
Abstract
In this review 14 studies were identified reporting the treatment strategy in 4891 patients with Critical Limb Ischemia (CLI) with the aim to investigate if the strategy of treatment of the first episode of CLI has changed during the last 15–20 years. A computer research has been performed on PubMed and Scopus databases on November 2016. The used terms for the investigation about studies evaluating the strategy of treatment of CLI at the first-time presentation, have been “critical leg ischemia”, “critical limb ischemia”, “critical lower limb ischemia” along with the terms “placebo”, “medical treatment” and/or “conservative” revascularisation, surgical revascularisation, endovascular revascularisation, hybrid revascularisation and primary amputation. Studies were included if they were either retrospective or prospective and reporting the rate of patients who underwent to any form of revascularization, conservative treatment and primary amputation. The one-year limb and life survival rates have been reported as major outcomes. The pooled rate of revascularization was 72.5% (95% CI 80-64.96) of which 54.5%, surgical, 38.3% endovascular and 7.1% hybrid. The bivariate regression of revascularisation procedures has been with not significant increase, from 68% in 1993 to 88% in 2015. The endovascular procedures have shown a significant increase of the trend, from 2% to more the 50% (p 0.007), while surgical and hybrid procedures have not. The pooled rate of conservative treatment was 18% (95% CI 11.6–24.5%) with a not significant increasing trend and primary amputation pooled rate was 8.7% (95% CI 12.0-5,4) with a significant decreasing trend (p 0.009). The one-year limb survival rate was 75,4% (95% CI 81.5-69.3%) and the life survival was 76%. (95% CI 85.4-66.1%) both with a not significant increasing trend. In conclusion, this review highlights how the treatment strategy of the first CLI manifestation has changed over the last 15–20 years. It has shown an increase of the rate of revascularization procedures, particularly for endovascular and a significant reduction of the rate of primary amputations. The rate of patients treated conservatively appears to be unchanged and maybe influencing the rate of limb and life survival, that have remained unchanged.
Introduction
Critical limb ischemia (CLI) is the most advanced stage of peripheral arterial disease associated with macro but also with microcirculatory as well as with rheological disorders [1–3]. CLI carries a high rate of limb amputation and cardiovascular mortality [1]. The limb revascularisation is considered the first line of the treatment strategy for CLI because it has significantly reduced the rate of limb amputations and mortality [1, 4].
The primary limb amputation is indicated in those patients with unreconstructable CLI, and limb and/or life-threatening skin lesions. But, for not revascularizable patients with a still viable limb and not life-threatening conditions, conservative treatments based on wound management associated with prostanoids, pain drugs and best medical treatment of atherosclerosis risk factors, are often indicated [1, 6].
According to the TASC documents published in 2000 and in 2007, the rate of patients treated with revascularisation at their first episode of CLI was 50%, while primary amputations or conservative treatment were indicated in the 25% each [1].
During the last 15–20 years, several new techniques and procedures of revascularisation (endovascular, surgery, hybrid) and of anaesthesiology have been developed. This progress should have permitted the revascularisations to those patients who were not good candidates for revascularisation in the past, such as those with infrapopliteal lesions or extensive femoropopliteal disease [7]. But data coming from real clinical life and from literature do not seem to confirm this trend showing that the rate of patients treated with conservative/medical treatments have remained unchanged than past decades [8]. This study wants to analyse the rate of limb revascularisation, conservative treatments and primary amputation at first episode of CLI with the aim to investigate if the strategy of treatment of CLI has changed during the last two decades knowing. The results of this observation could be of help in planning future studies for the treatment of CLI patients.
Materials and methods
A computer research has been performed on PubMed and Scopus databases analysing a time spam from January 1990 to November 2016. As the definition criteria of CLI were expected to be heterogeneous, the used terms for the investigation about studies evaluating the strategy of treatment of CLI at the first-time presentation, have been “critical leg ischemia”, “critical limb ischemia”, “critical lower limb ischemia” along with the terms “placebo”, “medical treatment” and/or “conservative” revascularisation, surgical revascularisation, endovascular revascularisation, hybrid revascularisation and primary amputation. One hundred and ninety-seven studies were found. After scrutiny the studies were selected only if reporting together the rates of patients that were selected for any form of revascularization, conservative treatment, primary amputation and at least one year of limb and life survival. Moreover, studies were accepted if they were either retrospective or prospective and included consecutives or not consecutive patients. With these criteria, 14 studies have been selected to study the trends that revascularisation, conservative treatments or primary amputations have had in the treatment of patients at their first episode of CLI.
Data on patient demographics and comorbidities were extracted from each study.
Statistical analysis has been performed using the Med Calc. Version 12.3.0–©1993-2012 Med-Calc Software bvba. The results were presented as pooled proportions (%) with 95% confidence interval (95% CI). Analysis of distribution and of the variant was calculated. A P < 0.05 was considered statistically significant.
Results
Fourteen studies were identified reporting the treatment strategy in 5084 patients with CLI from 1993 to 2015 [9–22]. The Patient demographics, risk factors, co-morbidities and mode of presentation are reported in Table 1.
Patient demographics, risk factors, co-morbidities and mode of presentation
Patient demographics, risk factors, co-morbidities and mode of presentation
The pooled rate of revascularization was 72.5% (95% CI 80-64.96) of which 54.5% surgical, 38.3% endovascular and 7.1% hybrid. The conservative treatment has shown a pooled rate of 17.1% (95% CI 10.4–23.8%) and the rate of primary amputation was 8.7% (95% CI 12.0-5,4) (Table 2).
Pooled rates of treatments and one year limb-life survival of CLI 1993–2015
The bivariate regression has shown a not significant increase for the cumulative revascularisation procedures from 68% in 1993 to 88% in 2015. But the endovascular procedures have shown a significant increase along the years from 2% to more the 50% (p 0.007), while surgical and hybrid procedures have not. The conservative treatment has a not significant increasing trend from 1993 to 2015 while the primary amputation had a significant decreasing trend (p 0.009) in the same time spam. The one-year limb survival rate was 75,4% (95% CI 81.5-69.3%) and the life survival was 76% (95% CI 85.4-66.1%) both with a not significant increasing trends (Fig. 1).
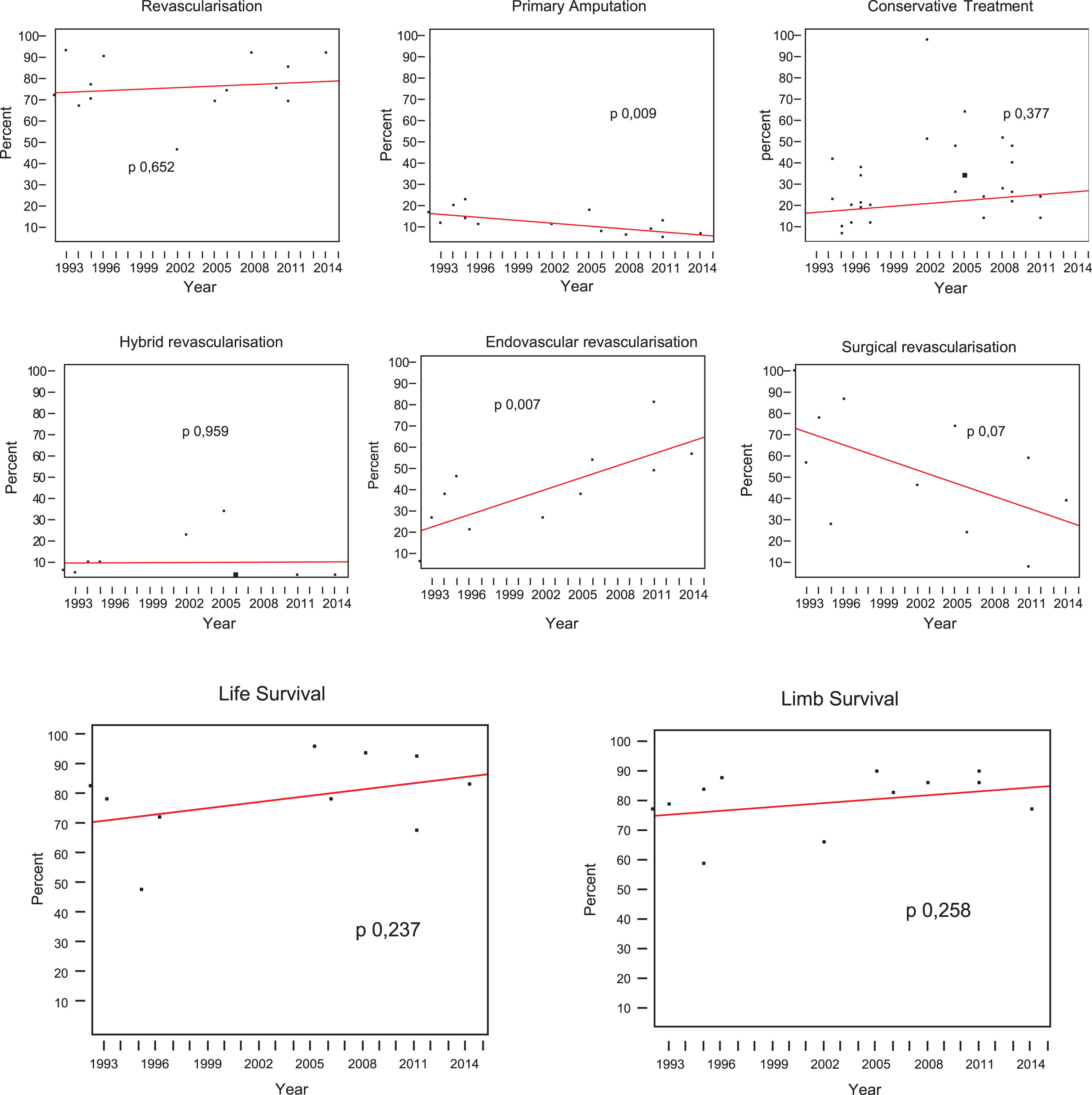
Bivariate regression of main treatment used for CLI from 1993–2015.
This review highlights how in the time span between 1993 and 2015, the strategy of treatment of the first episode of CLI has changed.
In comparison with TASC documents data published in 2000 and 2007, there have been an increase of the revascularization procedures from 50% to 72%, and a dramatic decrease of the primary amputations, from 25% to less than 10%. The proportion of patients treated with conservative/medical therapy have shown a slight reduction from 25% to 18% [1].
The rate of revascularisation was more than 80%, in some single centre study with more aggressive approach [10, 22]. The rates of multi centre studies was lower, 60/70% and 14 may represent the average patient care [9, 16].
Endovascular procedures have a significant increase more than the other revascularisation procedures, from 2% in 1993 to 77% in 2012 [9, 20]. This datum supports the significant drop of primary amputation rate reported in this study and confirms the great impact of the percutaneous transluminal angioplasty (PTA) and of the other endovascular procedures on the CLI management. Primary bypass surgery is now recommended as first line for patients with life expectancy of more than 2 years because of the improved durability of the reconstruction [23]. However, it should be noted that although the significant increase of limb revascularisation and significant reduction of primary amputations, the limb and life survival did not show significant changes from TASC. Norgren et al. reported 1 a one-year limb amputation rate of 30% and the mortality 25%, that is quite like rate reported in this review [1].
Perhaps these outcomes are due to the huge number of conservatively treated patients that have been included in the assessment of the limb and life survival outcomes. Most of studies have reported the results of the outcomes of medical treated patients with other treatments outcomes. It is likely that if the outcome data were selected for each type of procedure performed, the rate of limb and life survival could be better than that observed.
However, it is remarkable that despite the huge progress of revascularisations techniques, still one fifth of the patients with CLI has been treated conservatively with an increasing trend from 1993 to the more recent years, although the study of 2015 reports a lower rate of 9%, [22]. Two recent studies confirm this observation. Baser in 2013, in a Medicare population data study reported that the revascularisation was offered only to 34% of patients at their first episode of CLI. He concluded that it was reasonable to guess that in the real life, more than 50% were offered to conservative treatment [24] Biancari in 2014 reported in 2144 legs with CLI a 20% rate of conservative treatment with an increasing trend along with the mid-date of the studies included [8].
Despite the increasing trend this review underlines that patients conservatively treated do not have attention by the authors, although they represent a large part of the entire CLI population.
In the studies selected there are scarce details about their epidemiology, criteria of selection for conservative treatment and kinds of treatment utilised.
The nature of CLI in the studies chosen for the most was tissue loss, 70% (Table 1). This had significantly impacted on the choice of procedure and on the limb outcomes.
As far as it was possible to evaluate, the reasons for a conservative treatment were: the poor general health, the wheelchair bound with no prospect of mobilization, patients who were non-ambulatory or with limited life expectancy and patients who failed to give their consent to an invasive treatment in 3 studies (92 patients 11.2.4%) [15, 21]; (375 patients, 45.8%) [12, 16–22]. However, 5/14 studies of this review, (351 patients 42.9%) did not report the criteria that determined the choice of conservative treatment [9, 19]. It should be noted that only one study (118 patients 14.4%) reported detailed hemodynamic analysis of the lower limb arterial lesions [22] Table 3.
Motivations for conservative treatment
The conservative treatment was frequently based on wound management associated, prostanoids, pain drugs and the best medical treatment of atherosclerosis risk factors.
Consequently, in the studies considered it was difficult to evidence differences in the limb and patient survival rates between those undergoing revascularization (both surgical and endovascular) compared to those treated conservatively. This in our opinion could be a confounding variable. Perhaps most of the patients treated conservatively, likely either had no revascularization options or perhaps were non-ambulatory and thus not candidates for revascularization. The decrease of the primary amputation rate with the limb salvage not improved could mean that patients with limbs that were unsalvageable underwent revascularization. Despite the conservative treatment has shown excellent results in limb and life survival in selected CLI patients [5, 25] lower limb revascularization should be regarded as the treatment of choice in CLI as it may achieve leg salvage rates at one year higher than 80% [4].
Conservative treatment represents one of the major workload in terms of assistance and economic resources for vascular units [26].
Maybe a greater attention to the epidemiology of patients considered not revascularizable may provide useful data for understanding the natural history of the CLI and a better selection for appropriate treatments.
In the more recent years many studies have claimed significant success of autologous bone marrow-derived cell therapy in patients with no option critical limb ischemia. The available data about “cell therapy” suggest one-year limbs survival around 70–80% [27–30]. But it should be emphasized that these therapies are all investigational and no proven benefit has yet been achieved. Improved epidemiological data about this population will be of help in planning this new field of clinical research.
The incidence of CLI in subjects >65 years old may range from 113 to 200 cases per 100,000 population per year è. These data suggest that in the next decades there will be probably a dramatic increase of CLI particularly in elder population. There will be the need of prompt and effective revascularization and medical treatment to increase limb and life survival more than actual results and avoid economic consequences.
It is difficult to identify trends from a review of 14 papers published over a 22 years period. The sample size is too small, but this review aims to address the attention of the readers toward the actual situation of the treatments of CLI patients that seem not only about the revascularisation procedures.
Maybe registry or large administrative databases, that might more accurately capture the full spectrum of treatment, rather than series that may be more slanted to invasive treatments could avoid potential selection bias as in this paper.
In conclusion, this review highlights how the treatment strategy of the first CLI manifestation has changed over the last 15–20 years. It has shown an increase of the rate of revascularization procedures, particularly for endovascular and a significant reduction of the rate of primary amputations. The rate of patients treated conservatively 1 appears to be unchanged and maybe influencing the rate of limb and life survival, that have remained unchanged despite the increase of revascularisation procedure.
More observations about epidemiological data could be of help for the understanding the natural history of CLI and in planning future trials for improve the limb and life survival. We hope this study can help to focus more on this issue.
Disclosure
None.