of the Friedrich-Alexander-University of Erlangen–Nürnberg. All experiments were carried out according to the relevant guidelines and regulations.
Extracorporeal perfusion and external field stimulation
After harvest, the flaps’ artery and vein were cannulated and the arterial cannula was attached to the infusion bag via an iv line which was placed at a height of one meter above the flap. Perfusion rate was maintained between 3 and 5 ml/min. Arterial and venous oxygen partial pressure of the perfusate were measured (Sensor type: PSt3 FTC, Transmitter: OXY – 4 – mini, Presens Precision Sensing GmbH, Regensburg, Germany) and a comparison was drawn between the two values to quantify oxygen uptake. All experiments were performed over 6 hours at room temperature. In order to avoid additional animals being sacrificed, the results of the perfused group are compared to the results that have been already published as the control of a perfused muscle with Jonosteril® with a pump is identical with the control of a perfused muscle with an infusion bag: muscles with one-time intravasal flushing with Jonosteril® prior to ischemic storage [7].
Viability of the muscle was assessed throughout the whole experiment by external field stimulation (EFS), identically to previous studies [7, 9], recording the force exerted by muscle. For this purpose, the muscles were proximally and distally fixed with clamps with a passive resting tension of the muscles set to 0.25 N, set in acrylic glass bioreactors filled with electrolyte solution (Jonosteril®). EFS was applied every 15 minutes, whereby stimulation pulses were triggered three times in a row (stimulation unit: Myotronic™ Stimulator, Myotronic UG, Heidelberg, Germany). Over the whole perfusion period the muscles’ forces declined until a point where the initial stimulation voltage is not sufficient enough. When the muscle did not react to EFS with an adequate force response (Fmax >0.5 N), the initial voltage was increased (+0.5 V) so that the resulting force is elevated. Initially high stimulation voltages could not be applied as this leads to severe tissue damage.
Histology
Histological and immunohistochemical (IHC) analyses were performed identically to previous studies [7, 9]. Tissue samples were taken before and after stimulation tests, so that force evaluation was not compromised by destroyed muscle fibers. Biopsies were fixed in buffered 4% formaldehyde before embedding in paraffin. Haematoxylin and Eosin (H&E) staining was performed as described in the protocol of the Leica Autostainer XL (Leica Biosystems Nussloch GmbH, Nussloch, Germany).
IHC staining was performed using anti-Annexin V antibody kit (ab14196; Abcam, Cambridge, UK), to detect signs of progressed apoptosis. Nuclei with positive Annexin V labelling indicate muscle cell damage as Annexin V plays a major role in the determination of cellular membrane damage and, by extension, cell necrosis [7, 20–22]. For nuclei detection, a counterstaining of the section with Haematoxylin was performed before mounting.
For IHC analysis the slides were independently analysed by two specialists to obtain double-blinded quality controls. Therefore, five high power fields (HPFs) (magnification of 200, studies area: 600×400μm) were randomly distributed over each slide and documented for quality management. Only nuclei located at the inner border of the plasma membrane of skeletal muscle cells were recorded, whereas nuclei outside the plasma membrane or close to capillaries were not included, as they may be of non-muscle origin, e.g. blood or endothelium cells. With a 400 fold magnification, the counted nuclei in the HPFs were divided into positive and negative ones.
Oedema formation
To determine oedema formation, the flaps’ weights were recorded before and after the stimulation experiments (i.e. time point 0 and 6 hours).
Regressional and statistical analysis
A two-way analysis of variance was carried out (with post hoc Holm-Sidak analysis) for values of effective force with respect to the factors treatment (perfused, ischemic) and time using sigma plot (v11.0, Systat Software, Inc.). Regressional analysis was performed with the same software.
For statistical analysis of Annexin V positive nuclei ratios of perfused and ischemic muscles, a one-way analysis of variance was carried out using the same software.
Perfusion solution
A heparinized saline solution was used for continuous EP (Jonosteril®, Fresenius Kabi Deutschland; 5000IE heparin per 500 ml Jonosteril®). The perfusate is composed of 137 mmol/l Na+, 4 mmol/l K+, 1.65 mmol/l Ca2+, 1.25 mmol/l Mg2+, 110 mmol/l Cl– and 36.8 mmol/l acetate.
Results
Oxygen consumption
On arterial side the perfusate was oxygen saturated with ambient air. On venous side there was still residual physically solved oxygen left as pO2 values between 47.1% (±10.2%) and 68.4% (±5.1%) were recorded. During perfusion the muscles consumed between 0.15 ml/min*kg (±0.03 ml/min*kg) and 0.49 ml/min*kg (±0.04 ml/min*kg) oxygen.
Preservation of muscular function
The muscles’ functionality is an important marker for the tissue’s viability. To test the muscles’ functionality EFS was used. Over each single measurement of ten seconds the muscles exert a transient maximum force Fmax which declines rapidly and approaches a more stable steady-state force Fsteady after four to five seconds of stimulation. Both values were used for functionality evaluation. In Fig. 1 an example of triple force recordings from one muscle at one point in time is given.
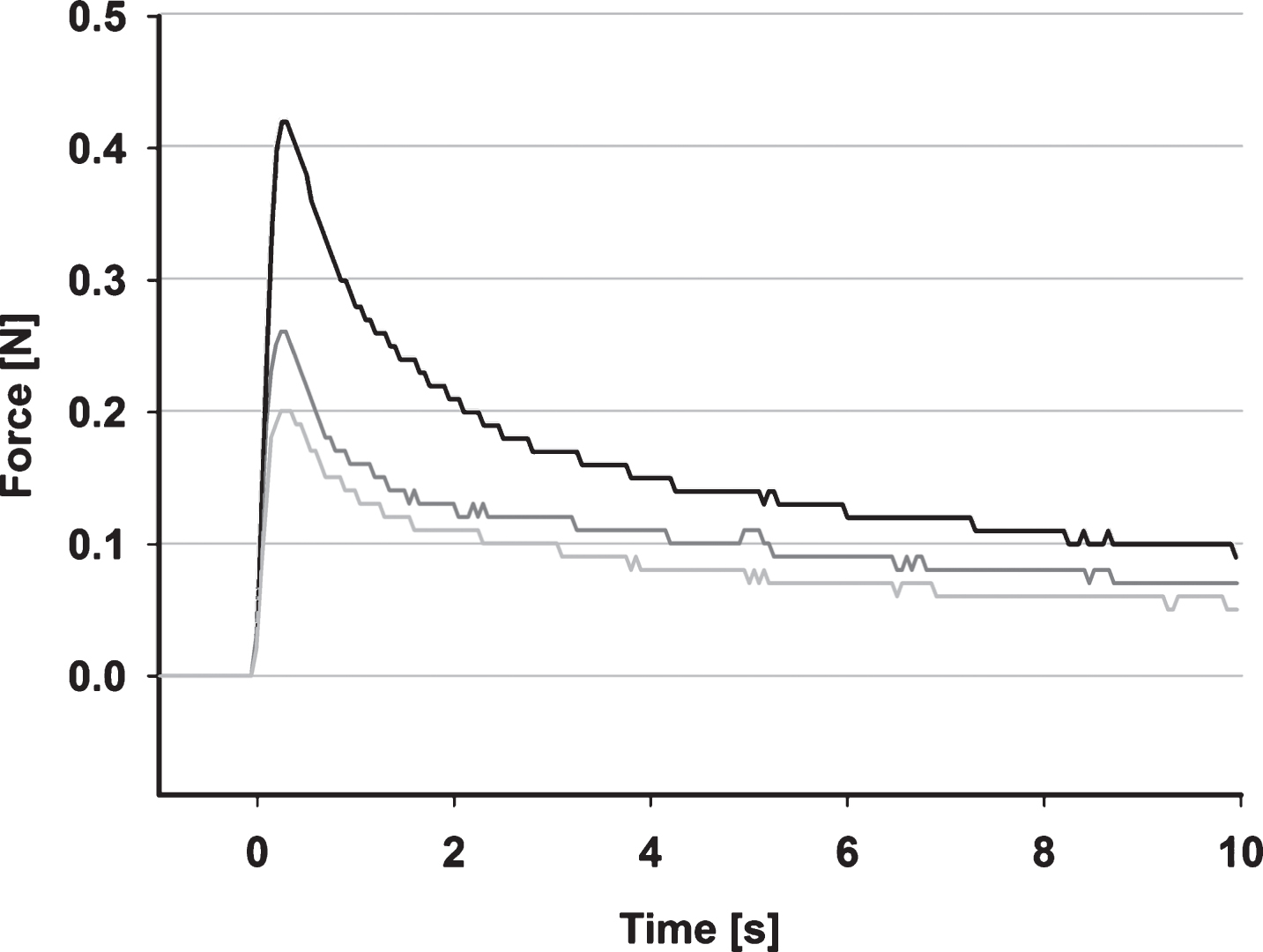
Representative force recordings taken from one muscle; forces were recorded for 10 s with a sampling rate of 20 Hz with a resolution of 0.01 N three times at every time point; black line: measurement 1; dark grey line: measurement point 2; light grey line: measurement point 3.
All muscles were treated according to the same protocol: in order to use the forces from different muscles of different length and cross-section as a relative measure between muscle flaps, the following normalization procedure proved to be useful: recorded forces at different points of time are normalized both with reference to the voltage used for stimulation as well as to the individual maximum value of effective force. The resulting effective forces (Feff,max and Feff,steady) are depicted in Fig. 2.
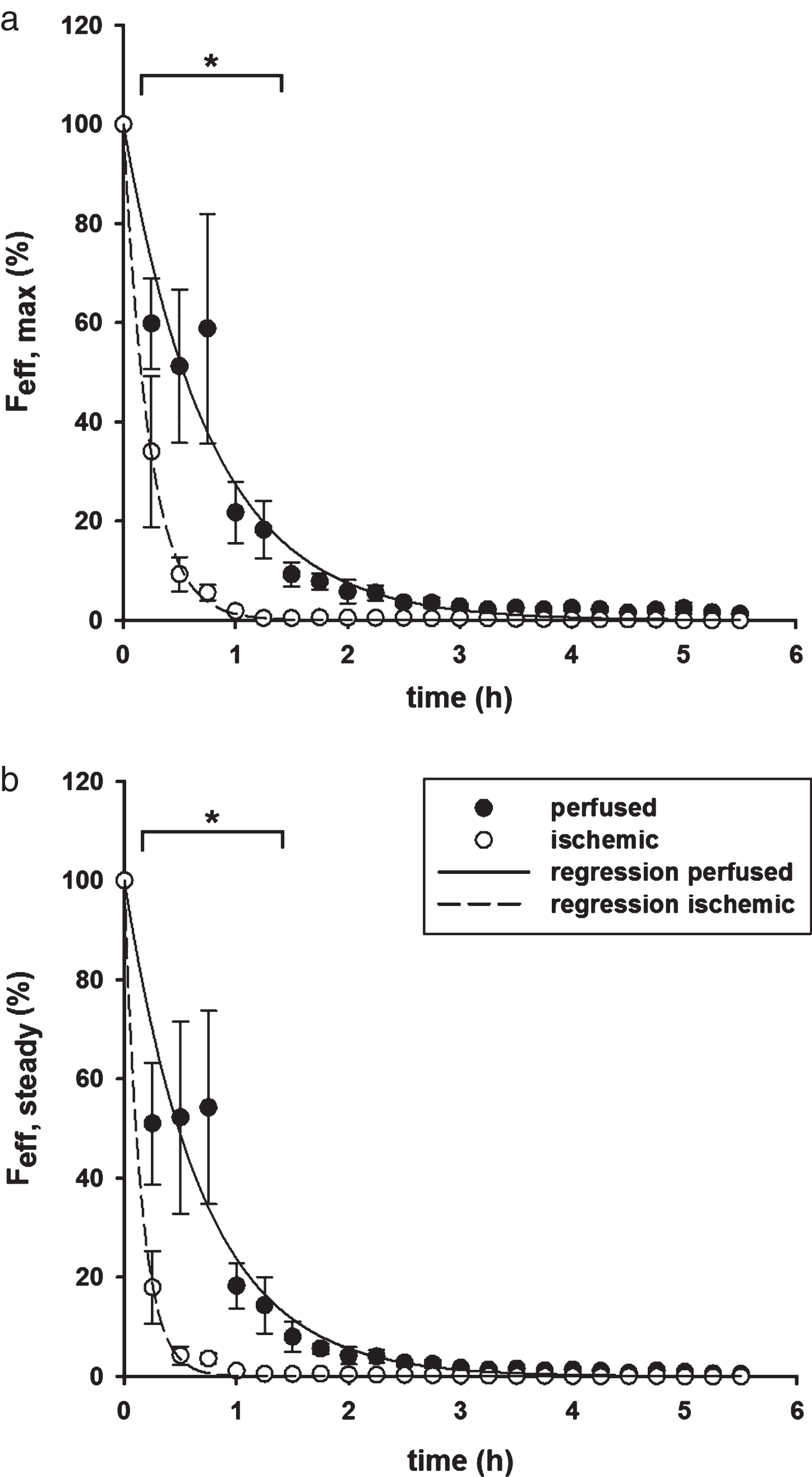
Normalized effective force per voltage of muscles undergoing hydrostatic EP (•) and ischemia [7] (∘) at different points in time after harvest; error bars represent standard error of individual values recorded at the same time (n = 5); a: Effective maximum force (Feff,max) at different points in time; b: Effective steady force (Feff,steady) at different points in time. Mathematical fits of the form F eff = a · e-μt.
Both effective forces decline markedly in the first two hours, with ischemic muscles failing to exert force between 105 and 315 minutes after harvest. All perfused muscles still exerted force after six hours, albeit significantly lower than the initial force. Statistical analysis with respect to treatment and treatment duration shows that there is an overall statistically significant difference between the two groups (p < 0.001), where the individual forces of perfused muscles are significantly higher in the first 75 minutes of perfusion regarding effective maximum forces (0.001 < p < 0.007) as well as steady forces (0.001 < p < 0.018).
Effective force values have been fitted with an exponential decay curve of the form F eff = a · e-μt, with a = 100%. Resulting force decline rates (μ) and coefficients of determination (Rsqr) are summarized in Table 1. The mean functional duration (τ) can be calculated with the reciprocal value of μ. These are also summarized in Table 1.
Resulting curve parameters after regressional analysis for effective force values over time for maximum (Feff,max) and steady (Feff,steady) forces for muscles perfused with an infusion bag or a pump and muscles under ischemic conditions [7]
The lower force decline rates of perfused muscles show that it is possible to conserve muscles’ functionality using EP, as the effective forces of ischemic muscles decline more rapidly. By putting τperfused,hydrostatic in relation to τischemic, we can say that by using hydrostatic EP the muscles’ functionality can be maintained 3.35 times longer regarding Feff,max and 4.60 times longer regarding Feff,steady.
The viability of the muscles has been evaluated by identification of apoptotic cell nuclei, marked by Annexin V. A rise in Annexin V positive cell nuclei is an indication of progressing tissue damage [7, 9]. The tissues’ integrity has been examined by staining with H&E. Representative images of muscle samples stained with H&E (Fig. 3 a&b) and against Annexin V (Fig. 3 c&d) are shown. Figure 3e also shows the ratios of nuclei stained positive against Annexin V in relation to the total number of identified nuclei.
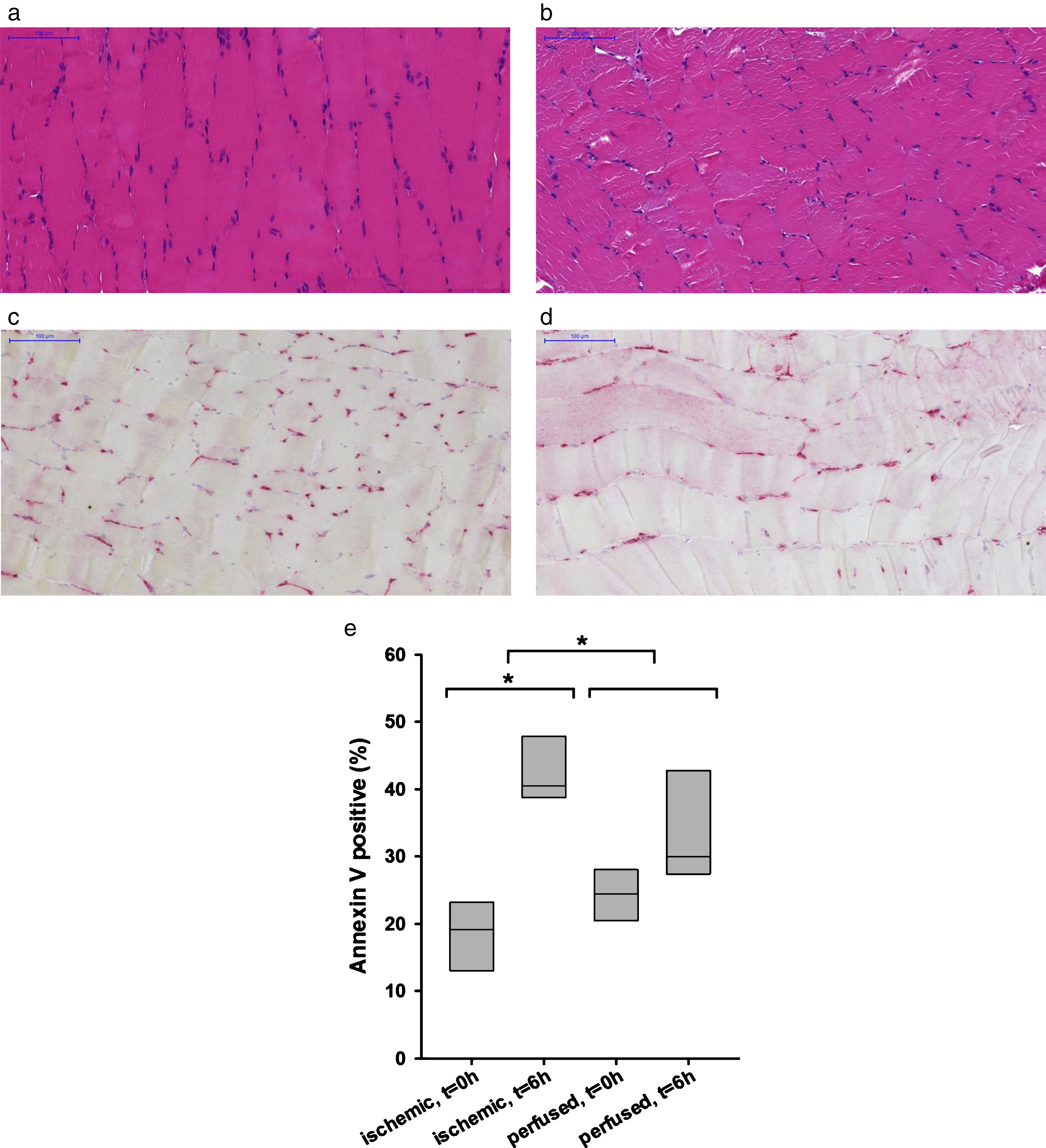
Histological images of rectus abdominis muscle tissue stained with H&E (a&b), against Annexin V (c&d), 200 fold magnification, scale is 100μm and resulting Annexin V positive ratios(e); a: H&E sample taken in vivo before muscle harvest; b: H&E after 6 h of EP; c: Annexin V sample taken in vivo before muscle harvest; d: Annexin V after 6 h of EP; e: Ratios of positive cell nuclei in relation to total number of cell nuclei for samples taken immediately after harvest and after six hours of EP or ischemia [7].
The in vivo samples already contain some Annexin V positive nuclei. Even immediately after harvest on average 24.3% (±3.4%) of all nuclei are stained positive for the accumulation of Annexin V. After six hours of perfusion this value rises by 9.7% to 34.0% (±7.2%), but without statistical significance. During six hours of ischemia the ratio of positive nuclei to the total number is statistically significantly increased by 24.4% (±6.5%) to a total of 42.7% (±4.8%), starting from 18.3% (±5.7%) after harvest [7]. When perfused with a pump this rise in Annexin V positive nuclei is also significantly lower than when suffering from ischemia: 6.3% (±4.8%). The increase of positive nuclei of muscles perfused via infusion bag is slightly higher than the one of muscles perfused by a pump but without statistical significance.
The formation of an oedema can be seen by measuring of the muscle’s change in weight after perfusion. After six hours of hydrostatic EP the average weight gain is 78.4% (±19.4%). Unperfused muscles showed no increase in weight (3.0% (±3.1%)) [7].
Discussion
The scope of this study was to evaluate the necessity of pumps and other peripheral devices that renew the circulating perfusate, or if a simple one-way infusion generates satisfactory results compared to a former study we performed using the aforementioned setup [7]. The pump’s setting of maintaining a constant volume flow rate means that an increase in resistance raised by the muscle’s vascular system is met by an increase of the pump’s perfusion pressure. This causes a widespread oedema. Gravity-driven perfusion, as used in this study, means that arterial pressure is maintained constant and perfusion flow rate is dictated by vasular resistance. But still, even with a lower perfusion pressure a high increase in weight can be observed, while the perfusion rate of the infusion method can be kept constant (between 2.8 ml/min and 5.1 ml/min). The higher residence time of the perfusate in the muscle’s vascular system still is low enough to introduce a sufficient amount of oxygen as venous oxygen partial pressure is not zero and muscles supplied by EP can in fact extract all physically dissolved oxygen [6]. The oxygen consumption of the muscles under EP by infusion (between 0.50 (±0.11) ml/(min*kg) and 0.29 (±0.10) ml/(min*kg)) is slightly higher than the one of resting muscles (0.1 ml/(min*kg)) [23, 24], but still not nearly as high as the one of muscles during intense exercise (300–400 ml/(min*kg)) [24]. The nonperfused muscle is considered to suffer from a lack of oxygen, as has been shown in previous publications [6], as diffusion of oxygen can be neglected, generating hypoxic cores in the center of the muscle just under the outer surface. Comparing force values of hydrostatic EP and pump driven EP shows that the EP system using a pump is slightly more effective. By putting τperfused,pump in realtion to τischemic, we can say that the muscles’ functionality can be maintained 4.43 times longer regarding Feff,max and 5.93 times longer regarding Feff,steady, instead of 3.35 times longer regarding Feff,max and 4.60 times longer regarding Feff,steady obtained from this setting.
Research on EP dates back to the 1980s. Most studies include the perfusion of amputated limbs from rats, pigs, dogs or even human [11, 25–28] but only some the perfusion of pure muscle tissue [12, 29]. The perfusion systems share some common elements, including a pump connected to the arterial branch of a supplying vessel, an oxygenator for gas exchange and in some cases a temperature control unit. EP is evaluated by several different methods. These include evaluating the uptake or secretion of compounds into or out of the perfusate, such as potassium, calcium, glucose, lactate, ATP, phosphocreatine kinase, or lactate dehydrogenase [11, 25–28]. Other methods are based on histology, staining with H&E or immunofluorescence [11–14, 26–28]. Another method is determining the muscle’s force response to EFS. It simultaneously examines the muscle’s viability and functionality [30]. The evaluation of muscle’s functionality after EFS or mechanical stimulation is in most cases simplified to the question if the muscle does react to stimulation or not, without quantification of the muscle’s exerted force. Muscle contractions have been observed previously after 3 hours EP [13] and up to 12 hours [11], respectively, whereas unperfused muscles showed no response [11, 13]. In this study unperfused control muscles did react to EFS, but with showed a significantly lower functional duration and individual force output than perfused ones.
In addition to viability or functionality parameters, the change in weight of perfused muscle tissue has been monitored in other studies with different results. While it has been reported that no oedema was formed during a perfusion period with whole blood of 12 hours [11], other EP techniques seem to evoke this problem as well, resulting in oedema formations ranging from 10% after 8 hours using a colloidal solution [12], 20% – 50% after 24 hours using solution based on Ringer-lactate with a low blood fraction [26], or, on average, 44% after 12 hours using a dextran-based solution [13]. In this study, using a physiological electrolyte solution for 6 hours, we observed a weight increase of 78.4% (±19.4%). When using a pump, the muscles weight increased by is 99.9% (±22.5%) [7].
As long as perfusate solutions are used which are limited in availability, e.g. autologous whole-blood or expensive perfusion solutions, EP is only feasible when performed in a closed circuit where the perfusate has to be recycled. Several promising results have been published in recent years using this technique [11–14, 32]. Some of those authors were able to show successful replantation after a prolonged EP of autologous tissue [12–14]. However, none of these approaches seems to be feasible in clinical daily routine due to the high effort associated with large perfusion systems and the limited availability of adequate perfusate solutions. We tried to simplify the method of EP to provide an easier and more cost-effective tool while still maintaining efficiency. No special expertise or equipment is necessary to perform EP. However, one has to mention that EP without recirculation of the perfusate comes along with a relatively high waste of perfusate, especially if the transplant has a large intravasal volume. A major factor that has to be addressed before EP can be transferred to clinical use is the oxygen supply. The results show that it is possible to supply the caudal segment of the musculus rectus abdominis or a muscle of comparable size and structure with oxygen adequately, without the need of an oxygenator or additional oxygen carriers, but this has to be confirmed for larger sizes. Nonetheless, one-way EP reduces the risk of bacterial contamination which poses a the major problem that prevents long-term EP [29]. The presented method of a one-way perfusion already found its way into first clinical use as already published in a case report [19].
To summarize, the results of the study show that EP can be a simple, cost-effective tool for protection of free transplanted tissue from ischemia-related cell damage. There is a significant decline in functionality, but no significant rise in tissue damage. Arterial pressure is constant during hydrostatic EP and lower than with pump driven EP, but there is still a significant formation of an interstitial oedema. A comparison with data that has been previously published [7] demonstrates the efficacy of on-way EP compared to a pump-driven circulatory EP system and the superiority to the current clinical standard, ischemic storage.
The simplicity of this setup allows it to be used on demand and without extensive preparations. However, looking at the functionality testing, there is still a large potential to improve the extracorporeal perfusion. It has to be considered whether the ongoing decline of excitability is due to the sub-normothermic perfusion with a lower cell metabolism or whether the lack of nutrients or other essential components of whole blood is the reason, or a combination of both. To clarify this the presented EP setup is an ideal model to understand which and to what extent certain components of whole blood lead to an ideal EP solution, as it is possible to selectively modulate parameters, e.g., the perfusion temperature or to add nutrients into the perfusate.
Footnotes
Acknowledgments
This study was funded by ELAN (Erlanger Leistungsbezogene Anschubfinanzierung und Nachwuchsförderung) University Hospital of Erlangen-Nuernberg FAU.
Author contributions
C.T. performed and designed the research, performed the operations, wrote the paper and supervised all experiments, O.F. helped to design the muscle contraction experiments, acted as consultant for the study and contributed to writing the paper, R.H. reviewed the paper and acted as consultant for the study, C.D. as doctoral student was involved in the experiments and analysed the data, A.W. performed the anaesthesia, C.G. performed immunohistochemistry, T.B. acted as consultant regarding perfusion parameters, C.W., S.G., L.P. and R.B. reviewed the paper and acted as consultant for the study, K.P. designed, performed and supervised the research, wrote the paper, supervised and performed all experiments.
Conflicts of interest
The authors declare no conflict of interest.