
Abstract
BACKGROUND:
Ischemia-reperfusion injury may lead to insufficient microcirculation and results in partial flap loss during the free flap surgeries.
OBJECTIVE:
This study aimed to investigate the effect of trimetazidine (TMZ) on oxidative stress, inflammation and histopathological changes, using the epigastric skin flap model in rats.
METHODS:
40 male Wistar rats were used, that were divided into four groups. Control group, non-treated ischemic (I/R)-group and two trimetazidine treated groups (preischemically, postischemically) were established. To create ischemia in the skin flap, the superficial epigastric vessels were clamped for six hours, followed by twenty-four hours of reperfusion. Blood samples and biopsies from skin flaps were collected at the end of the reperfusion period. The inflammatory response, the degree of oxidative stress (by measuring the plasma level of malondialdehyde (MDA), reduced glutathione (GSH); sulfhydryl (–SH) groups) and histopathological changes were evaluated.
RESULTS:
Inflammatory response, and oxidative stress were significantly attenuated in the trimetazidine treated groups, compared to the non-treated ischemic group. Histopathological findings were also correlated with the biochemical results.
CONCLUSION:
In our study trimetazidine could reduce the ischaemia-reperfusion injury, even after an unexpected ischemic period, so it is a promising drug during free tissue transfer, replantation or during revascularization procedures in the future.
Keywords
Introduction
Ischemia-reperfusion (I/R) injury can cause considerable problems in various fields of the surgery, like in reconstructive plastic surgery, vascular surgery, traumatology or cardiac surgery. Ischemia-reperfusion injury is a cascade of pathophysiological events, that can occur after the reperfusion of the tissues, exposed to prolonged ischemia and results in tissue damage [1, 2]. Unfortunately, this condition is unavoidable during free flap surgery or during replantation. Free tissue transfer has become a routine procedure to cure tissue defects after oncological ablative surgery or trauma. In the last decade, the technique of the free flap surgeries improved a lot and it has reached the 90–95% success rate. Although, the success rates of these surgeries are high, there are still some cases, where the insufficient microcirculation, caused by I/R injury, leads to partial flap loss and results in the reoperation of the patient. In addition, the flap/limb can become irremediable because its poor circulation, and it may make the reconstruction more difficult or impossible [3–7]. For these reasons the detection of biochemical changes and microcirculatory disorders in flaps during I/R, are of high importance [8, 9].
Even though many drugs and methods have shown promising results experimentally, there is not an existing consensus treatment in the clinical practice, because of their unfavourable systemic side effects, excess toxicity, limited efficacy, invasive administration or because of the time-consuming technique [10–15].
Trimetazidine (TMZ, water soluble form: trimetazidine-dihydrochloride) is a widely used anti-anginal drug worldwide. It is a potent anti-ischemic agent and a free radical scavenger. It has been used in many studies to protect different organs (myocardium, the intestine, liver, and kidney) from the ischemia-reperfusion injury. Numerous evidence exists, which shows that the reperfusion injury could be decreased by TMZ-preconditioning in animals. It was found that TMZ conserves ATP production, maintains cellular homeostasis and reduces the intracellular acidosis [16]. Moreover, it decreases the oxidative damage to the mitochondria and protects the organ from tissue damage, induced by I/R injury [17, 18]. Furthermore, Devynck et al. investigated the effect of TMZ on membrane in human platelets and found that TMZ reduced cAMP content and aggregation responses to collagen and ADP [17]. TMZ is accepted as an agent without any hemodynamic activities, and only minor side effects (episodes of a headache) were mentioned in a few cases [19].
We hypothesised that a single shot of TMZ will be protective against I/R injury. This study aimed to investigate the effect of trimetazidine on oxidative stress, inflammation, and histopathological alterations (before visible changes (e.g. tissue necrosis) occur), using the epigastric skin flap model. To determine the efficacy of TMZ, levels of blood malondialdehyde (MDA), reduced glutathione (GSH), and plasma thiol groups (SH-) and tissue TNF-alpha were measured, histopathology and immunohistochemistry were performed.
Material and methods
Animal model
Forty male Wistar rats of the same age, weighing between 350 to 400 g, were used for this study. The rats were housed in separate cages, under standard conditions (temperature: 25±2°C, and air filtered room), with 12/12-hour light-dark regimen and were fed with standard rat chow, and water ad libitum. Food was withdrawn 12 hours prior to experiment. The study protocol was approved by the National Scientific Ethical Committee on Animal Experimentation (number: ZOHU0104L 16).
Experimental protocol
The animals were divided randomly into four groups (10 rats in each group). The first group was the non-ischemic control group. Although the control flaps did not undergo ischemic insult, flap harvest produced some temporary ischemia. In the other groups (groups 2 through 4) ischemia was induced by placing a single microvascular clamp across the epigastric superficial artery and vein. In the second group (I/R) the superficial epigastric vessels were clamped for 6 hours, followed by 24 hours of reperfusion. The third (Preisch.TMZ+I/R) and fourth (I/R+Postisch.TMZ) groups were the trimetazidine treated groups. In the third group, the TMZ was administered 30 minutes prior to the ischemic period. In the last group, animals received the drug at the onset of the reperfusion (Fig. 1). To standardize the study, all procedures were performed at similar time points in all groups. Animals, in the treated groups, received 10 mg/kg trimetazidine (trimetazidine-dihydrochloride, Sigma-Aldrich, St. Louis, Missouri, USA) intraperitoneally (i.p) depending on the groups, 30 minutes prior to ischemia (Preisch.TMZ+I/R) or at the onset of the reperfusion (I/R+Postisch.TMZ). The drug was freshly solved into 0,9 % NaCl solution before the administration.
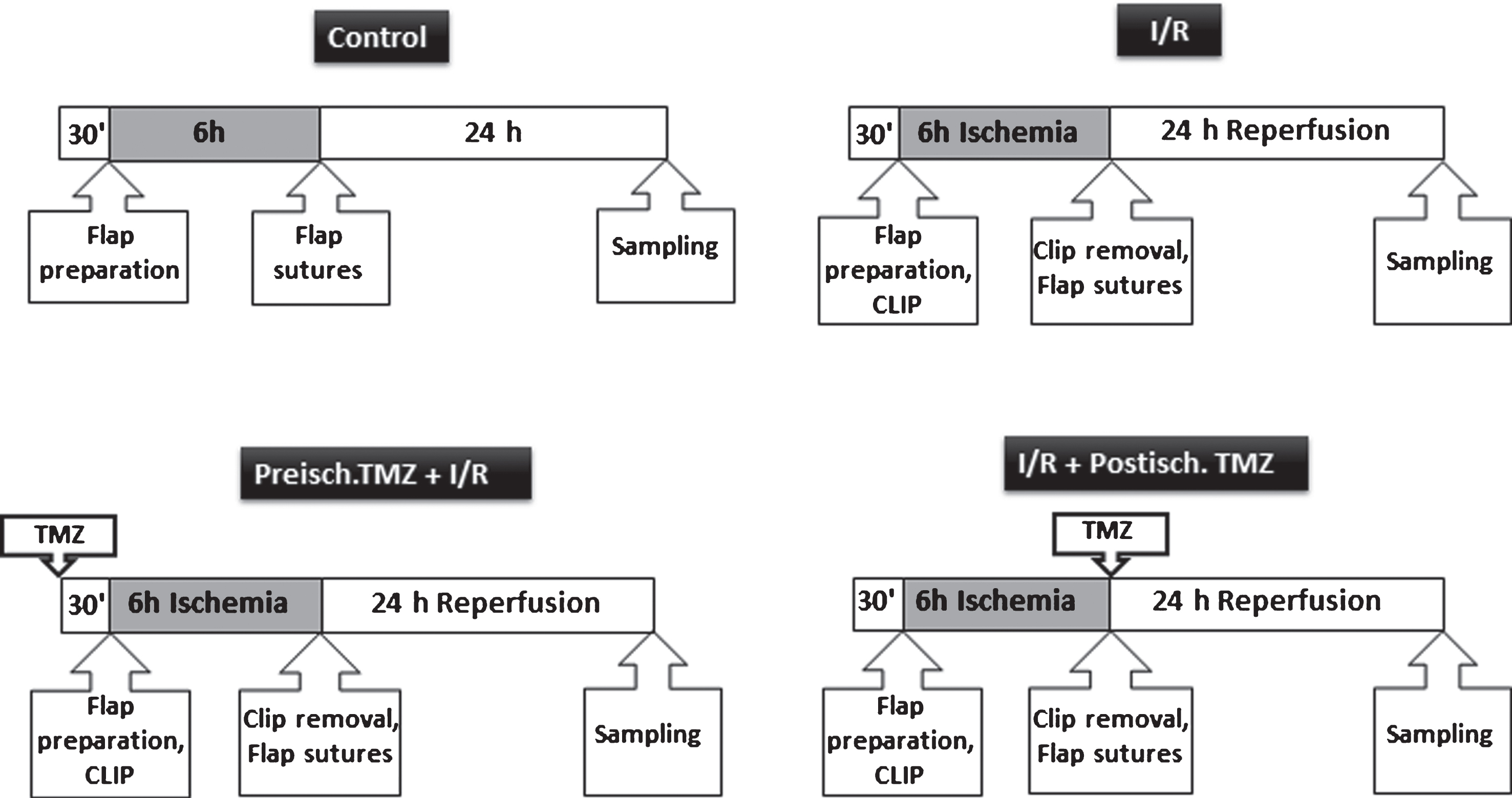
Investigation groups: I: ischemia, R: reperfusion, TMZ: trimetazidine.
The rats were perioperatively anesthetized with an intraperitoneal (i.p) application of a mixture consisting of ketamine hydrochloride (5 mg/100 g) and diazepam (0,5 mg/100 g). The ratio was 1:1. The skin of the abdomen was depilated using an animal depilatory agent. During the operation, the animals were placed on a heated pad and ECG monitoring was also used. The carotid artery was catheterized (22 gauge) for blood pressure measurement. (Siemens Sirecust 1260, Düsseldorf, Germany). The skin of the abdomen was scrubbed with betadine and then 3×6 cm flap was created on both sides of the abdomen. In our study, the epigastric flap was chosen, because it simulates microsurgical free tissue transfer closely. This model was first described in 1967 by Strauch and Murray and has been widely used in various experimental animal researches on I/R injury and skin flap survival [20–23]. The flaps include the area within the boundaries of costal arch as an upper limit, the inguinal ligament as a lower limit and both axillary lines as lateral borders. The medial borders were on both sides of the midline structures (the xiphoid and pubis). The vascular supply of the flap is provided by the medial and lateral branches of the superficial epigastric artery and accompanying veins, based on the superficial epigastric vascular pedicle. After 6 hours of ischemia, the microvascular clamp was released and the blood flow was confirmed by arterial pulsation, flap colour, and the vascular patency test was also performed to ensure that the blood flow is recovered successfully. Flaps, where we could not detect any flow, were not included in this study. After checking the blood flow, the skin was sutured back to its original place with interrupted stitches (5–0, Prolene (Ethicon), 30 stitches on both flaps). After the operation, the animals got a collar neck to prevent the automutilation. On the next day, before the sampling, animals were re-anesthetized.
Skin samples (3×1 cm) were taken from the most distal end of the flaps, after 24 hours of reperfusion, for biochemical examination. The samples were stored immediately at –80°C within individual containers. MDA, GSH, SH levels were measured from these skin samples. MDA is a marker for the quantification of membrane lipid peroxidation. MDA levels were detected using a photometric method of Placer, Cushman and Johnson [24]. GSH and plasma SH levels were determined in anticoagulated whole blood by Ellman’s reagent, according to the method of Sedlak and Lindsay [25]. Both indicate the antioxidant status of the body. To measure the TNF-alpha levels and to perform histopathological analysis, samples were taken from the central part of the flap. Tissue TNF-α (one of the indicators of the inflammatory response) levels were studied by using the Rat TNF-α ELISA Kit (Abcam, Cambridge, UK) following the manufacturer’s protocol. A histopathological study of the samples was carried out by the same pathologist. The tissue samples were fixed in 10% neutral buffered formaldehyde solution and embedded in paraffin. Three-micron-thick (Microtome: Thermo Scientific Microm Hm 325) histological sections were cut, mounted on glass slides, stained with haematoxylin-eosin (HE) and evaluated by light microscope to quantify foreign body giant cells, polymorphonuclear, and mono-nuclear reactive cells. For detection of apoptosis, TUNEL was also performed.
For statistical evaluation, one-way analysis of variance (ANOVA) was used, followed by adequate post hoc tests (Dunnett’s, Sidak) for multiple comparisons. All data are represented as the mean±SEM. The difference was considered statistically significant when p value was less than 0.05.
Results
The statistical analysis of the MDA levels showed significantly reduced values in the pre-ischemic trimetazidine treated group compared to the I/R group (59,84±2,8 vs. 75,3±6,4; p = 0,0145), which refers to smaller lipid peroxidation (Fig. 2).
Significantly higher GSH levels, both in pre-and postischemic trimetazidine treated groups (preisch. TMZ: 965,5±6,3, p = 0,0035; postisch. TMZ: 1002±38,6, p = 0,0002 vs. 820,9±13,5) also supported an antioxidant effect of the drug (Fig. 3).
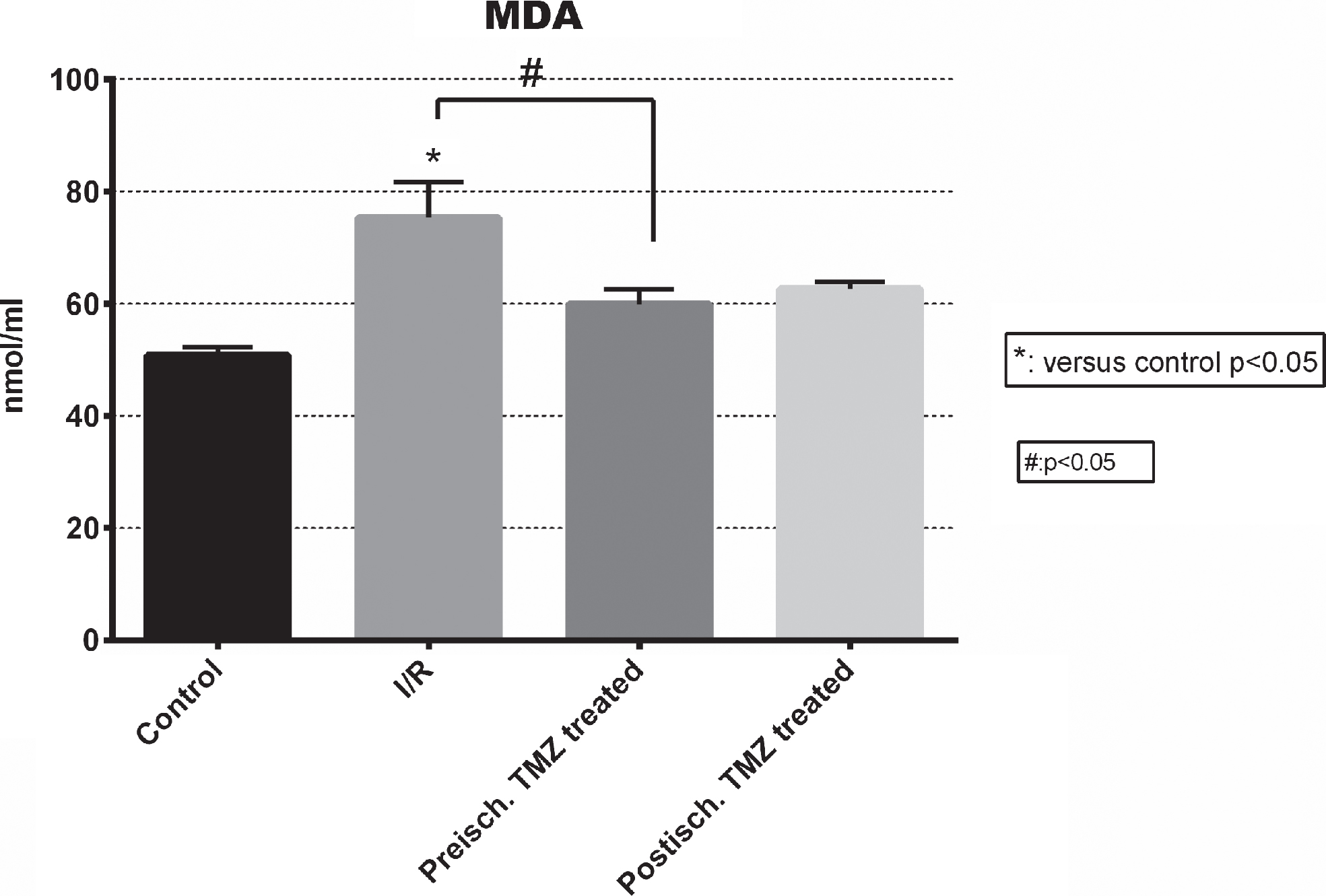
Malondialdehyde concentrations in the experimental groups. MDA serves as a marker of the lipid peroxidation. *: p < 0,05 vs. control; #: p < 0,05 between the signed groups; error bars: SEM.
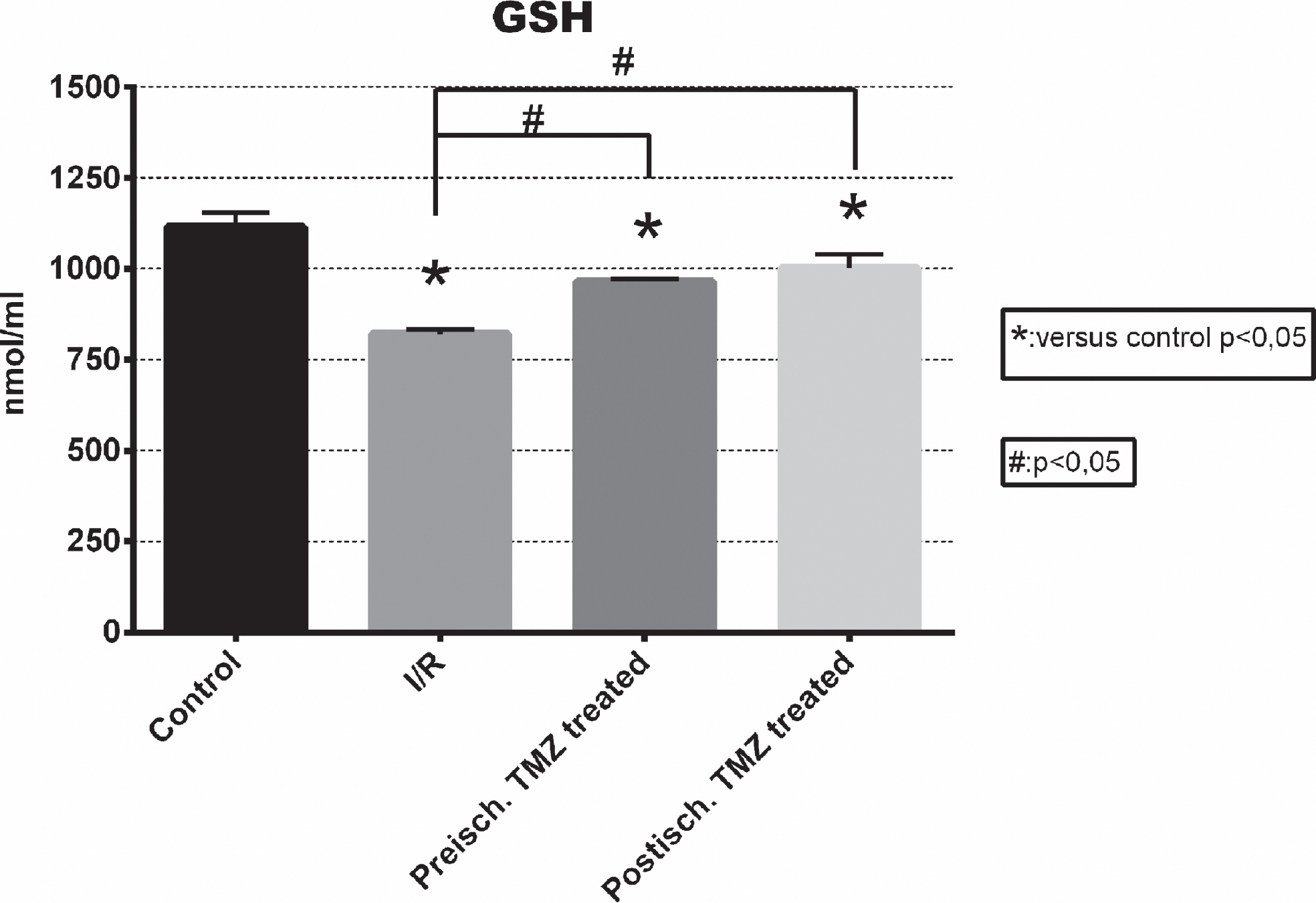
Plasma concentration of reduced glutathione in the investigated groups. GSH serves as a marker of the antioxidant status. *: p < 0,05 vs. control; #: p < 0,05 among the signed groups; error bars: SEM.
There were no significant differences in the SH- levels among the groups (control: 94,03±8,584; I/R: 74,3±3,763; preisch.TMZ: 98,62±11,4; postisch.TMZ: 91,65±6,5) (Fig. 4).
The considerable decrease of TNF- α levels in the treated groups compared to the I/R group (preisch. TMZ: 41243±2183 p = 0,0001; postisch. TMZ: 54025±5924 p = 0,0437 vs. 73331±5762) can prove the anti-inflammatory effect of the drug (Fig. 5).
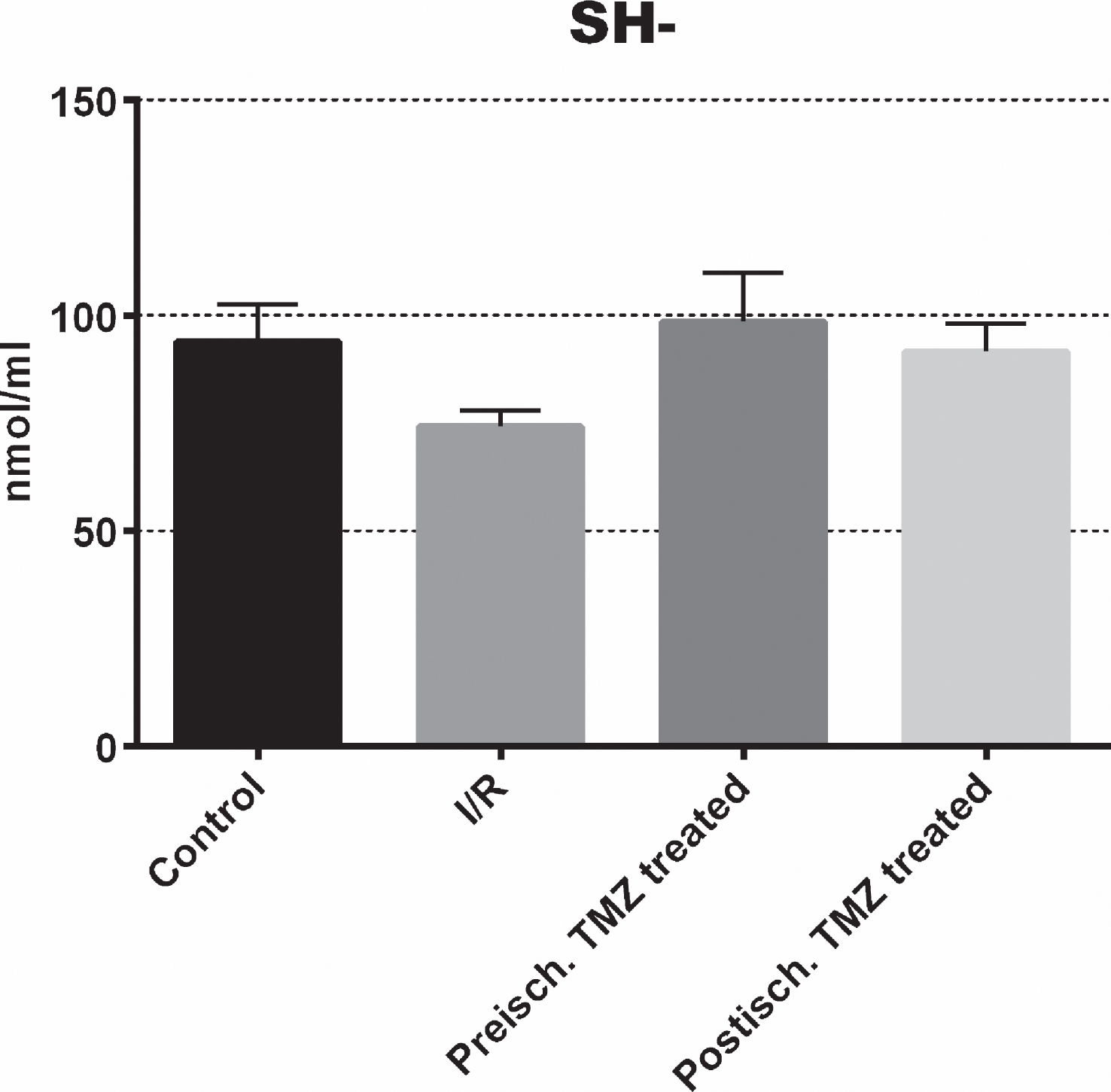
Concentrations of SH- groups in the plasma. The levels of SH- refer to the antioxidant status. Error bars: SEM.
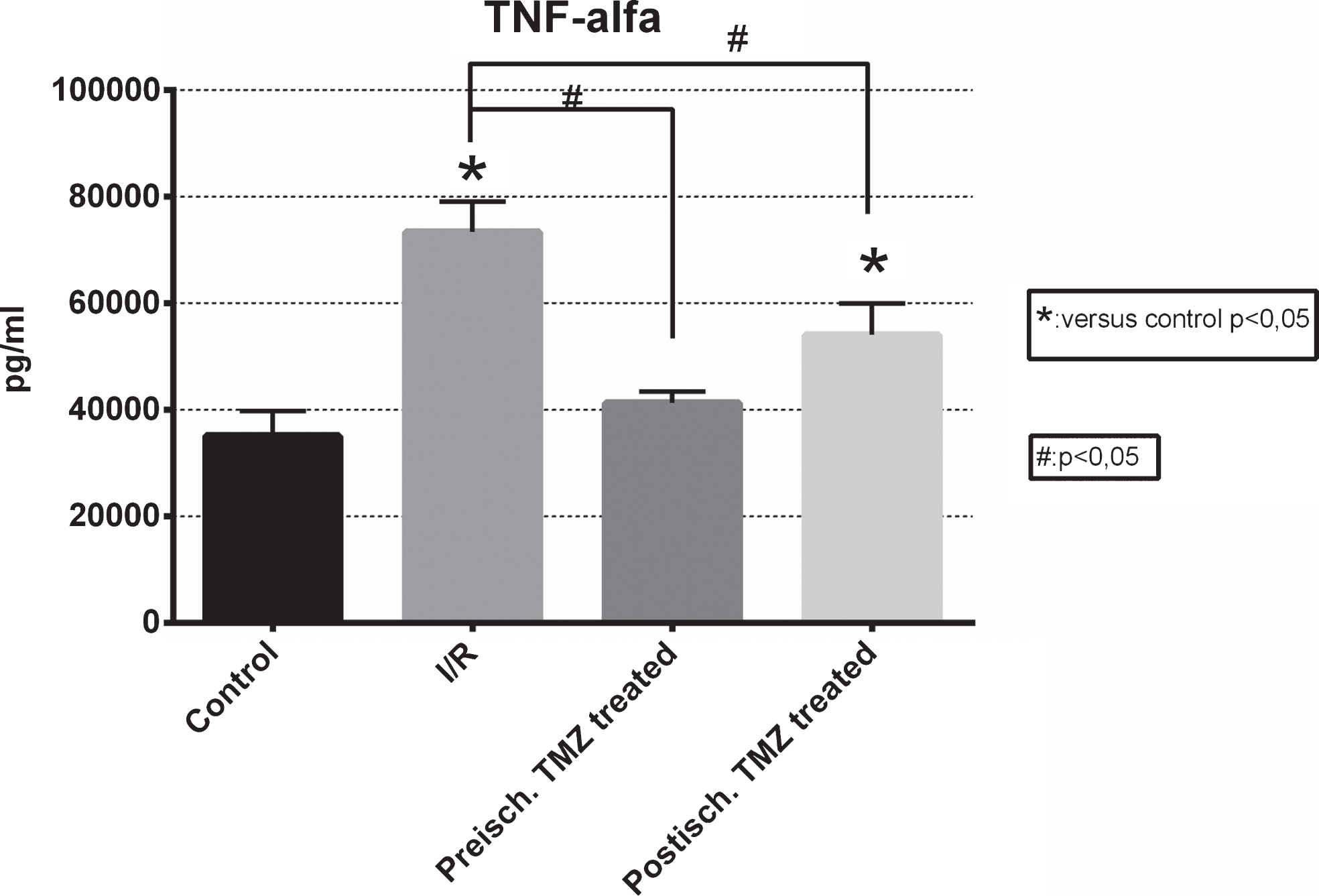
TNF-alpha concentrations show the grade of the inflammatory response in the investigated groups. *: p < 0,05 vs. control; #: p < 0,05 among the signed groups; error bars: SEM.
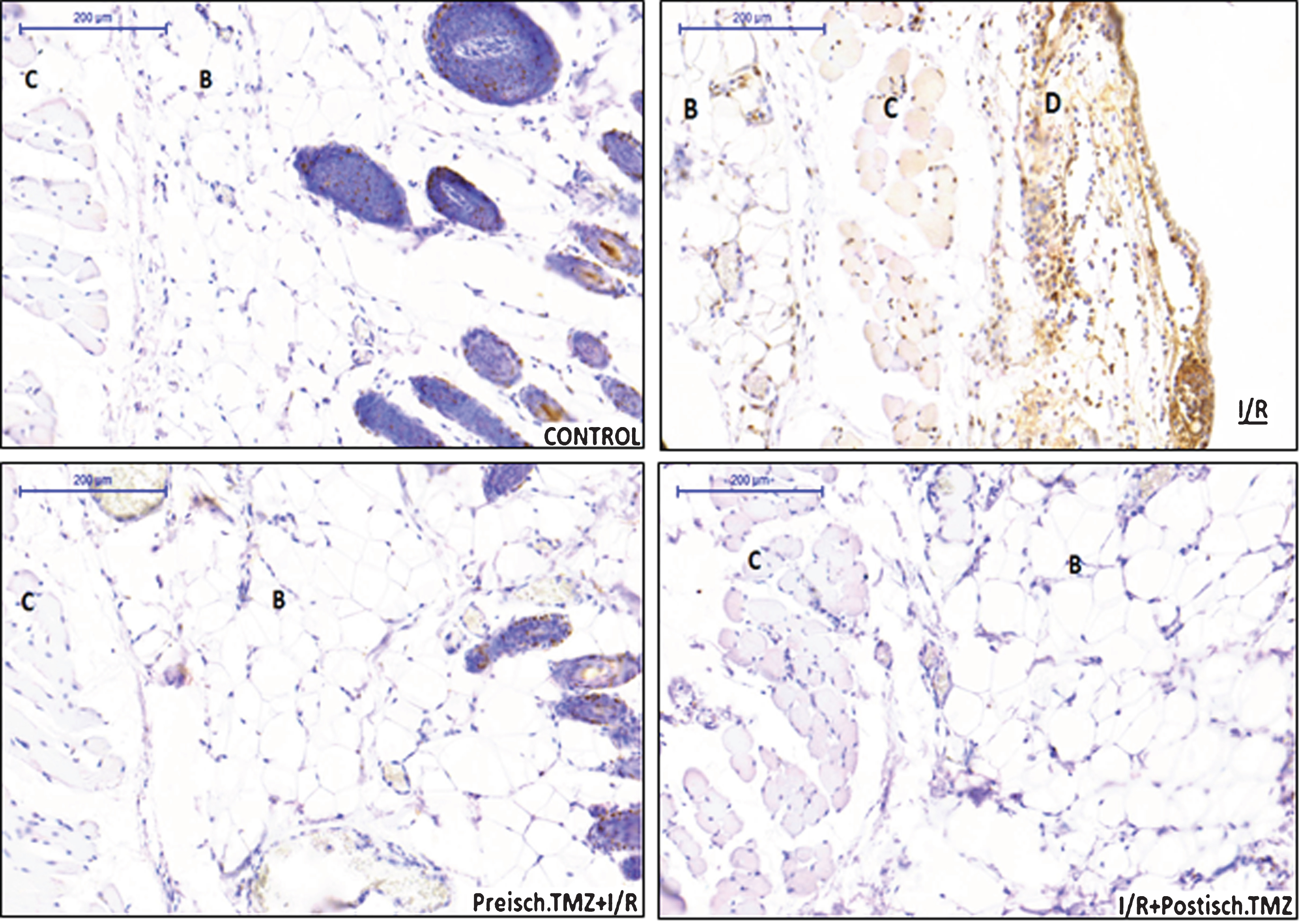
Our histopathological findings correlate with the biochemical results. Four zones are identified in all tissue samples (Fig. 6, Control). In the control group, the basic tissue structures mainly kept, oedema, necrosis or significant inflammation cannot be detected.

Staining: HE, magnification: 5x. In the control group, the four zones can be clearly identified: A: epidermal-dermal zone; B: fatty zone; C: muscular zone, D: submuscular zone. In the I/R group oedema can be seen in the submuscular and fatty zone and the muscle fibres are swollen and irregular-shaped in the zone C. The protective function of the TMZ is well demonstrated in both (Preisch. TMZ+I/R and I/R+Postisch. TMZ) groups, showing less changes in the tissue samples: muscle fibres are approximately normal shaped, oedema and PMN-cells are barely detected in the different zones.
In the I/R group (Fig. 6, I/R) many changes can be noticed: oedema was occurring in the fatty zone and in the submuscular zone. A large number of polymorphonuclear (PMN) cells could be seen under the muscle. The muscle fibres were swollen and irregular-shaped.
In both TMZ treated groups tissue changes were seen to a lesser degree than in the I/R group. The muscle fibres were approximately normal shaped, oedema and PMN-cells were barely detected in the different zones (Fig. 6; Preisch. TMZ+I/R, I/R+Postisch. TMZ).
The good influence of the drug is also supported by TUNEL staining (Fig. 7). In the control group the high number of positive cells, showing up only in the follicle, are physiological - since these are holocrine glands (Fig. 7; Control). In the I/R group (Fig. 7, I/R) many apoptotic cells were found in every zone of the flap. TUNEL-positive nuclei were stained brown. This confirms that I/R also promotes the apoptosis. The TMZ management of skin flaps clearly decreased the quantity of the apoptotic cells. Apart from the epidermal-dermal zone, where apoptotic cells can be found physiologically, the number of the positive cells were considerably less in the treated groups, compared to the I/R group (Fig. 7; Preisch. TMZ+I/R, I/R+Postisch. TMZ).
Staining: TUNEL, magnification 10x: TUNEL staining demonstrates the apoptotic nuclei. 1. In the control group the high number of positive cells, showing up only in the follicle, are physiological - since these are holocrine glands. 2. The homogeneous positivity in the I/R group is the evidence to demonstrate the damage in the tissue, caused by the ischemia/reperfusion. 3. The protective function of the TMZ is well demonstrated in both (Preisch. TMZ+I/R and I/R+Postisch. TMZ) groups, showing barely positivity in all investigated zones.
The use of microvascular flap transfer is very popular for defects of the whole body. It is known, that the success rate of the microsurgical vascular anastomosis, even with experienced surgeons is 90 to 95 percent, however, some severe problem such as I/R injury or the inadequate blood perfusion may still impede the complete success. I/R injury can cause severe problems in the microcirculation and it may lead to patient’s morbidity and prolonged hospitalization. The intracellular biochemical changes that occur during the ischemic period can cause cellular dysfunction, cellular and interstitial oedema and finally can lead to cell death. Severity of these changes depend on the length of the ischemic time, since it is well known that brief ischemic condition can be protective against the negative alterations [26]. During reperfusion, following the ischemic period, reactive oxygen species are produced, which include oxygen ions, free radicals, and peroxides, all of which worsen ischemia-reperfusion damage [27, 28], impact on red blood cells micro-rheological parameters and may result in considerable disturbance of blood flow [29–31]. In the pathogenesis of I/R injury inflammation is also considered to be a critical element [32, 33].
In our study, we chose the superficial epigastric skin flap model, because it was suitable to simulate a clinical situation, that occurs when microsurgical tissue transfer is made. As Yoshida and Campos suggested the model could also simulate a vascular pedicle thrombosis, where the procedure from the diagnosis to the restoration of vascular supply could reach or exceed 6 hours, or it also can simulate a traumatic situation when replantation of amputated fingers is made [34]. In these type of models, flaps contain the epidermal-dermal zone, fatty zone, muscular zone (panniculus carnosus) and submuscular zone with a vascular pedicle of the superficial inferior epigastric artery and vein. There are controversies related to the position of the microvascular clamp. They could be used on both the artery and on the vein, or separately on the vein or on the artery to simulate different situations, which can occur in the clinical practice. Our experimental model based on superficial inferior epigastric artery and veins to reach a higher level of I/R injury and the extension of the flaps were 6,0×3,0 cm bilaterally.
The length of the ischemic time was based on the literature [35]; ÇetIn et al. [33]. subjected the rats to 6 hours and 10 hours of ischemia, because these time points have been reported to produce consistent biochemical, histopathological and macroscopic findings [36].
TMZ is a potent anti-ischemic drug, which decreases fatty acid oxidation and stimulates glucose utilization via the inhibition of the mitochondrial long chain 3 ketoacyl-CoA thiolase, leading to the production of adenosine triphosphate (ATP) with less oxygen consumption. It limits intracellular acidosis, decreases sodium and calcium accumulation into cells, inhibits the extracellular leakage of potassium during cellular ischemia and reduces cytolysis and membrane injury caused by oxygen free radicals. In addition, TMZ conserves mitochondrial function and energy metabolism and it is capable of inhibiting platelet adhesion-aggregation and neutrophil infiltration [19, 38]. Because it does not have a negative alteration on the hemodynamic status, besides the cardiology, it also can be useful in other areas of the clinical practice.
Previously, the effect of the TMZ on the survival of skin flaps was already studied and the agent was proved to be effective. Nieto et al. investigated various pharmacological agents on the survival of skin flaps in rats. All treated groups showed a significantly greater survival of the flap than the control group. One of the best outcomes was shown in those groups receiving trimetazidine and hydralazine [39]. Kara et al. studied the effect of trimetazidine on the survival of rat island skin flaps. They compared the pre-ischemic and post-ischemic effect of the drug, and both ways seemed to be effective to improve flap survival [40].
However, this is the first study where, before the visible tissue changes, the histological and biochemical alterations were investigated after pre-and postischemic TMZ treatment in skin flaps. Blood MDA, GSH, and SH- levels and tissue TNF-α levels were evaluated for biochemical analysis. MDA is a stable product of polyunsaturated lipid peroxidation in cells, that is generated after free radical damage. GSH is one of the major endogenous antioxidants produced by the cells, participating directly in the neutralization of free radicals and reactive oxygen compounds. The serum levels of protein -SH in the body, can indicate antioxidant status. TNF-α is a polypeptide compound and it is an important member of the cytokine family, which plays a significant role in the regulation of the systemic inflammatory response.
In the literature, there are controversies in the administration routes and doses of this antioxidant agent [41–43]. In our study 10 mg /kg dose was chosen and the drug was administered intraperitoneally, based on some previous studies where this dose was proved to be effective [34, 44]. The timing was also different in many studies. For example, Khan and colleagues [42] published that TMZ was cardioprotective (via the activation of p38 mitogen-activated protein kinase and Akt signalling pathway) when administered at the beginning of the reperfusion period. Elimadi et al. [44] investigated the effect of TMZ on hepatic warm I/R injury, administered as an intramuscular injection with different doses (5 mg, 10 mg, 20 mg). They demonstrated that 10 mg/kg/day for 7 days before the induction of ischemia was the optimal dosage, that gave the maximal protective effects at both cellular and mitochondrial level. All these observed differences among the studies could be a consequence of different animal models, examined organs and I/R protocols. Further investigations are required to determine the optimal time and dose of administration of TMZ and to have more insight into clinical application.
In our study, we hypothesised that a single shot of TMZ will be preventive against I/R injury in epigastric skin flaps. Since in the previous studies the timing of the administration of TMZ was different, we investigated both pre- and postischemic TMZ treatment. Our data confirm the earlier findings, that TMZ has anti-inflammatory and anti-ischemic effects, independently of the timing. It could be a useful drug in the surgical practice to increase the survival time of the tissue, not just given before a planned ischemic period but also after an unexpected trauma where a reconstructive surgery is required.
Conclusion
TMZ is a clinically applicable and non-toxic agent, which may increase the ischemic tolerance of the tissues and can protect them from ischemia-reperfusion injury, even after an unexpected ischemic insult.