
Abstract
INTRODUCTION:
Laparoscopy is more beneficial than the conventional open technique, however the pneumoperitoneum created may have an ischemic side effect.
OBJECTIVE:
Our aim was to evaluate the protective effects of preconditioning during laparoscopic cholecystectomies (LC).
METHODS:
30 patients were randomized into 2 groups: I. PreC (preconditioning: 5 min. inflation, 5 min. deflation, followed by conventional LC), II: LC (conventional LC). Blood samples were taken before hospitalization (C = control), before surgery, after anaesthesia (B.S.), after surgery (A.S.) and 24 hours after the procedure (24 h). Measured parameters were: malondialdehyde (MDA), reduced glutathione (GSH), sulfhydril groups (-SH), superoxide-dismutase (SOD), catalase (CAT), myeloperoxidase (MPO), length of hospitalization and pain (VAS = visual analogue scale).
RESULTS:
Compared to the BS levels, no significant changes were detected in SOD’s activity and MDA levels. GSH concentrations were significantly increased in the PreC group after operation. SH-, MPO, CAT and liver function enzymes were not significantly different. Hospitalization was shorter in the PreC group. Based on the VAS score patients had less pain in the PreC group.
CONCLUSION:
Significant differences concerning PreC group were found in GSH values. In the PreC group pain decreased by 2-2.5 units following the procedure, 24 h after surgery, and hospitalisation was also significantly shorter. In our pilot study the potential protective effect of preconditioning could be defined.
Introduction
Laparoscopy is considered as a substantial diagnostic and therapeutic method in current surgical practice. Laparoscopic technique is much more beneficial than conventional open technique regarding many aspects like less postoperative pain and shorter hospitalization. However, there are some concerns about its adverse effect. Pneumoperitoneum created for better visualisation and for working place causes an increased intra-abdominal pressure (12–15 mmHg) which decreases perfusion of the splanchnic area. Due to hypoperfusion and ischemic-reperfusion injury reactive oxygen radicals and inflammatory cytokines accumulate [1–3]. This injury depends on the magnitude and length of the increased intra-abdominal pressure, however there is not enough information on the complications due to increased intra-abdominal pressure (IAP). Studies performed on animals had confirmed that the systemic oxidative stress caused by high IAP, this is why laparoscopic procedures are performed at the lowest IAP, still sufficient for a safe operation. Murry et al. [4] noted that short repeated ischemia/reperfusion cycles, – the so-called preconditioning (early, classical preconditioning)-before long ischemic insults can reduce oxidative stress in the myocardium. Implementing preconditioning, a stronger, better and longer defence against injury develops 24 hours after reperfusion. (late preconditioning, "second window of protection” SWOP). Aksöyek et. al reported that preconditioning can reduce ischemic damage in abdominal organs as well [5]. Javor et al. have proven on Wistar female rats that preconditioning can reduce negative effects of pneumoperitoneum [6]. Remote Ischemic Conditioning (RIC) has been demonstrated to be an effective way to improve microcirculation of surgical flaps in humans. Kolbenschlag J et al. in their randomized study examined 60 healthy volunteers randomized into different groups and received a RIC protocol consisting of three cycles of either 1 second, 1, 5, 10 minutes of ischemia followed by ten minutes of reperfusion. RIC was applied with an inflatable tourniquet placed on the upper arm. Changes in microcirculation were assessed via combined laser Doppler/spectroscopy (O2C device) at the anterior lateral thigh. They found that RIC caused significant changes in cutaneous microcirculation (p < 0.05) that were more pronounced in groups with longer ischemia intervals. The ten-minute RIC group was significantly superior [7]. The aim of our pilot study was to investigate whether preconditioning (5 min. inflation-5 min. deflation) before laparoscopic operations could reduce the harm caused by pneumoperitoneum.
Preconditioning: Ischemic preconditioning is intended to create an increased tolerance to ischaemia and reperfusion induced by a previous sublethal period of ischemia. During the short ischemic preconditioning period, several trigger substances are released (adenosine, bradykinin, norepinephrine, opioids etc.). By activating the membrane-bound receptors these substances activate a complex intracellular signalling cascade, which converges on mitochondrial end-effectors, including the ATP-sensitive potassium channel and the mitochondrial permeability transition pore. Activation of this pathway protects the cells against both necrosis and apoptosis during a subsequent more prolonged ischemic episode. The protection caused by preconditioning lasts only for two to three hours, but reappears 24 hours after the preconditioning stimulus. This ‘delayed preconditioning’ requires synthesis of new proteins, including inducible nitric oxide synthase (iNOS), cyclooxygenase-2 (COX-2) and heat shock proteins.
Patients and methods
This pilot study was conducted from February 2013 to June 2014 at the Surgery Clinic and at the Department of Surgical Research and Techniques, University of Pécs, Hungary. Informed consent was obtained from patients before the procedures. This study was carried out in accordance with the Code of Ethics of the Declaration of Helsinki. The study protocol was authorized by The Hungarian Committee of Ethics (No. ad.774/PI/2012; ad.50760/2012/EKU). As it being a pilot study we decided to involve only thirty patients into this study. In case of favourable results a multicentre study could later be implemented. At random a total of thirty patients admitted for elective laparoscopic cholecystectomy were enrolled in this prospective blinded clinical study. 15 patients were submitted to preconditioning before the operation, and 15 were operated on with a routine laparoscopic procedure. Patients were randomized by procedure utilizing sequentially numbered opaque sealed envelopes to one of the two groups (ratio 1:1) by the study coordinator. The study was single blinded. The operating surgeon right before the operations received a closed envelope containing cards “LC” or “preconditioning”. Patients were not informed which procedure they were assigned to, neither after they filled in the VAS questionnaire nor after leaving the hospital. Patients were not informed about randomization results. Anaesthesia was performed by the same team using similar protocols. Patients aged between 18 and 70 years were entitled in the study. Information sheets were given about the procedure and patients signed an Informed Consent prior to the operation. Exclusion criteria included any known malignancy, morbid obesity, any disorder of the immune system, autoimmune disease, uraemia, massive hypoproteinaemia, icterus, chronic decompensated hepatic disorder and refusal to participate. Laparoscopic operations were performed in the Surgical Clinic of the University of Pécs (Hungary); analysis of blood samples and all statistical calculations were performed at the Department of Surgical Research and Techniques and Institute of Bioanalysis of the University of Pécs. All patients were operated on under general anaesthesia. Antibiotics and low molecular weight heparin were not administered preoperatively. A skin incision was made in the umbilical region, and in the preconditioning phase pneumoperitoneum was created by CO2 insufflation using a Veres needle. After trocars were inserted, the intra-abdominal pressure was set at 15 mmHg.
The limitations of this study lie in the heterogeneity of the patients, and the limited patient numbers. However this was only initiated to test the idea of preconditioning during pneumoperitoneum, and to measure any detectable biochemical changes. It was also useful to select those parameters that were rather heterogeneous to provide useful information. These parameters were age, co-morbidity of patients, the majority of measured oxidative parameters.
Preconditioning: Before starting dissection a 5 minutes interval was kept with constant 15 mmHg intraabdominal pressure, followed by another 5 minutes with complete deflation of the abdomen. After this procedure a routine laparoscopic cholecystectomy was performed also using 15 mmHg pressure. Venous blood samples were collected from patients on four occasions: before hospitalization (BH), after induction of anaesthesia (A), after operation (AO) and on the 1st postoperative day (Post). Lipid peroxidation marker malondialdehyde (MDA) concentration, endogenous antioxidant reduced glutathione (GSH) and sulfhydryl-group (SH-) concentrations, antioxidant superoxide-dismutase (SOD) and catalase (KAT) activities were measured from whole blood for detecting the magnitude of oxidative stress. Plasma malondialdehyde (MDA) concentration and myeloperoxidase (MPO) activity were also measured from plasma. We also checked liver enzyme changes. Pain was evaluated with Visual Analog Scale on the day of the operation, and 24 hours later. Size and state of wounds as well as adverse reactions were evaluated.
Detection of malondialdehyde (MDA) concentration
A mixture of 4.5 ml TBA (thiobarbituric acid) and TCA (trichloroacetic acid) were added to 0.5 ml plasma or diluted blood. Samples were incubated for 20 minutes at 100 C° then cooled at 0 C°. Blood was centrifuged in a cooled centrifuge at 4000 rpm for 15 min. The concentration of MDA was determined using a spectrophotometer at 532 nm and expressed in nM/ml [8].
Detection of reduced glutathione (GSH) and sulfhydryl-group (SH-) concentration
For the determination of GSH and SH- a mixture of one ml quintuple blood sample and 4 ml trichloroacetic acid (TCA) were used. The mixture was centrifuged at 4000 rpm for 15 min. The supernatant was added to 4 ml TRIS puffer (0,4 M, pH:8,7) 2 ml and 100μl DTNB (5.5’-ditio-bis-2-nitro-benzoe acid) was added to the mixture immediately before measurement. The concentrations of GSH and SH- were determined using a spectrophotometer at 412 nm and expressed in nM/ml [9].
Detection of superoxide-dismutase (SOD) activity
For the determination of SOD activity 1 ml blood was mixed with EDTA, then 9 ml Hartman’s solution was added to the blood sample. The mixture was centrifuged at 2000 rpm for 5 min. After discarding the supernatant the washing procedure was repeated. A mixture (2 : 1) of 1 ml chloroform and ethanol were added to 1 ml haemolysed red blood cells and they were centrifuged at 17000 rpm for 4 min. Supernatant was separated thereafter, and adrenalin (16.488 mg adrenalin diluted in 10 ml 0.1 N hydrochloric acid) was added to it. The concentration of SOD was determined by using a spectrophotometer at 480 nm and expressed in U/ml [10].
Detection of myeloperoxidase activity (MPO)
For the determination of MPO activity 1 ml work solution (10.9 ml Na-citrate, 100μl o-Dianisidin) was mixed with 200μl plasma. The compound was incubated at 37 C° for 5 min, then 1 ml of 35% perchloric acid was added to the mixture and centrifuged at 2500 rpm for 10 min. MPO concentration was measured using spectrophotometer at 560 nm and expressed in U/l.
Detection of catalase levels (CAT)
To determinate the catalase enzyme level we mixed 2 ml of buffer, 1 ml of peroxide solution and a 100 times diluted, washed red blood cell. With spectrophotometer we measured the loss of peroxides at 240 nm. Catalase levels were expressed in BE/ml.
Statistical analysis
The Statistical Package for Social Sciences (SPSS; SPSS Inc., Chicago, IL) version 22.0 was used for statistical analysis. Serum MDA, GSH, SH, SOD and plasma MDA, MPO levels were analysed using Mann-Whitney or Wilcoxon singed – rank test. Statistical significance was set at p≤0.05. The graphic expression of the data was performed in box plots.
Results
In total 30 patients were enrolled in the study. The mean age was 38.3±6.4 years and the length of procedure was 25–80 mins. Distribution ratio between male-female was 6 : 24. Average hospitalization was 2.37 days but in PreC group we noticed a shorter hospitalization by 10%. Comparing the two groups, the mean hospitalization was 2.67 days in the LC group (SD 1.047), and 2.29 days in the PreC group (SD 0.72). (Mann-Whitney test p = 0.377)
SOD
Data was very heterogeneous, therefore no statistical analysis was carried out. During control (C) we measured almost the same SOD activity.(LC 720.71 U/ml; SD: 334.18; PreC 720.56 U/ml, SD: 251.22) According to the B.S data it can be concluded that anesthesia causes decrease in SOD activity in both groups, but this decrease was not significant (LC 655.54 U/ml, SD: 308.95; PreC 645.91 U/ml, SD: 210.32). A.S. we concluded the following: LC 674.67 U/ml, SD: 303.60; PreC 690.58 U/ml, SD: 223.37 and 24 h after operations LC 730.76 U/ml, SD: 217.19; PreC 631 U/ml, SD: 169.34.
MDA (blood)
In case of MDA concentration moderate heterogeneity was also detected. There was no significant difference between LC and PreC groups.(C groups: LC 82.30 nM/ml, SD: 4.15; PreC 79.43 nM/ml; SD: 5.35; B.S. groups: LC 82.51 nM/ml, (SD: 3.81) PreC 82.08 nM/ml; (SD: 11.49) A.S. groups: LC 87.03 nM/ml, (SD: 5.2); PreC 90.03 nM/ml; (SD: 21.99) 24 h groups: LC 85.75 nM/ml, (SD:10.95); PreC 85.26 nM/ml (SD: 11.11).
GSH
In case of GSH concentrations we also noticed heterogeneity, but in the PreC group a significantly higher concentration was measured postoperatively (908.80 nM/ml, SD: 81.65) compared to the LC group (853.93 nM/ml, SD: 67.70). (M-Wht test p = 0.05) Fig. 1.
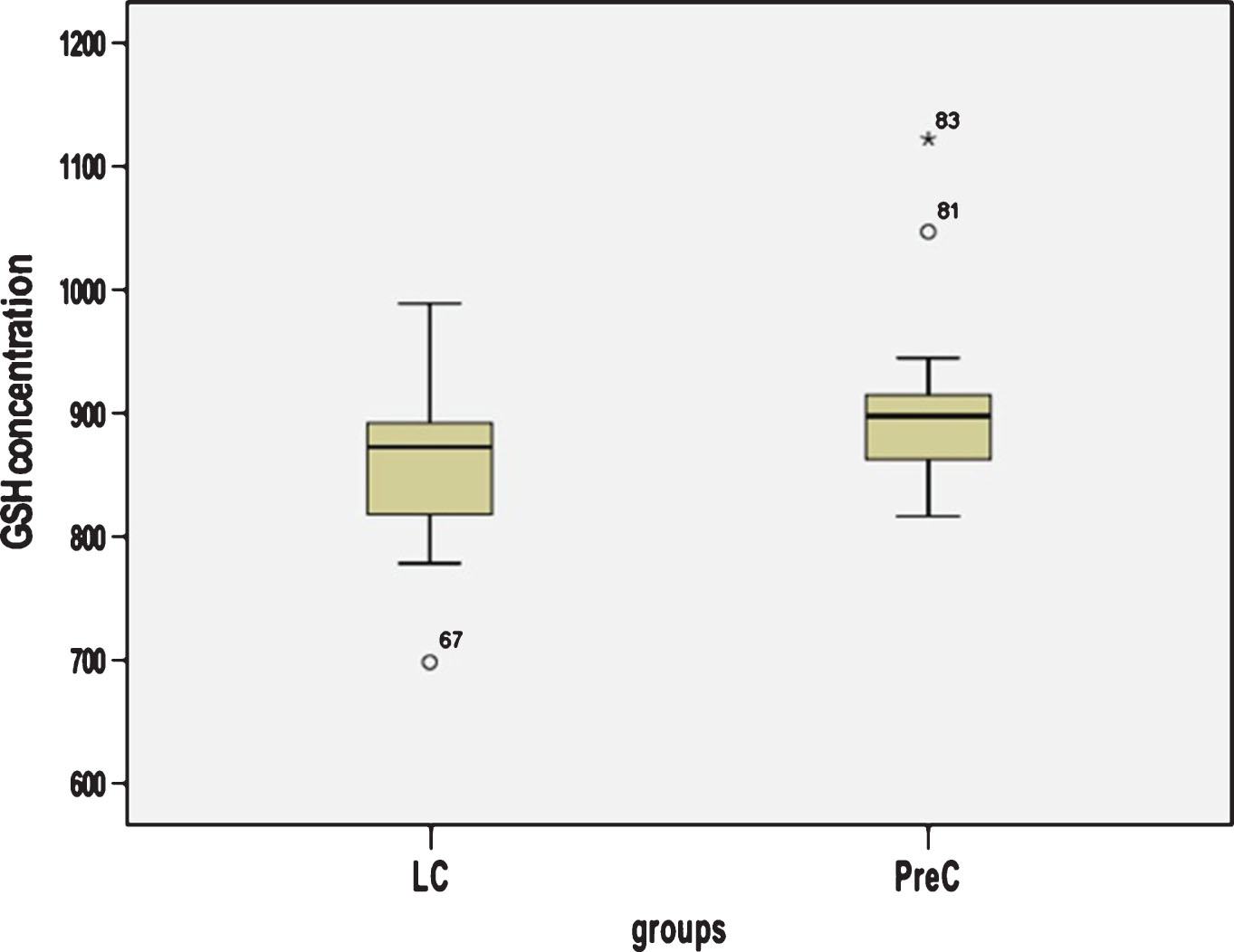
In the PreC group a significantly higher concentration was measured postoperatively compared to the LC group. (M-Wht test p = 0.05).
No significant changes were detected in SH- concentration and catalase levels.
MPO, MDA (plasma)
In case of plasma MPO activity and MDA concentration we noticed no significant changes.
Pain measured with Visual Analog Scale
A significant difference was noted in the PreC group, both after the operation (LC 6.60 U, SD 1.77; PreC 4.25 U, SD 2.17) (p = 0.014 M-Why test), and also 24 hours later (LC 3.10 U, SD 1.5, PreC 1.17 U, SD 1.03) (p = 0.006 M-Why test, p = 0.005 Wilcoxon singed – rank test). Pain in PreC group was about 2–2.5 units lower at both times. One day advantage was detected in pain level due to preconditioning. Fig. 2.
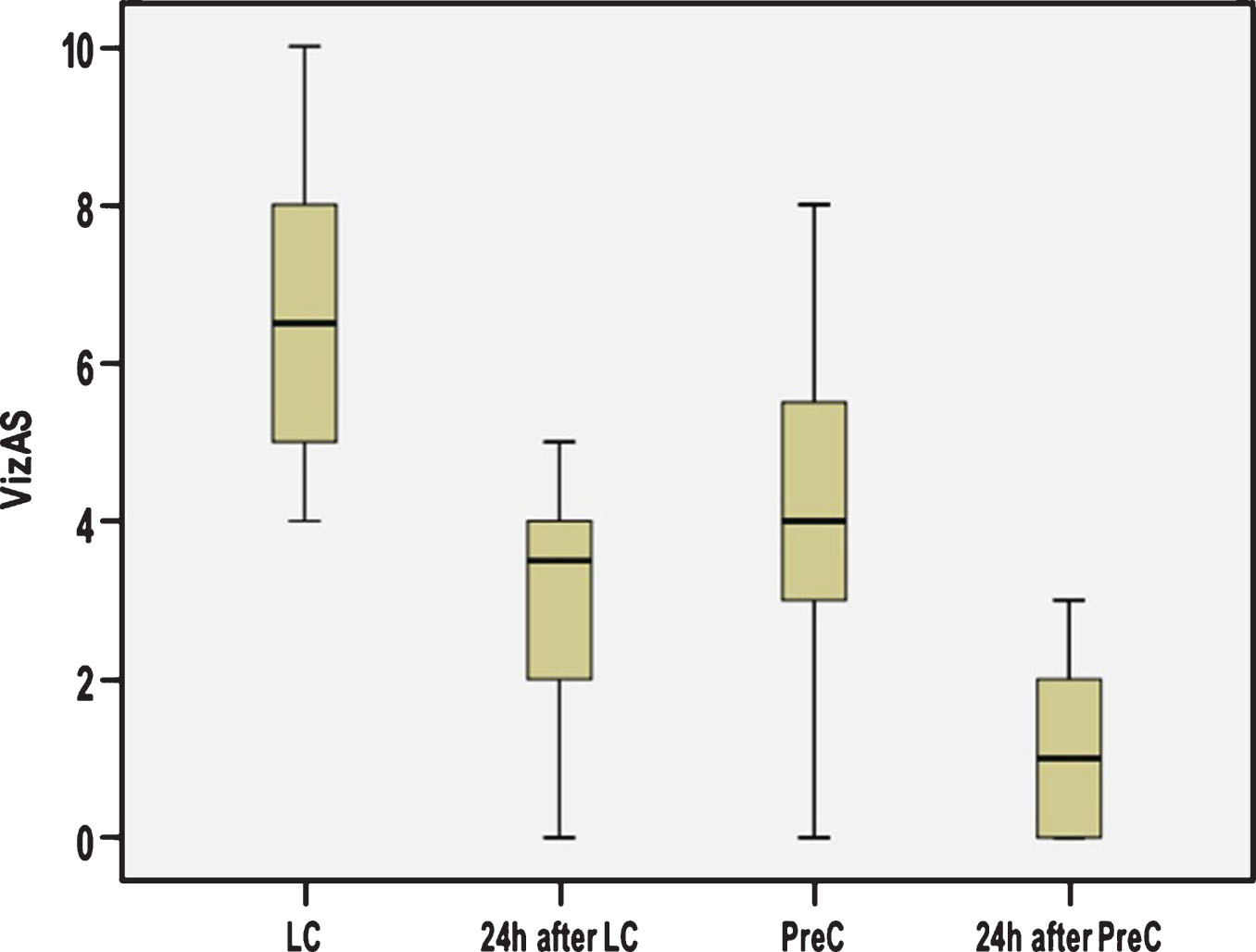
A significant difference can be seen in the PreC group, both after the operation (p = 0.014 M-Why test), and 24 hours later (p = 0.006 M-Why test, p = 0.005 Wilcoxon singed – rank test). Pain in PreC group was about 2–2.5 units lower at both times.
Laparoscopic technique has many advantages over conventional laparotomy: reduced hospitalization, reduced pain, scaring, and postoperative hernia, etc. Operation time is notably shorter, and recovery is faster, therefore it decreases costs. Pneumoperitoneum used for adequate visualization has some side-effects, too. Ischemic preconditioning is a concept that has been employed to avoid the harmful effects of ischemia-reperfusion injury in cardiac [11], liver [12] and reconstructive surgery [13]. To our knowledge no human study on preconditioning during pneumoperitoneum has been conducted, only in animal experiments. Some concerns have arisen that preconditioning is too lengthy for practical use.
The redox status of the body is tightly regulated and - as shown in the majority of the studies - returns to normal within 24 hours after surgery. In particular, in one study involving children, there was no change in markers of oxidative stress after either open or laparoscopic surgery [14]. Gutt and Schmandra examined abdominal blood flow at different intra-abdominal pressures (0–12 mmHg) caused by CO2 pneumoperitoneum in rats. They observed that by increasing the intra-abdominal pressure, blood flow will decrease and at 12 mmHg it becomes minimal. Hypoxia will evolve and abdominal organs will be damaged by reactive oxygen species [15]. Polat et al. performed laparoscopic cholecystectomy on 24 patients (12 male and 12 female). MDA and sulfhydryl-group concentration were measured and they observed that concentration of these markers had increased if they applied higher intra-abdominal pressure (10 vs. 15 mmHg) [16]. Based on the above mentioned two articles, in our study we set the IAP to 15 mmHg. Yilmaz et al. could reduce oxidative stress caused by pneumoperitoneum by using preconditioning in rats. They investigated oxidative stress markers and inflammatory cytokine concentrations in sham operated animals, after pneumoperitoneum and after preconditioning for 10 minutes. They concluded that increased intra-abdominal pressure could cause oxidative stress and preconditioning could reduce that. They used preconditioning before creating pneumoperitoneum at a pressure of 15 mmHg and observed that using preconditioning has a better protective effect than lower intra-abdominal pressure (10 mmHg) [17–20]. Athanasiadis D. et al. examined the effect of remote ischemic preconditioning (RIPC) in decreasing renal ischemia-reperfusion injury (IRI) during a suprarenal aortic cross-clamping porcine model. They found that repetitive short periods of cycles of ischemia-reperfusion (IR) ameliorate the biochemical kidney effects of IRI. RIPC groups presented significantly less impaired results compared to the IR group when evaluating MDA, cystatin C, CRP and creatinine levels. Between the two RIPC groups, RIPC II presented a better response regarding CRP, NGAL, TNF-α, MDA and cystatin C values. They concluded that remote IR and mainly repetitive short periods of cycles of IR ameliorate the biochemical kidney effects of IRI in a model of suprarenal aortic aneurysm repair. This fact also explains, that short repeated ischemia decreases ischemic-reperfusion injury [21]. In our pilot study we also found that considering GSH changes preconditioning could reduce the I-R injury. In animal studies subjects are mostly raised up under the same conditions. (same food, same temperature etc). Our data was heterogeneous, because in a human study it is impossible to assure that the patients are of the same age, weight, and fed similarly. Francisco Elano Carvalho Pereira et al. in their prospective study with twenty patients used RIPC after anaesthesia but before cholecystectomy. They evaluated the opioid analgesics consumption in the postoperative period, the presence of secondary mechanical hyperalgesia, the scores of postoperative pain by visual analogue scale, and the plasma interleukin (IL-6) levels. The total dose of morphine consumption in 24 hours was significantly lower in the RIPC group than in the control group (p = 0.0156). The intensity analysis of rest pain, pain during coughing and pain in deep breathing, showed that visual analogue scale (VAS) scores were significantly lower in the RIPC group compared to the control group respectively: p = 0.0087, 0.0119, and 0.0015 [22]. In our study pain in PreC group was about 2–2.5 units lower, and we could show a significant difference in the PreC group, both after the operation (p = 0.014 M-Why test), and 24 hours later (p = 0.006 M-Why test, p = 0.005 Wilcoxon singed – rank test). Leventi A. et al. used twenty-five female pigs in an experimental model. They used ischemic preconditioning for 15 minutes and 15-minute deflation before maintaining pneumoperitoneum. They concluded that ischemic preconditioning (IP) attenuated oxidative stress induced by intra-abdominal hypertension, mainly by increasing antioxydative capacity and the levels of protective mediators. It was proven that IP was effective, even in case of extremely high levels of intra-abdominal pressure [23]. Nesek-Adam et al. in their study demonstrated that ischemic preconditioning prevented hepatocyte injury and oxidative stress during CO2 pneumoperitoneum [24]. All our findings demonstrate that pneumoperitoneum has a negative effect which correlates with time and pressure. It seems that preconditioning can reduce the harm caused by pneumoperitoneum, and can reduce the pain as well. There are still many questions but there are a lot of investigations in progress around the world to answer this assumption [25]. The method of preconditioning may have some important clinical implications.
Conclusion
Laparoscopic surgery causes systemic ischemia and this ischemic effect can be confirmed by measuring serum antioxidant levels. In our pilot study we established a clinical model reproducible in any hospital. Based on the findings of our pilot study a larger scale multicentre trial can be initiated. For adequate results a more homogeneous patient population has to be selected (minimal co-morbidity, no chronic medication, normal BMI etc.) Based on our findings it can be stated that preconditioning made laparoscopic operations 10 minutes longer, but shortened hospitalization, and decreased pain. Considering cost-benefit aspect, preconditioning might be introduced into everyday clinical practice.
Footnotes
Acknowledgments
This work was supported by the Hungarian Science Research Fund OTKA-K108596. The present scientific contribution is dedicated to the 650th anniversary of the foundation of the University of Pécs, Hungary.