
Abstract
OBJECTIVES:
To compare the diagnostic performance of conventional strain elastography (CSE) and acoustic radiation force impulse (ARFI) induced SE for qualitative assessment of breast lesions and evaluate the additional value of the two techniques combined with Breast Imaging Reporting and Data System (BI-RADS) respectively for the differentiation of benign and malignant breast lesions.
METHODS:
In a cohort of 110 women, the conventional ultrasound (US) features and the elasticity scores of CSE and ARFI induced SE were recorded. The diagnostic performances of BI-RADS, elastography and BI-RADS plus elastography were evaluated, including the area under the receiver operating characteristic curve (AUROC), sensitivity, specificity and accuracy.
RESULTS:
Pathologically, there were forty-eight malignant and sixty-two benign breast lesions in the final analysis. The AUCs for CSE and ARFI induced SE are similar (CSE, 0.807; ARFI induced SE, 0.846; p > 0.05), however, the specificity of the latter method was significantly higher than that of CSE (83.9% vs. 58.1%, p = 0.004) in differentiating breast lesions. The accuracy and specificity of BI-RADS plus ARFI induced SE (84.5%, 80.6%, respectively) were significantly higher than BI-RADS alone (73.6%, 54.8%, respectively) and BI-RADS plus conventional SE (72.7%, 56.5%, respectively), respectively (p < 0.05) without loss of sensitivity.
CONCLUSIONS:
Our study showed that BI-RADS plus ARFI induced SE had a better diagnostic performance in the diagnosis of breast lesions in comparison with BI-RADS alone or BI-RADS plus CSE.
Introduction
Breast cancer is one of the leading causes of cancer mortality worldwide among women [1]. Mammography screening is the standard imaging modality to diagnose breast masses in clinical field, however, it is exposed to radiation and it might be influenced by dense breast tissue [2]. Therefore, conventional ultrasound (US) has been regarded as an important complementary method for mammography in depicting breast lesions due to its advantages of convenience, cost-effectiveness and wide availability [3].
The Breast Imaging Reporting and Data System (BI-RADS) was proposed by the American College of Radiology to standardize the breast scanning process and facilitate understanding between radiologists and clinicians based on the conventional US characteristics [4]. However, it would be helpful for radiologists to evaluate the breast lesion aside from morphologic features. As a novel technique, US elastography technique is capable of offering additional clues to assess the nature of the target area by providing the tissue elasticity [5–11]. In terms of the guidelines and recommendations for US elastography presented by the World Federation of Ultrasound in Medicine and Biology (WFUMB), elastographic technology includes strain imaging and shear wave imaging. Strain imaging is classified into conventional strain elastography (CSE) (i.e. elasticity imaging, EI) and ARFI induced SE (i.e. virtual touch imaging, VTI) according to different excitation methods. CSE requires manual compression to be exerted on the tissue to estimate the stiffness. In contrast, tissue is mechanically excited by using free-hand short-duration acoustic pulses to generate localized tissue displacement during ARFI induced SE examination [12, 13]. Both strain imaging methods are effective in differentiating benign and malignant lesions as a qualitative method [14–19]. On the other hand, US strain imaging has been proven to significantly reduce the false-positive rate and decrease unnecessary biopsies of breast lesions by combining with US BI-RADS category in comparison with BI-RADS alone [19–23]. However, Xu et al. [24] suggested that CSE was more operator dependent, subject to external compression and questionable reproducibility in thyroid nodules in comparison with ARFI induced SE. To our knowledge, there have been few studies concerning the diagnostic performances of these two different SE techniques in assessing breast lesions in the same population.
Therefore, the aim of this study was to compare the diagnostic performance of CSE and ARFI induced SE for qualitative assessment and evaluate the additional value of the two techniques combined with BI-RADS respectively for the differentiation of benign and malignant lesions in breasts.
Materials and methods
Patients
This retrospective study was approved by the institutional ethics committee, and patients’ informed consents were waived due to retrospective nature of this study. From November 2016 to May 2017, 157 breast lesions in 149 consecutive women were examined with conventional US and elastography. The exclusion criteria for the patients were as follows: (a) breast lesions lack of US or elastography data (n = 14); (b) breast lesions without pathological confirmation by core-needle biopsy or surgery (n = 20); (c) women underwent previous treatment before the examination (n = 5); If multiple breast lesions were present, the most suspicious lesion on BI-RADS category was enrolled in the study; If the lesions with same BI-RADS category, the largest one was included (n = 8). Finally, 110 breast lesions in 110 women were included in our study in total (Fig. 1).

Flowchart of breast lesions selection. IDC = invasive ductal carcinoma; DCIS = ductal carcinoma in situ.
Breast conventional US and elastography examinations were performed with the same Siemens S3000 US scanner (Siemens Medical Solutions, Mountain View, CA, USA) equipped with a linear array transducer (9L4, multi-frequency, 4–9 MHz; Siemens Medical Solutions) by 1 of 2 radiologists with 6 and 5 years of experience in breast US, respectively. In terms of the breast US examination guideline of the American Institute of Ultrasound in Medicine [25], the transverse and longitudinal conventional US images for each breast lesion were obtained with patients in supine position. Then, in CSE application, light pressure was exerted on the location of the lesion and a region of interest (ROI) was placed to cover the lesion and adequate surrounding tissue as well. The image of CSE was displayed with color-code map in terms of the degree of strain in the ROI with a scale from red (softest component), to green (intermediate component), to blue (hardest component). For acquirement of high-quality ARFI induced SE gray-scale images, the transducer was fixed and kept perpendicular to the skin as far as possible by slight pressure with patients holding their breath for 5 seconds. A ROI was adjusted according to the lesion size in order to include the lesion and sufficient surrounding tissue. The ARFI induced SE image is seen as a grayscale image, in which dark indicated hard tissue and bright indicated soft tissue. Blind to any patients’ clinical information, two independent radiologists with more than 5 years of experience in breast US were asked to review all the images. All the lesions were analyzed in 2 orthogonal planes at least. The B-mode US features were recorded as following: maximum diameter, lesion depth (measured as the distance from the skin to the shallowest margin of the mass), lesion position (upper outer quadrant/upper inner quadrant/lower outer quadrant/lower inner quadrant), margin (circumscribed/non-circumscribed), shape (regular/irregular), internal echo (evenly/unevenly), calcification (present/absent), posterior features (none/posterior shadowing), orientation (parallel/non-parallel). Then, the BI-RADS categories of breast lesions were recorded depending on conventional US features [26]: category 1, negative; category 2, benign; category 3, possibly benign; category 4a, lowly suspicious; category 4b, moderately suspicious; category 4c, highly suspicious; category 5, highly suggestive of malignancy. We viewed the BI-RADS category 4 and 5 lesions as malignant and BI-RADS category 3 as benign. Color Doppler flow patterns were defined as follow: Type I, absent vessels; Type II, vessels in rim; Type III, rare internal vessels with or without peripheral ones; Type IV, internal vascularity with or without peripheral vessels. CSE were classified and recorded according to a 5-point by Tsukuba scoring system [27]: score 1, the entire lesion was green; score 2, the lesion has a mosaic pattern of green and blue; score 3, the peripheral part of the lesion was green, and the central part was blue; score 4, the entire lesion was blue, but its surrounding area was not covered; score 5, the entire lesion and its surrounding area were both blue. ARFI induced SE images were scored in terms of a 6-point scoring system proposed by Zhang et al. [28]: score 1, the lesion was predominantly white; score 2, the lesion was predominantly white with few dark portions; score 3, the lesion was equally white and black; score 4, the lesion was predominantly black with a few white spots; score 5, the lesion was almost completely black; and score 6, the lesion was completely black.
Statistical analysis
Statistical analyses were conducted by using SPSS version 13.0 (IBM corporation, Armonk, NY) software. The continuous quantitative data were expressed as the mean±standard deviation (SD) and range, if normal distribution was achieved, and were analyzed by independent t-tests. The categorical data were analyzed by Chi-square test or Fisher’s exact test if necessary. Regarding pathologic results as the reference standard, the diagnostic performances of CSE and ARFI induced SE were assessed by receiver operating characteristic (ROC) curves in evaluating breast lesions. The optimal cutoff values were obtained, when the Youden index (sensitivity+specificity-1) was maximum. If the CSE score was greater than or equal to the optimal cutoff value, the BI-RADS category 3 lesions were upgraded to BI-RADS+CSE category 4a; If the CSE score was less than the optimal cutoff value, the BI-RADS category 4a lesions were downgraded to BI-RADS+CSE category 3. The same principle was applied in the combination of BI-RADS and ARFI induced SE. The sensitivity, specificity, accuracy, positive predictive value (PPV), negative predictive value (NPV) of BI-RADS alone, BI-RADS plus CSE and BI-RADS plus ARFI induced SE were calculated and compared. The Z-test was performed to compare the AUC. The McNemar test was used to compare the sensitivity, specificity, accuracy. The Chi-square test was plotted to compare the PPV and NPV. A p-value <0.05 was considered statistically significance.
Results
Pathologic diagnoses
Of the 110 breast lesions, the final pathologic diagnoses confirmed that 62(56.4%) were benign (Figs. 2 and 3) and 48(43.6%) were malignant (Figs. 4 and 5). The 62 benign lesions included fibroadenoma (n = 44, 71.0%), adenosis (n = 8, 12.9%), papilloma (n = 8, 12.9%) and phyllodes (n = 2, 3.2%). The 48 malignant lesions included invasive ductal carcinoma (n = 39, 81.2%), ductal carcinoma in situ (n = 7, 14.6%), invasive lobular carcinoma (n = 1, 2.1%) and mucinous carcinoma (n = 1, 2.1%). The histopathological results confirmed by both surgery and biopsies are regarded as the gold standard in our study.
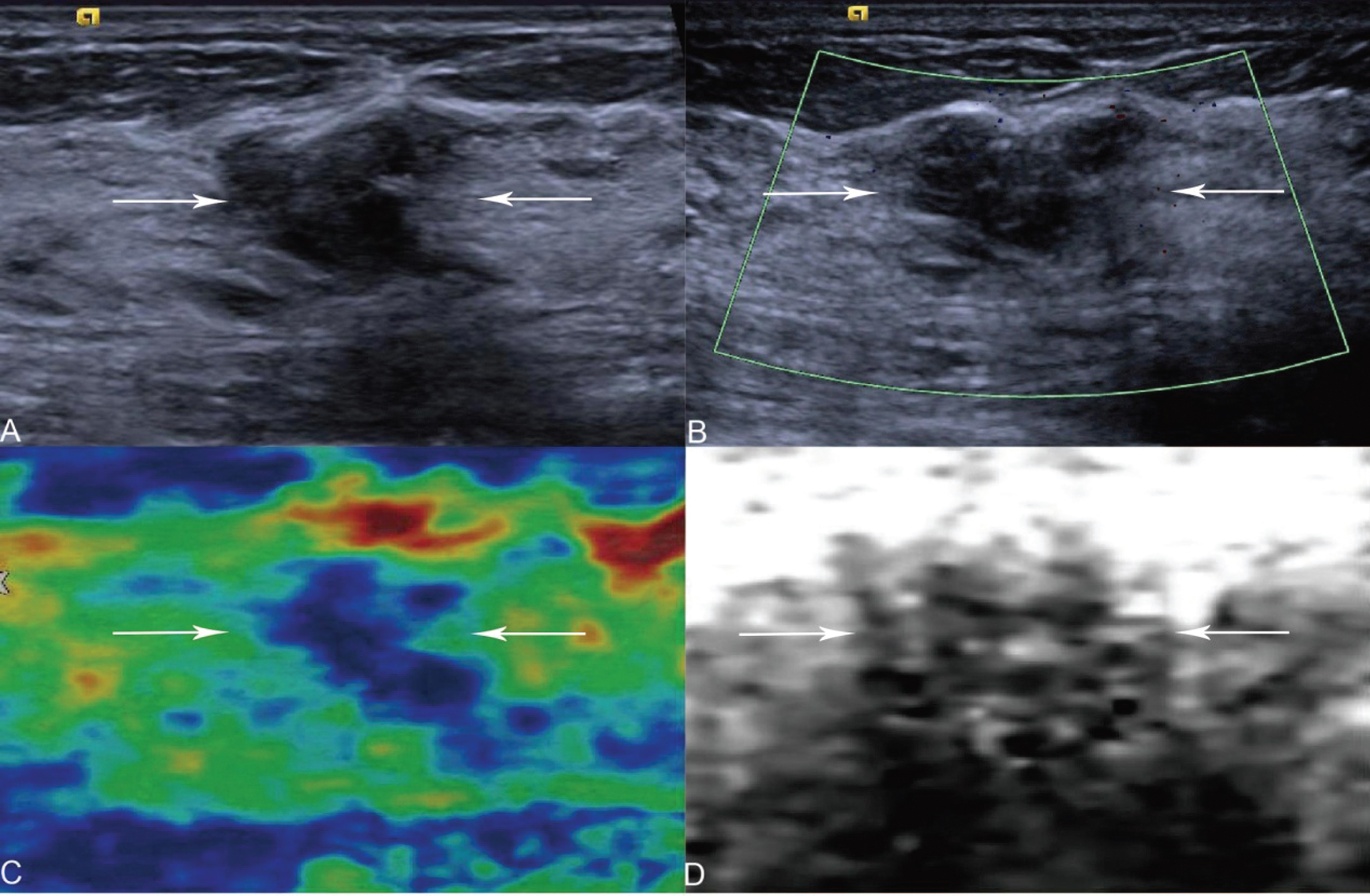
A 37-year-old woman with breast fibroadenoma. (A) A solid, hypo-echogenic, irregular shaped, non-circumscribed lesion (arrows) is shown on US, which is classified as BI-RADS category 4a. (B) The color Doppler flow patterns of the lesion (arrows) is Type I. (C) The CSE score of the lesion (arrows) is 2, downgrading from BI-RADS category 4a to BI-RADS+CSE category 3. (D) The ARFI induced SE score of the lesion (arrows) is 2, downgrading from BI-RADS category 4a to BI-RADS+ ARFI induced SE category 3.
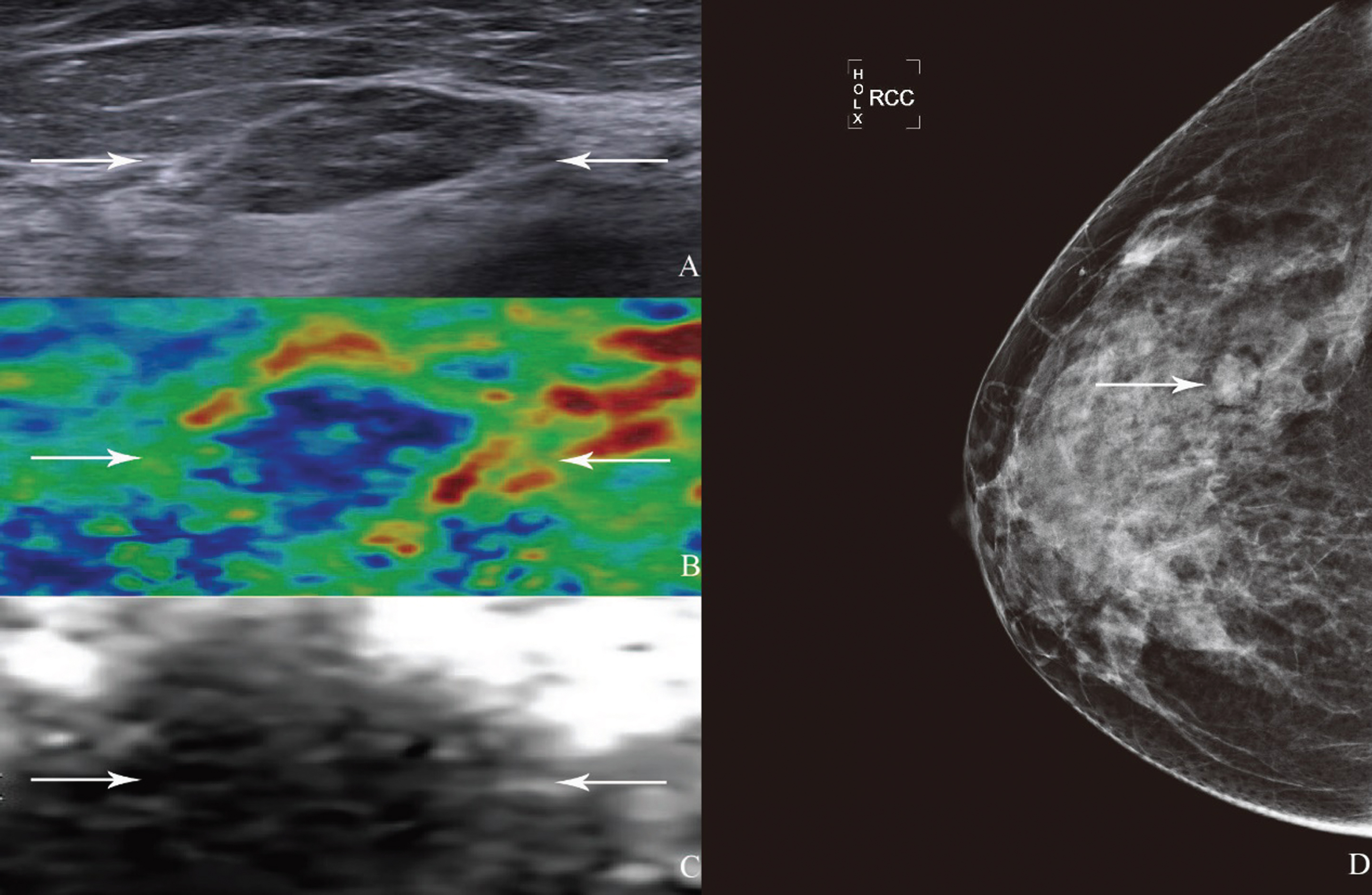
A 41-year-old woman with breast fibroadenoma. (A) A solid, hypo-echogenic, regular shaped, circumscribed lesion (arrows) is shown on US, which is classified as BI-RADS category 3. (B) The CSE score of the lesion (arrows) is 2. (C) The ARFI induced SE score of the lesion (arrows) is 4. (D) Mammography displayed an isodensity lesion with non-circumscribed margin in the upper outer quadrant of the right breast (arrows), which is classified as BI-RADS category 3.
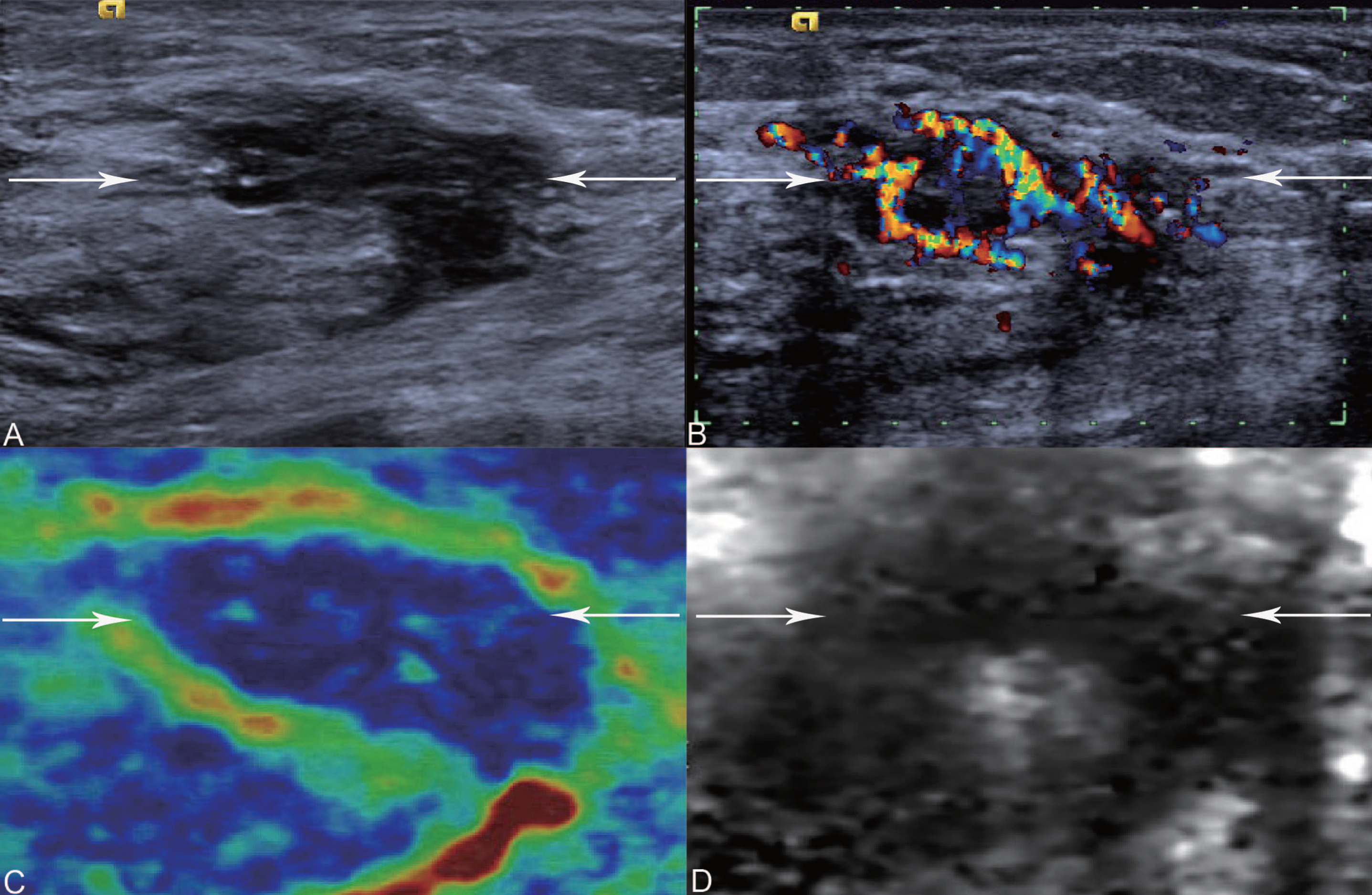
A 45-year-old woman with breast ductal carcinoma in situ. (A) A solid, hypo-echogenic, irregular shaped, non-circumscribed lesion (arrows) is shown on US and micro-calcifications are found in the lesion (arrows), which is classified as BI-RADS category 4c. (B) The color Doppler flow patterns of the lesion (arrows) is Type IV. (C) The CSE score of the lesion (arrows) is 4. (D) The ARFI induced SE score of the lesion (arrows) is 4.
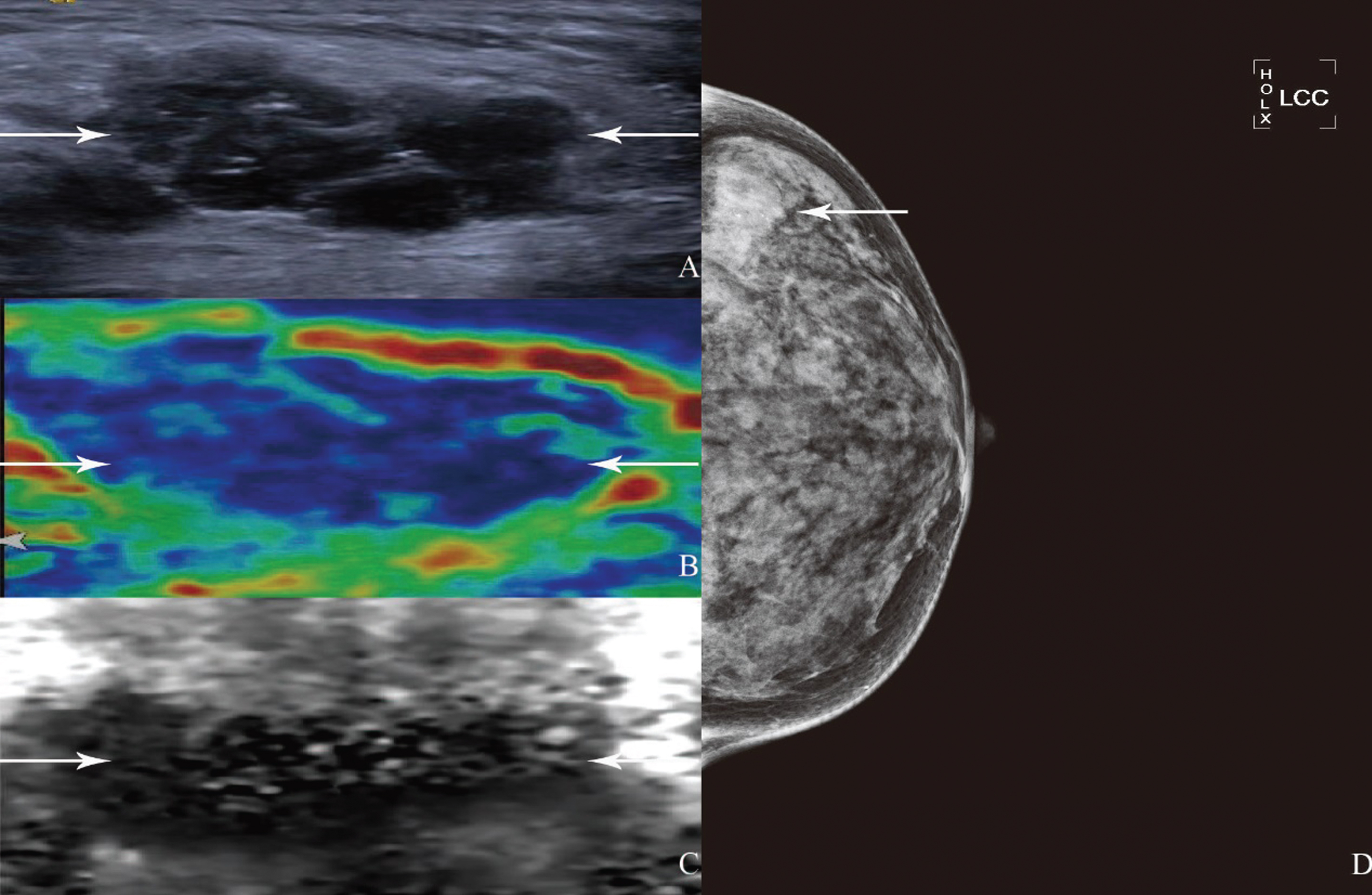
A 44-year-old woman with breast invasive ductal carcinoma. (A) The hypo-echoic lesion with irregular shape, parallel orientation, relatively circumscribed margin, micro-calcification and internal vascularity is classified on the BI-RADS as 4c on B-mode ultrasound. (B) The CSE score of the lesion (arrows) is 4. (C) The ARFI induced SE score of the lesion (arrows) is 3. (D) Mammography revealed a high density lesion with spiculated border in the upper outer quadrant of the left breast (arrows), which is classified as BI-RADS category 4b.
The mean age of patients with malignant breast lesions was significantly higher than those with benign breast lesions (52.7years±10.3 vs. 38.5years±12.8) (p < 0.001) and the maximum depth of malignant breast lesions was significantly higher than that of the benign ones (7.0 mm±3.4 vs. 5.4 mm±3.8) (p < 0.05) (Table 1). In terms of conventional US features, non-circumscribed margin, irregular shape, calcification, non-parallel orientation and vascularity were more frequently found in malignant breast lesions (all p < 0.001) (Table 1). In elastography examinations, CSE score≥3 and ARFI induced SE scores of 4–6 were observed more often in malignant lesions (all p < 0.001) (Table 1).
The characteristics of patients, US and elastography features of breast lesions
The characteristics of patients, US and elastography features of breast lesions
Unless otherwise indicated, data are numbers of lesions, with percentages in parentheses. †Data are mean±standard deviation, with ranges in parentheses. *Indicates a significant difference. CSE = conventional strain elastography; ARFI = acoustic radiation force impulse; SE = strain elastography.
Using ROC analysis, we determined that CSE score ≥ 3 was the optimal cutoff value (Youden index = 0.435), with a sensitivity of 85.4% (41 of 48), specificity of 58.1% (36 of 62), accuracy of 70.0% (77 of 110), PPV of 61.2% (41 of 67) and NPV of 83.7% (36 of 43). Also, we found that ARFI induced SE score ≥ 4 (Youden index = 0.589) was the optimal cutoff value for the ARFI induced SE, achieving a sensitivity of 75.0% (36 of 48), a specificity of 83.9% (52 of 62), an accuracy of 80.0% (88 of 110), PPV of 78.3% (36 of 46), NPV of 81.3% (52 of 64). The AUC of ARFI induced SE (AUC = 0.846) showed similar with CSE (AUC = 0.807) (p = 0.549). However, the specificity of ARFI induced SE was significantly higher than that of CSE (p = 0.004).
Based on the actual diagnoses, we constructed ROC curves for CSE and ARFI induced SE in two lesion-depth groups respectively. For the CSE, AUCs were similar for different depths: 0.798 for lesions of depth <10 mm versus 0.846 for those ≥10 mm (p > 0.05). In addition, for the ARFI induced SE, there was also no significant difference between two groups: 0.859 for lesions of depth <10 mm versus 0.778 for those of depth ≥10 mm (p > 0.05). There was also no significant difference concerning the diagnostic performance between the both SE techniques in two groups (all p > 0.05) (Table 2).
Comparison of CSE and ARFI induced SE AUC values between different lesion-depth ranges
Comparison of CSE and ARFI induced SE AUC values between different lesion-depth ranges
*No significant difference compared with CSE in the same group; #No significant difference compared with breast lesions with lesion depth of <10 mm; CSE = conventional strain elastography; ARFI = acoustic radiation force impulse; SE = strain elastography; AUC = area under the ROC curve.
The sensitivity, specificity, accuracy, PPV and NPV for BI-RADS alone, BI-RADS plus CSE and BI-RADS plus ARFI induced SE were shown in Table 3. Although there were no significant differences among the three in terms of the sensitivity, PPV and NPV, the specificity of the combined method with ARFI induced SE increased significantly compared with US BI-RADS alone and combined method with CSE (p = 0.004, p = 0.004, respectively). With regard to accuracy, the combination of US BI-RADS and ARFI induced SE was higher significantly than US BI-RADS alone, as well as combined method with CSE (p = 0.043, p = 0.016, respectively).
The diagnostic performances of three BI-RADS modalities in predicting benign and malignant breast lesions
Data are percentages, with numerators and denominators in parentheses. ‡In comparison with BI-RADS, p < 0.05. §In comparison with BI-RADS+CSE, p < 0.05. US BI-RADS = ultrasound Breast Imaging Reporting and Data System; CSE = conventional strain elastography; ARFI = acoustic radiation force impulse; SE = strain elastography; SEN = sensitivity; SPE = specificity; PPV = positive predictive value; NPV = negative predictive value; ACC = accuracy.
Strain imaging elastography has been confirmed to be effective for discriminating benign and malignant breast lesions [14, 29–31]. In our study, by setting a cutoff value of score 3, CSE showed a sensitivity of 85.4% and a specificity of 58.1% in diagnosing breast lesions, which is consistent with previous studies [15, 32]. However, the reproducibility of CSE has always been doubted, owing much to the potential influence of uncontrollable pre-compression caused by the operator and relativity of strain displacement between lesion and surrounding tissue [33, 34]. Also, according to elastography guidelines [13], possibly artifacts in CSE evaluation exists because of divergent stress distribution within the body and the non-linear stiffness of tissue. Xu et al. [24] reported better diagnostic performance of ARFI induced SE in predicting thyroid malignancy than CSE. ARFI can overcome the limitations of CSE, which is initiated by free-hand pressure, thus leading to better inter-rater agreement. In our study, ARFI induced SE had a significantly higher specificity (83.9% vs. 58.1%, p < 0.05) without loss of sensitivity. Additionally, it was shown in a prior study that ARFI induced SE was a predictor of breast malignancy with an AUC value of 0.871 and 81.7% specificity, which was similar with our results [17].
According to previous studies [35, 36], lesion depth is known to influence the quality of US elastography. However, there was no significant difference concerning the diagnostic performance between the two groups with the both SE techniques (all p > 0.05) in this study. This discrepancy was possibly on account of the differences in measuring methods and group standard. Zhou et al. [35] found that the lesion with a lesion depth of >15 mm was associated with lower quality of shear wave propagation compared with the lesion with a lesion depth of <15 mm, and measured lesion depth as the distance from the skin to the center of the lesion. In our study, by contrast, all breast lesions were categorized into two groups according to lesion depth:<10 mm and >10 mm, also, we termed the distance from the skin to the shallowest margin of the lesion as the lesion depth.
Our results suggested that BI-RADS plus CSE did not show a higher accuracy or specificity for differentiation between benign and malignant lesions in comparison with US BI-RADS alone, which is in agreement with some studies [27, 37]. However, multiple previous studies concluded that CSE might be of powerful use in improving the diagnostic performance of the US BI-RADS alone [14, 30].This difference was probably due to the divergence in the inclusion criteria or pathological diagnoses of breast lesions. Prior studies either focused on circumscribed lesions [14] or included more lobular carcinoma (n = 6) or micro-invasive ductal carcinoma (n = 2) than those of the present study (n = 1, n = 0, respectively) which may have potential effect on elastography scores [30]. On the other hand, the specificity and accuracy of the combined method with ARFI induced SE (80.6%, 84.5%, respectively) increased significantly compared with US BI-RADS alone (54.8%, 73.6%, respectively) and combined method with CSE (56.5%, 72.7%, respectively) (all p < 0.05) without the loss of sensitivity. The higher specificity may lead to avoid 16 unnecessary biopsies commended by US BI-RADS alone. A similar diagnostic performance of BI-RADS combined with ARFI induced SE was found in a study performed by Zhou et al. [17]. Therefore, it appears that this combination method in the current study is more promising. However, this finding is needed to be investigated thoroughly and maybe the subject of further studies. The specificity of US BI-RADS combined with ARFI induced SE was elevated from 54.8% to 80.6% (p < 0.05).
There were some limitations in this study. First, this study was performed in a single institution with a limited sample size. Thus, a multicenter study with a larger number of patients in the future is needed. Second, there was unavoidable selection bias in the present study due to its retrospective nature. Third, we did not evaluate the inter- and intra-observer variability of both elastgraphy techniques. In addition, strain elastography in the present study were performed after conventional US examinations, in which elastography results might be subjective to radiologist’s bias. What’s more, elastography technology is available only in some special high-end ultrasound machines. Also, performing B-mode imaging with a high-resolution probe (e.g., an 18L6 linear array transducer, frequency range: 5.5-18 MHz) would enable better visualization of anatomical structures on conventional US. Finally, a few alternative imaging modalities should be taken in consideration with potential clinical benefits of improved diagnostic performance for distinguishing benign from malignant lesions: contrast-enhanced ultrasound can aid identification of benign and malignant breast lesions through visualization of the microcirculation within the lesion [38], and the MicroPure ultrasonography technology has an advantage in detecting microcalcifications [39], etc.
In conclusion, both CSE and ARFI induced SE are promising for breast cancer prediction with good diagnostic performance. Our study showed that BI-RADS plus ARFI induced SE had a better diagnostic performance in the diagnosis of breast lesions in comparison with BI-RADS alone or BI-RADS plus CSE.