
Abstract
BACKGROUND:
Sickle cell trait (SCT) is a benign condition of sickle cell disease. Nevertheless, previous reports showed that SCT carriers have increased blood viscosity and decreased vascular reactivity compared to non-SCT carrier. The benefit of regular exercise on vascular function has been well documented in the general population but no study focused on the SCT population.
PURPOSE:
The aim of our study was to compare arterial stiffness and blood viscosity between trained and untrained SCT carriers, as well as a group of untrained non-SCT.
METHODS:
Arterial stiffness (finger-toe pulse wave velocity) and blood viscosity were evaluated in untrained non-SCT carriers (n = 10), untrained SCT carriers (n = 23) and trained SCT carriers (n = 17) who reported at least 10 hours of physical exercise per week.
RESULTS:
Untrained SCT carriers had higher pulse wave velocity (p = 0.032) and blood viscosity (p < 0.001) than their trained counterparts. In addition, untrained SCT carriers had higher blood viscosity (p < 0.001) than the untrained non-SCT group. A positive association was noted between blood viscosity and pulse wave velocity in the whole study population.
CONCLUSION:
Our study suggests that regular exercise may be beneficial for the vascular function of SCT carriers.
Introduction
Sickle cell trait (SCT) is the heterozygous form of sickle cell anemia. While usually asymptomatic, it has been demonstrated that SCT carriers could be at higher risk to develop pulmonary embolism, end-stage renal disease and ischemic stroke [1–3] than non-SCT carriers. Increased blood viscosity [4, 5], decreased vascular reactivity [6] and enhanced coagulation [7] have been reported in SCT carriers.
Pulse wave velocity (PWV) is commonly used to assess arterial compliance/stiffness and is considered an integrative marker of overall vascular function [8]. In the general population, higher arterial stiffness is associated with hypertension, ventricular hypertrophy, higher risk of cardiovascular events and lower tissue perfusion [9–15]. While sickle cell anemia has been associated with lower PWV [16–18], only two studies investigated PWV in SCT carriers [18, 19]. Both studies found that PWV was not different between SCT carriers and non SCT-carriers. However, in the study of Bayramoğlu et al. [19], the PWV values within the SCT group were highly variable as indicated by the large standard deviation suggesting large inter-subjects variability. Moreover, Diaw et al. [6] found decreased flow-mediated dilation in SCT carriers compared to non-SCT carriers suggesting slight but significant impaired vascular function in the former population that could be due to enhanced inflammation and oxidative stress, as well as impaired blood rheology.
Regular exercise increases arterial compliance in the general population, which reflects improved vascular function [20–25]. The same benefits of regular and moderate exercise on arterial compliance have been extensively described in populations at risk for cardiovascular disorders such as in metabolic syndrome and obesity [26–29]. Diaw et al. previously reported lower blood viscosity in trained compared to untrained SCT carriers but no study focused on the effects of regular physical activity on the vascular function in this population [30]. The aims of the present study were: 1) to compare PWV between physically trained and untrained SCT carriers, and a group of untrained non-SCT individuals, and 2) to investigate the possible association between PWV and blood viscosity since carotid artery elasticity has been recently found to be associated with blood viscosity [31].
Material and methods
Subjects and study design
The protocol complies with the Declaration of Helsinki and was approved by the Cheikh Anta Diop University Ethical Committee, Dakar, Senegal on November 20, 2014 (Ref: 017/2014/REC/UCAD). Ten untrained non-SCT individuals and forty SCT carriers participated in the study. Untrained non-SCT carriers (n = 10; age, 26 [20 to 33] years; BMI, 22 [16 to 24] kg/m2) and untrained SCT carriers (“SCT Untrained” group, n = 23; age, 26 [16 to 39] years; BMI, 21 [16 to 26] kg/m2) were recruited from the National Blood Transfusion Center. They all declared not having practiced regular sport activities within the last 3 years. Seventeen SCT individuals recruited from the National Institute of Popular Education and Sport (age, 26 [20 to 40] years; BMI, 21 [18 to 24] kg/m2) were assigned to the “SCT Trained” group. SCT trained subjects practiced various sports since at least three years (e.g., soccer, basketball, handball, and gymnastics) and reported to practice at least 10 hours per week. Hemoglobin electrophoresis was used to confirm the presence of abnormal hemoglobin (HbS) in SCT carriers. All subjects were non-smokers, free of diabetes and cardiovascular/systemic diseases, informed about the procedure and purpose of the study, and provided written informed consent.
All measurements were performed at the Cheikh Anta Diop University between April and November 2015. Subjects were invited to the university medical center at 8 a.m. following an 8-hour overnight fast. No sport or vigorous activity was allowed for at least 24 hours before the experimental day. Tests included blood pressure measurements, heart rate (HR) monitoring, blood sampling (to assess blood viscosity) and an evaluation of PWV.
Hemodynamic variables
Systolic and diastolic blood pressures (SBP and DBP, respectively) and heart rate (HR) were evaluated in resting conditions according to the recommendations of the American Society of Cardiology [32]. Mean arterial pressure (MAP) was calculated by using the following equation: MAP = DBP + 1/3 (SBP – DBP).
Blood viscosity and hematocrit
Blood samples were withdrawn from antecubital vein after an overnight fasting for at least 8 h to be collected in EDTA tubes (4 ml; 7,2 mg) to evaluate blood viscosity, according to the recent international guidelines for the standardization of hemorheological techniques. Blood viscosity was measured using a cone plane viscometer (Brookfield DV II + Pro, with CPE40 spindle; Middleboro, MA), at 225 s–1 and at 37°C [33]. Hematocrit (Hct) was evaluated using micro-centrifugation (Jouan-Hema-C, Saint Herblain, France) for 5 min at 1500 g and 25°C.
Assessment of arterial stiffness
Pulse wave velocity was measured as a surrogate marker of arterial stiffness using a finger-toe pulse wave velocity (PWVft) device (pOpmètre®, Axelife SAS, France) [34]. Consistent with the procedure described in Alivon et al. [11] and to ensure a resting condition, subjects were asked to remain comfortably in a supine position for at least 10 min prior to the measurement. In addition, no coffee or tobacco was allowed within the three hours preceding the experiment. Briefly, the PWVft examination consists of assessing the arterial pulse wave time offset between the finger and toe. The wave propagation speed can then be calculated using the subject size as an estimation of the distance between the two locations.
Statistical analyses
Data were expressed as median and range. All measured variables were not normally distributed. Comparisons between groups were performed using non-parametric tests (Kruskal-Wallis ANOVA). Spearman correlation tests were used to test the association between PWVft and blood viscosity. The significance level was set at p < 0.05. Analyses were performed using SPSS 16.0 software package (IBM Corporation, New York, USA).
Results
Hemodynamic variables and hematocrit
Untrained and trained SCT groups showed similar characteristics for HR, DBP and MAP, however untrained non-SCT group had higher SBP than untrained and trained SCT groups (p < 0.05). Hct was significantly lower in trained SCT than in untrained SCT (p < 0.01), but not different from the untrained non-SCT group (Table 1).
Cardiovascular and hematocrit measurements
Cardiovascular and hematocrit measurements
Untrained SCT: untrained sickle cell trait carriers; Trained SCT: trained sickle cell trait carriers; Untrained non-SCT: untrained non-SCT carriers; SBP: systolic blood pressure; DBP: diastolic blood pressure; MAP: mean arterial pressure; HR: heart rate; Hct: hematocrit; †: Difference between untrained non-SCT subjects and untrained SCT carriers (†p < 0.05); Ψ : difference between untrained non-SCT subjects and trained SCT ( Ψ p < 0.05); ¥: Difference between trained and untrained SCT carriers (¥¥p < 0.01).
As shown in Fig. 1, blood viscosity was significantly higher in the untrained SCT group than in the trained SCT and untrained non-SCT carriers (all p < 0.01).
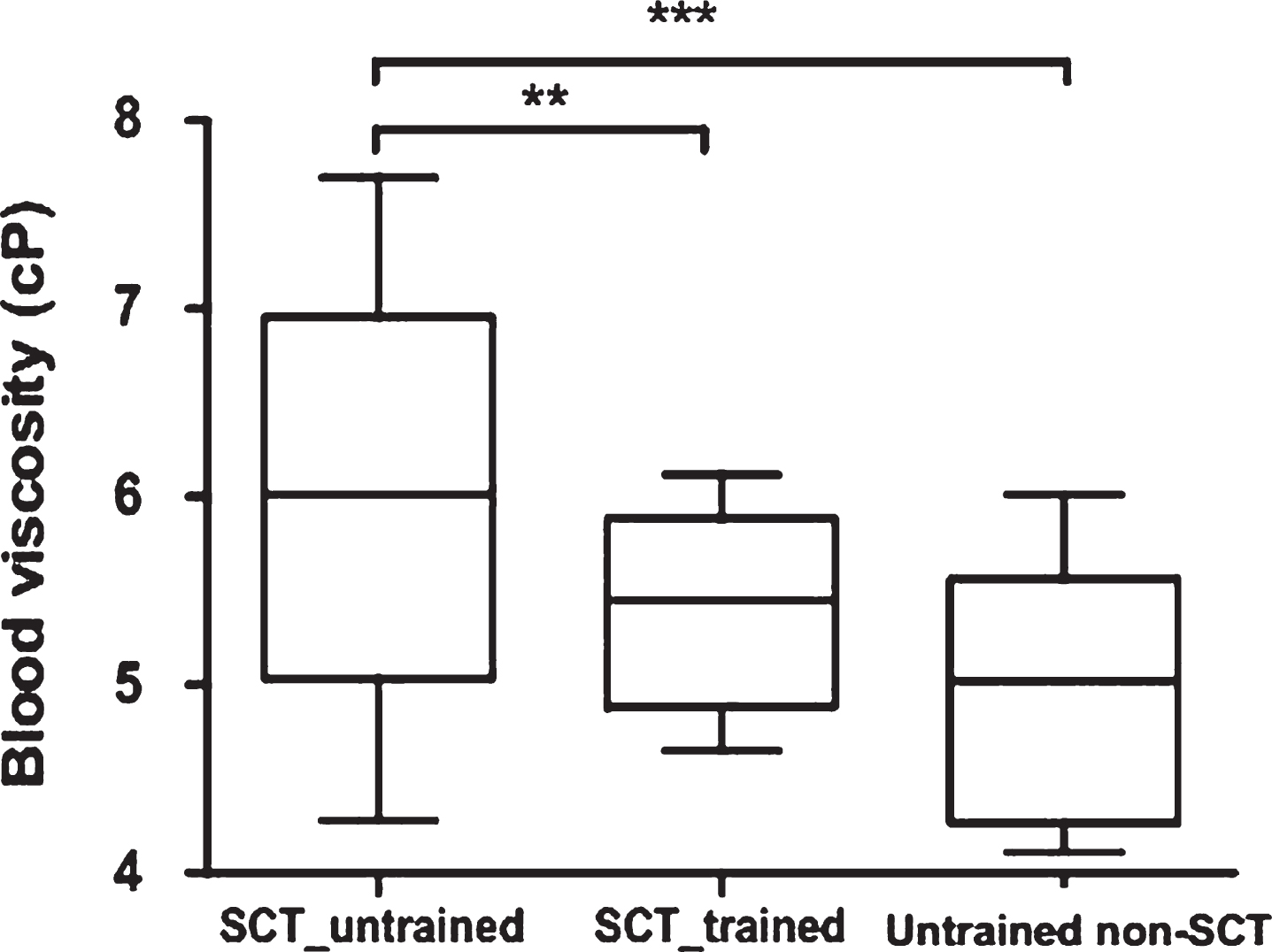
Comparison of blood viscosity between untrained and trained SCT carriers and untrained non-SCT subjects; **p < 0.01; ***p < 0.001.
The untrained SCT group had significantly higher PWVft compared to the trained SCT group (p < 0.05, Fig. 2) but was not different from the untrained non-SCT group. A positive association was detected between PWVft and blood viscosity (ρ= 0.33; p = 0.019) in the whole study population.
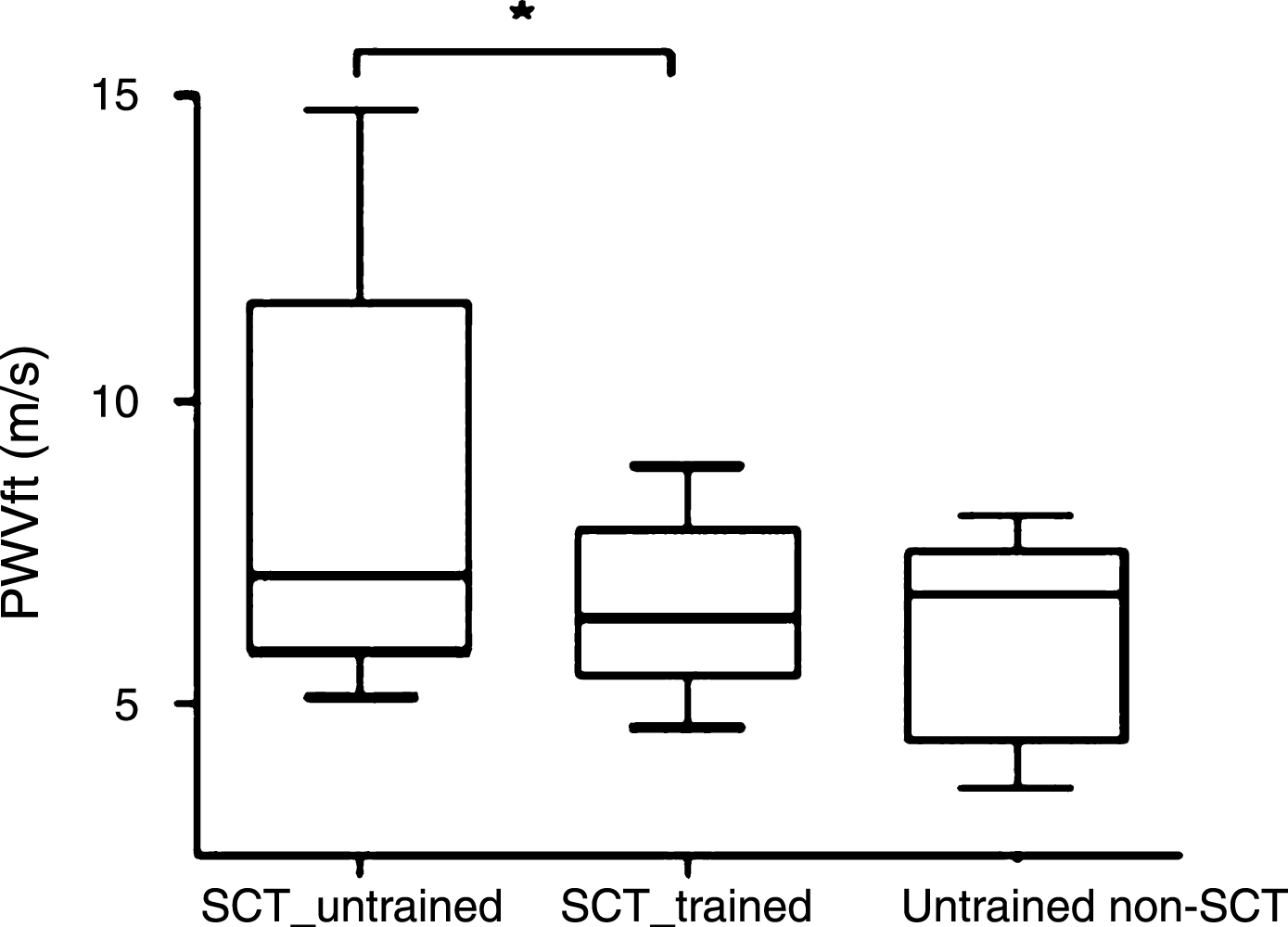
Comparison of pulse wave velocity between untrained and trained SCT carriers and untrained non-SCT subjects; *p < 0.05.
The results of this study demonstrated that trained SCT carriers have more compliant arteries and decreased blood viscosity compared to their untrained counterparts. Moreover, our findings demonstrated a significant correlation between blood viscosity and PWV in the whole study population.
Although several studies have described the beneficial effects of regular and moderate physical activity on arterial compliance in healthy populations [22, 35], the present study is the first to show that regular physical activity is also able to lower arterial stiffness in SCT carriers. Our results corroborate the literature that showed the positives effects of regular training in population with cardiovascular disorders [26–29]. For instance, low-intensity aerobic training has been demonstrated to reduce arterial stiffness [36]. Although not investigated in this study, it is highly possible that regular training [37] could have decreased inflammation and oxidative stress in SCT carriers, two parameters known to be increased in untrained SCT carriers [6].
Furthermore, sympathetic activation of the vascular smooth muscle cell causes vasoconstriction, decreasing lumen diameter, and increasing arterial stiffness [38]. Although not investigated in this study, exercise training has been shown to reduce the muscle sympathetic nerve activity in subjects with cardio-vascular risk [39], which may contribute to the better arterial stiffness observed in the present study in the trained SCT carriers. Arterial stiffness is also, in part, modulated by endothelial dysfunction [38]. Exercise training has been shown to improve endothelial function by increasing nitric oxide (NO) bioavailability and decreasing endothelial activation in SCT carriers [45, 46].
Our study also detected a decreased blood viscosity in trained compared to untrained SCT carriers, as it was previously reported [30]. This finding may be explained by the fact that trained SCT carriers had also decreased Hct compared to untrained individuals. Similar to subjects with normal hemoglobin, sport training-related plasma volume expansion was likely responsible for the improvement in blood viscosity [40, 41]. We could also suspect that regular training has led to a decrease in plasma viscosity [30, 43]. It has already been suggested that a low blood viscosity in SCT carriers could improve blood flow in both the macro- and microcirculation and enhance oxygen supply to muscles [44]. Therefore, the hemorheological improvement observed in the present study supports the hypothesis that sport training should be considered as a strategy to decrease cardiovascular strain and prevent medical events that are sporadically observed in SCT carriers [30, 46]. Regular physical activity has been shown to promote the production of NO by endothelial cells and to decrease the level of endothelin-1 in healthy individuals, which results in improved arterial function [47]. We found a positive correlation between PWV and blood viscosity in the whole population studied. Through its effects on shear stress and on the activity of the endothelial NO-synthase activity, blood viscosity plays a key role in the maintenance of normal vascular resistance in healthy individuals [48]. However, in case of impaired vascular function, which seems to be the case in SCT carriers [6], elevated blood viscosity could lead to vascular remodeling, endothelial inflammation and vascular damage [49]. Indeed, the correlation found in the present study suggests that lowering blood viscosity by regular activity in SCT carriers could participate to decrease arterial stiffness.
One limitation of this study is the lack of a trained non-SCT group. However, because the effects of regular exercise on arterial stiffness has already been described in healthy population [47], we focused mainly on SCT and included only a group composed of untrained individuals.
In conclusion, the results of the present study showed the beneficial effects of regular exercise on arterial compliance in SCT carriers. It is the responsibility of the medical community to determine whether SCT should be recognized as a medical condition. The prescription of regular and moderate exercise is a simple way to improve the vascular function of SCT carriers like in other population.