
Abstract
OBJECTIVE:
This study was aimed to develop microhemodynamic indices to evaluate the effectiveness of herbal medicine in diabetic tissues.
METHODS:
Male Sprague-Dawley rats were divided into four groups: normal control rats (Control), type 2 diabetic rats without (DM2) and with supplementation of alpha mangostin (DM2-MG) or curcumin (DM2-CUR). Alpha-mangostin or curcumin (200 mg/kg BW) were fed followed by i.p. injection of streptozotocin (STZ). Mean arterial pressure (MAP) and retinal blood flow (RBF) were measured and retinal flow resistance (RFR) was calculated. Three indices were developed to evaluate the effectiveness of herbal medicines in RFR-MAP diagram based on experimental data of MAP and RFR in type 2 diabetic rats. These indices are α, β, and γ where α is a ratio of reduction in MAP, β is a ratio of reduction in RFR increasing with MAP increase, and γ indicates a ratio of reduction in RFR.
RESULTS:
The elevated MAP and RFR and decreased RBF were observed in DM2 rats.
Interestingly, alpha-mangostin or curcumin supplementation significantly increased RBF while decreased MAP and RFR. Using α, β and γ indices, it was found that alpha-mangostin is more effective than curcumin in type 2 diabetic retina.
CONCLUSIONS:
These microhemodynamic indices may be useful to compare various herbal medicines in different tissues.
Keywords
Introduction
There are a number of natural plant products that prevent or improve diabetic vascular complication, including mangosteen and tumeric. Several studies have reported their various benefits in diabetes, but there are few studies to compare their effectiveness in the diabetic tissue of animal model. The main problem is the lack of an index available to compare the effectiveness of different natural products in different tissues.
In normal conditions, blood pressure changes along an arterial tree from artery, arteriole and capillaries to venules. Pressure drop is very large in the arteriolar regions, while it is usually small in the capillary network as single capillaries are short and numerous. However, the pressure drop in the capillary network may be elevated under some conditions when the number of single capillaries is reduced. In fact, several abnormalities in arterioles and capillaries in diabetes are observed from capillary to cellular and molecular level [1, 2]. Especially, at the arteriolar level, microaneurysms are formed or arterioles can become narrowed.
At the capillary level, capillary flows and pressure are heterogeneous or maldistributed leading to changes in density of functional capillaries. Fegan et al., have shown that the skin capillary pressure is elevated in hypertensive subject with type 2 diabetes. They suggested that increased capillary pressure may be caused by failure of protective mechanism to prevent transmission of the increased pressure to the capillary bed [3]. At the cellular level, endothelial cells can become dysfunctional with disruption of tight junction proteins leading to a breakdown of the blood barrier. These abnormal arterioles and capillaries affect the distributions of blood pressure in diabetes.
During elevation in mean arterial pressure (MAP) in diabetes, total flow resistance of the capillary network is increased in association with a reduction in capillary density due to abnormalities in arterioles and capillaries. Based on this concept, we develop hemodynamic indices to evaluate the effectiveness of natural products in retinal tissues. Using these indices, we compared the effectiveness of alpha-mangostin with that of curcumin on type-2 diabetic eye. Garcinia mangostana Linn. or mangosteen is known locally as “queen of all fruits” in Thailand. The active ingredients in the mangosteen fruit belong to a class of naturally occurring polyphenolic compounds, known as mangosteen xanthones (mainly including α-mangostin, β-mangostin, γ-mangostin) [4–6]. The mangosteen pericarp extracts possess a potent antioxidant capacity acting as a free radical scavenger that can boost body immunity and enhance its functions [5, 6]. Recently, research and clinical observations have confirmed that mangosteen has anti-inflammatory, anti-allergy, antioxidant, anti-tumor, anti-bacterial, anti-fungi, antiviral, and anti-malarial properties [4]. Curcumin, the yellow pigment extracted from the rhizome of Curcuma longa, is a principal curcuminoid. Curcumin extract has been shown to contain anti-inflammation and antidiabetic properties [7, 8].
The use of natural products is gaining acceptance among the people in the prevention of diabetic complications. However, up until now, there is a lack of index to evaluate the effectiveness of different natural products. Therefore, to evaluate the effectiveness of natural products in diabetic tissues we introduce microhemodynamic indices based on experimental data of mean arterial pressure (MAP) and retinal flow resistance (RFR) performed in high fat (HF) diet with low dose streptozotocin (STZ)-induced type 2 diabetic rats.
Materials and methods
We use low dose of streptozotocin-induced type 2 diabetic rats fed with high fat diet as an animal model, and use alpha-mangostin (alpha-MG) and curcumin (CUR) as natural products.
Alpha-mangostin (alpha-MG) preparation
The fruit mangosteen was collected from Kombang District, Chantaburi Province, Thailand in 2012. Mangosteen extract was prepared by extracting dried and pulverized fruit pericarp (0.5 kg) in 95% ethyl alcohol (3 L) at room temperature for 48 hours. The solvent was then removed to give a brownish residue. Water was then added and the resulting yellow solid was separated and dried under vacuum to give a crude extract (35 g). The alpha-MG was isolated and purified by repetitive column chromatography as previously described [9]. Its purity exceeded 95% as determined by HPLC [10]. The alpha-MG freshly dissolved in 1.0 ml of corn oil (Mazola, Malaysia) was given to rat at a concentration of 200 mg/kg BW.
Curcumin
The curcumin from Curcuma longa (Turmeric), a powder is a 95% standardized curcumin extract (Sigma-Aldrich, USA). The CUR at the concentration of 200 mg/kg BW of a rat was freshly dissolved in 1.0 ml of corn oil (Mazola, Malaysia) before use.
Induction of experimental type 2 diabetic rat model (DM2)
Rats were daily fed with high fat diet consisting of 40.0% fat, 35.0% carbohydrate, and 25.0% protein, with total calorific value of 5,085 kcal/kg diet (Plus Value Enterprise Co., Ltd, Thailand). After four weeks of dietary manipulation, the rats were intraperitoneally (I.P.) injected with streptozotocin (STZ; Sigma, St. Louis, MO, USA, 35 mg/kg, in 10 Mm sodium citrate buffer, pH 4.5). The normal control group received a regular diet which containing 4.5% fat, and 24.0% protein with a total calorific value of 3,040 kcal/kg diet for four weeks followed by an I.P. injection of 0.5 ml of 10 mM sodium citrate buffer, pH 4.5. Fasting blood glucose (FBG) level was determined one week after STZ or citrate buffer injection. The rats with a FBG ≥250 mg/dL were diagnosed as type 2 diabetes mellitus [11].
The natural products (alpha-MG and CUR) were supplemented from the first week after the injection of STZ. Control rat or diabetic rats were examined without or with supplementation of alpha-MG or CUR, separately (n = 6-7).
Animals and study design
Twenty- eight rats, 6 weeks old male Sprague-Dawley rats (National Laboratory Animal Centre of Salaya Campus, Mahidol University, Thailand), weighing 150–180 g were used in this study, which was approved by the ethical committee, Faculty of Medicine, Srinakharinwirot University, Thailand (identification number: EC 5/2015, SWU-MED). After a week adaptation and housing under a constant temperature of 20±2°C at the Animal Centre, Faculty of Medicine, Srinakharinwirot University, Bangkok. Thailand, the rats were randomly divided into four groups. The normal control group (CON) was fed a regular diet for 8 weeks. Type 2-diabetic group (DM2) induced by HF diet feeding combined with an I.P. injection of STZ was continuously fed with HF diet for 8 weeks. Type 2-diabetic supplemented with alpha-MG or CUR (DM2-MG and DM2-CUR) were prepared in the same way as the DM2 group, but they also received gavage feeding of alpha-MG (200 mg/kg BW/day) and CUR (200 mg/kg BW/day) for 8 weeks after STZ injection. To monitor all parameters, rats were anesthetized with an I.P. injection of sodium pentobarbital (60 mg/kg BW) and kept warm at 37C on a warming board. Their femoral veins and arteries were cannulated with polyethylene tubes for sodium pentobarbital administration to maintain anesthesia and to monitor arterial blood pressure respectively. The arterial pressure was measured using a pressure transducer (AD instrument, Power Lab system).
Hemodynamic measurements
Mean arterial pressure (MAP) was determined as:
Blood flow perfusion in the eye (retinal blood flow (RBF)) was measured using a laser-Doppler flowmetry (moorLAB monitor, Moor Instruments, England). A laser probe (0.1 mm) was used and put at about one mm from the surface of the tissue (cornea). The probe received laser-Doppler signals from blood cells flowing in capillaries of the tissue. By performing five different measurement points around the eye, we determined the mean of five points of RBF for each rat [11].
Retinal flow resistance (RFR) of the capillary network from arterioles to venues was calculated as:
Microhemodynamic indices
Three indices (α, β and γ) were conducted based on experimental data of MAP, RBF, and RFR in type 2 diabetic rats as follows:
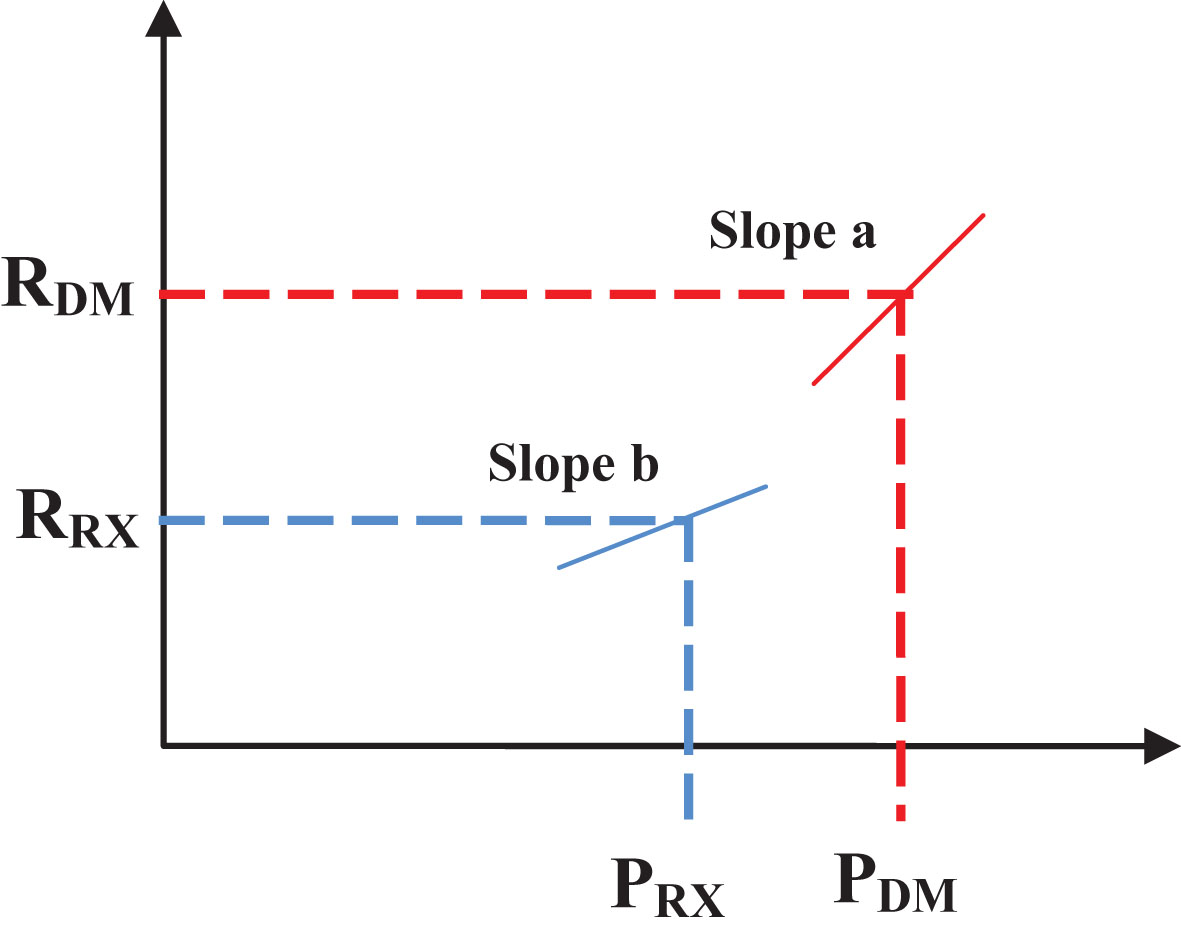
RFR-MAP diagram to evaluate the effectiveness of alpha-MG or CUR.
The α indicates the ratio of reduction in MAP, the β indicates a ratio of reduction in RFR increasing with MAP increase, and the γ indicates a ratio of reduction in RFR. Positive values of α, β and γ indicate improvement by supplementation of alpha-MG or CUR. The γ is related to increase in a number of single capillaries when an arteriolar condition is not altered.
Results are presented as mean±standard error of mean (SEM). Significant differences between groups were determined using one-way analysis of variance (one-way ANOVA), and differences between pairs of mean values were evaluated by Independent Samples t-test. Statistical analysis was performed using SPSS IBM Singapore Pte Ltd (Registration No.1975-01566-C). A value of p < 0.05 was considered statistically significant.
Results
Effects of alpha-MG and CUR on changes in mean arterial pressure (MAP), retinal blood flow (RBF), and retinal flow resistance (RFR)
The effects of alpha-MG or CUR on changes of MAP, RBF, and RFR are summarized in Table 1. Apparently, the MAP and RFR in DM2-rats was markedly higher than those of the Control rats, while the mean RBF was reduced significantly in the DM2 rats compared with those of the control rats (p < 0.001). Interestingly, supplementation of alpha-MG or CUR for 8 weeks had a great potential to significantly reduced MAP (p < 0.001 or p < 0.01, respectively) and RFR (p < 0.001 in both DM2-MG and DM2-CUR rats) compared with those monitored from untreated DM2 rats. On the other hand, the RBF levels in DM2-MG or DM2-CUR rats were significantly higher (p < 0.001) compared with those of untreated DM2 rats.
Mean values of mean arterial pressure (MAP), retinal blood flow (RBF) and retinal flow resistance (RFR) measured at 8 weeks after injection of citrate buffer and STZ in Control rats (Control), and diabetic rats without (DM2) and with supplementation of alpha-MG or CUR (DM2-MG and DM2-CUR, respectively)
Mean values of mean arterial pressure (MAP), retinal blood flow (RBF) and retinal flow resistance (RFR) measured at 8 weeks after injection of citrate buffer and STZ in Control rats (Control), and diabetic rats without (DM2) and with supplementation of alpha-MG or CUR (DM2-MG and DM2-CUR, respectively)
Values are means±SEM. PU: perfusion unit. *** indicates significant differences compared to the control rats at p < 0.001. ++, +++ indicates significant differences compared to the DM2 rats at p < 0.01, p < 0.001, respectively.
Collecting data of RBF against MAP and calculated RFR against MAP without and with supplementation of alpha-MG or CUR are plotted in Figs. 2 and 3, respectively. In DM2 rats increased MAP appeared to be associated with a reduction in the RBF (Fig. 2). In DM2-MG or DM2-CUR, the MAP was lower than those of DM2 rats. In addition, the values of RFR and MAP are also included in Fig. 3. The graph exhibits a good correlation between RFR and MAP. It was noted that in DM2 rats, RFR increased in association with the increase in MAP.
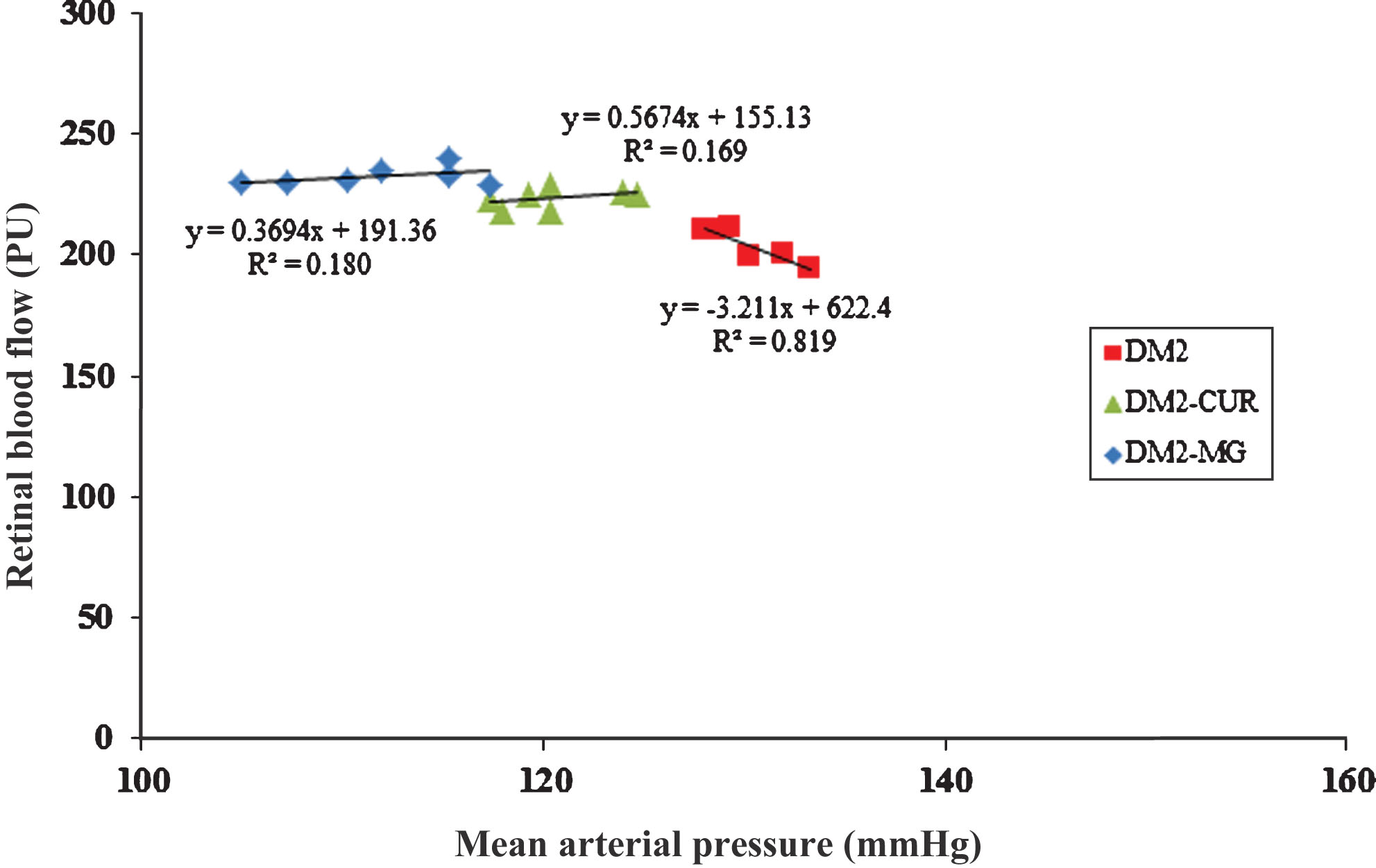
RBF against MAP measured in diabetic rats at 8 weeks after STZ-injection without (DM2) and with alpha-MG and CUR (DM2-MG and DM2-CUR supplementation). The linear regression equation are expressed as: y = –3.211x+622.4 (R2 = 0.819) in DM2 rats, y = 0.369x+191.3 (R2 = 0.180) in DM2-MG rats, y = 0.567x+155.1 (R2 = 0.169) in DM2-CUR rats, where x is mean arterial pressure and y is retinal blood flow, and R is correlation coefficient.
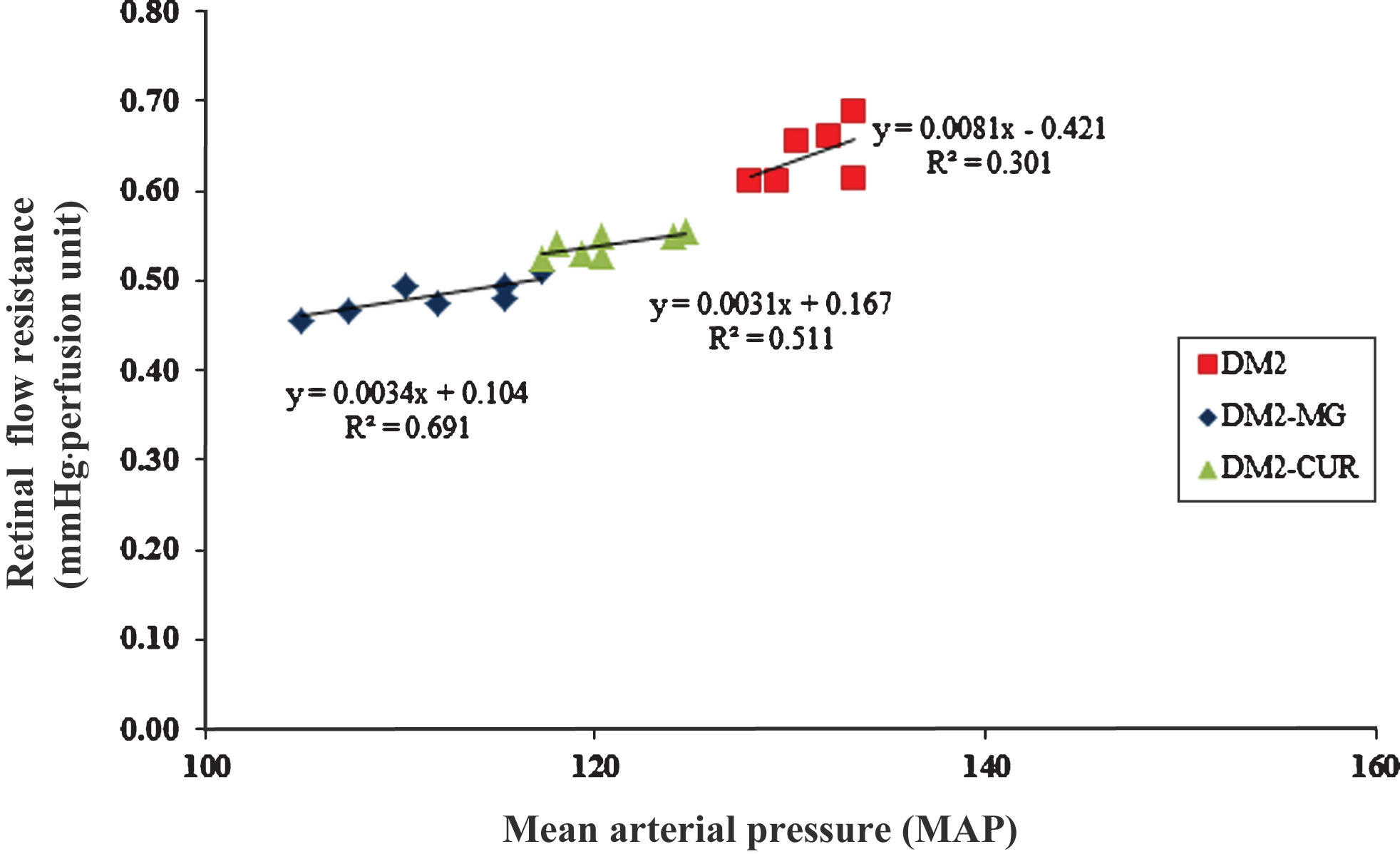
RFR against MAP measured in diabetic rats at 8 weeks after STZ-injection without (DM2) and with alpha-MG or CUR (DM2-MG and DM2-CUR) supplementation. The linear regression equation are expressed as: y = 0.0081x+0.421 (R2 = 0.301) in DM2 rats, y = 0.0034x+0.104 (R2 = 0.691) in DM2-MG rats, y = 0.0031x+0.167 (R2 = 0.511) in DM2-CUR rats, where x is mean arterial pressure and y is retinal flow resistance, and R is correlation coefficient. Note that the slope a in the RFR-MAP diagram corresponds to 0.0081, while slope b corresponds to 0.0034 in DM2-MG and 0.0031 in DM2-CUR.
To examine the effectiveness of alpha-MG and CUR, we evaluated three indices of α, β and γ based on data of RBF, MAP, and RFR and line slope data of DM2-MG or DM2-CUR groups in Table 1 and Fig. 3.
It is interesting to note that the values of α and γ under alpha-mangostin supplementation are much larger than those under CUR supplementation (Fig. 4A) while the β values remain almost equal under alpha-mangostin or CUR supplementation (Fig. 4B).
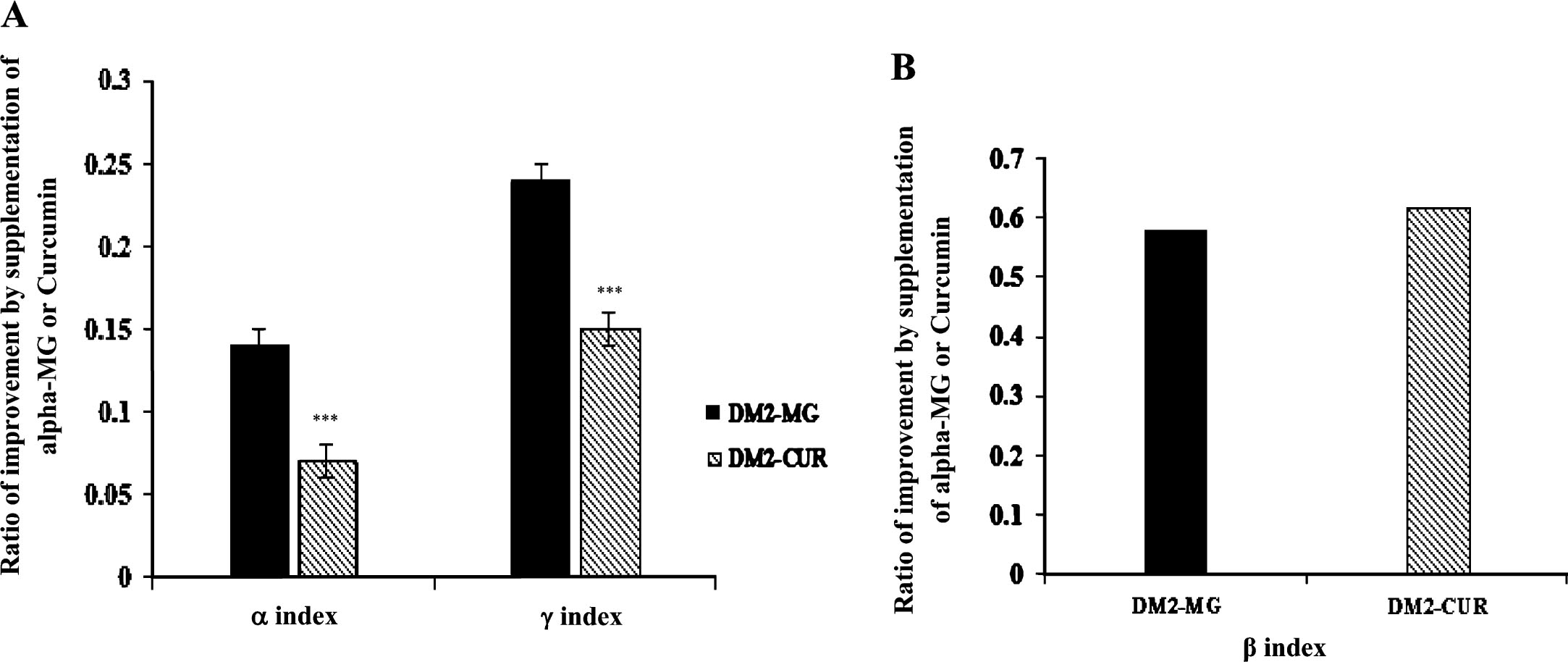
The ratio of improvement by supplementation of alpha-MG or CUR; α index and γ index (A) and β index (B) in diabetes retinal tissue. Values are presented as mean±SEM. *** indicates significant difference compared to the DM2-MG rats at p < 0.001.
In the present study, we developed three microhemodynamic indices to compare the effectiveness of various herbal medicines in diabetes. The present evaluation is based on the experimental relationship of RFR and MAP in HF-STZ-induced type 2 diabetic rats. As shown from the RFR-MAP diagram (Fig. 3), the RFR changes almost linearly with changes in MAP with and without supplementation of alpha-MG or CUR. These changes may be a reflection of changes of blood flow in the capillary network. In agreement with other studies [12–14], we found a significant decrease in the retinal blood flow in type 2 diabetic rats compared with those in type 2 diabetic rats supplementation with alpha-MG or CUR. Arend et.al., (1991) used scaning laser technique to analyse the perifoveal capillary circulation in patients with type1 and type2 diabetes. They demonstrated a reduction in capillary blood flow velocity and increasing foveal avscular zones. They have suggested that the reduction in blood flow velocity and increasing capillary avascular zones may lead to retinal tissues hypoxia and cause of capillary leakage and neovascularization [15]. In general, capillary density is an important factor to evaluating microcirculatory changes because it is a marker of disease severity. Several studies have demonstrated that diabetic retinopathy is caused by capillary degeneration, pericytes loss and development of avascular zones [15, 16]. Up to now, a number of intravital observations of organ microcirculation have reported perfused or non-perfused flow in the iris [17] or cerebral cortex [18]. Such heterogeneous flows in the capillary network are frequently associated with formation of neocapillary (or capillary angiogenesis) [19, 20].
Our concept of RFR is most convenient to consider changes in capillary density under diabetes. The RFR is elevated when the capillary density is reduced with capillary rarefaction due to non-perfused capillaries or loss of existing capillaries. The RFR also decreases when the capillary density is increased with increased number of perfused capillaries or formation of neocapillaries (angiogenesis). Capillary rarefraction indirectly reflects structural change in microvessels, which further increased peripheral vascular resistance and an increase in blood pressure [21–23]. In accordance with other studies, we have demonstrated that RFR increased significantly in type 2 diabetic rats, but this elevation was suppressed by supplementation of alpha-MG or CUR. These changes in RFR might be a reflection from those in the capillary density under the effect of alpha-MG or CUR. Assuming that arteriolar changes are negligibly small by alpha-MG or CUR, this elevated RFR and reduced capillary density might be due to capillary rarefaction in diabetes. A part from the beneficial effect of alpha-MG or CUR, Machado et al., have demonstrated that long-term physical exercise could reverses skeletal and cardiac muscle capillary rarefaction and impaired endothelium-dependent microvascular reactivity induced by diabetes in rats [24].
In our study, we compared two natural products: alpha-MG and CUR which have been used for clinical prevention of microvascular complications in diabetes. Curcumin is a polyphenol compound to exhibit antioxidant, anti-inflammatory, antitumorigenic, and antimicrobial properties. It may play roles in scavenging free radicals by redox activity and enhancement of cellular antioxidant system [25–29]. Several studies report the effects of reduction of adhesion molecules or leukocyte-endothelium [30]. Alpha-MG is a major active compound which is isolated from the dried skin of mangosteen [31–33]. Previous studies have demonstrated the anti-inflammatory and antioxidant effects of alpha-MG both in vitro and in vivo. For anti-inflammation and antioxidant properties in alpha-MG, much attention has been paid to its effectiveness on various diseases such as diabetes [34–36]. Alpha-MG or Curcumin is one of many natural plant products that have been believed to prevent or improve diabetic vascular complication. Several studies have reported their various benefits in diabetes, but there are few studies to compare their effectiveness in the diabetic tissue of animal model mainly because of lacking in an index to evaluate the effectiveness in different tissues for comparison of different natural products. The present three indices may be most useful to evaluate natural products in diabetes. It is more simple to use a tail-cuff technique for blood pressure measurement, combined with a laser-Doppler flowmetry for blood flow measurement. Laser Doppler flowmetry (LDF) has been widely used to measure blood flow perfusion in the tissue noninvasively. This noninvasive technique for assessment organ blood perfusion is an importance for studying microvascular alterations related to systemic and ocular diseases such as diabetic retinopathy. The LDF allows stable, continuous and repeatable measurements of organ blood perfusion to test pathological conditions and effectiveness of medicine [37, 38]. The obtained information (laser Doppler output) provides only the relative quantity related to blood flow-velocity (or flow-volume), perfusion unit (PU) is usually used.
Conclusion
The present study provides three indices (α, β and γ) to estimate the effectiveness of natural products in Asia. These may be useful for comparison of various Thai herbal medicines. It is future work to estimate and compare indices in different tissues (skin etc.) and herbal medicines.
Conflict of interests
The authors have no conflict of interests to report.
Footnotes
Acknowledgments
This study was supported by the Thailand Research Fund (TRF: DBG5480008).