
Abstract
Coronary scaffolds have been recently developed to address the long-term limitations of metallic drug eluting stents. Concerns have however been expressed on the safety of these devices, with evidence of both early and late scaffold thrombosis. While early thrombosis has been associated with incomplete scaffold expansion, leading to flow disturbances, blood recirculation, and platelet activation, the pathophysiology of late events remains less understood. Recent cases series have shown that malapposition and scaffold dismantling might play a role in this phenomenon, an observation that further confirms the importance of an accurate implantation. Further, the role of dual antiplatelet therapy, and whether prolonging it may reduce event rates, remains to be elucidated. As well, the role of inflammatory phenomena has been proposed but never demonstrated. This brief review summarizes the current evidence on these phenomena.
Introduction
Metallic drug-eluting stents (DES) have been employed since almost 15 years for the treatment of coronary artery disease. Although these devices appear to be safe and effective over long-term follow-up, particularly in their newer generations, their drawback is the risk of late (i.e., beyond 1 year) adverse events, including repeat revascularization [1] and thrombosis. Since it is believed that these events might be partly due to the permanent nature of the metallic stents in the coronary artery wall [2], bioresorbable scaffolds (BRS) were developed with the hope that they would attenuate the 1.5–3% annual risk of adverse events occurring with DES after the first year of implantation. BRS initially offer a mechanical support similar to that of DES, but rapidly lose their structural integrity and are completely resorbed within 12 to 36 months. This allows the return of coronary vasomotion, which has been linked to the increased risk of repeat revascularization [3]. Further, preclinical studies provided evidence to the concept that implantation of BRS is associated with favorable vessel remodeling [4], even though this evidence was not confirmed in the Absorb III trial. The use of the first commercialized scaffold, the Absorb of Abbott Vascular was approved in June 2016 by the US Food and Drug Administration based on the results of the 1-year data of the ABSORB III trial showing non-inferiority compared with everolimus-eluting stents at 1 year [5]. Despite these initial results, BRS have been rather consistently associated with a ∼ two-fold excess risk of device thrombosis within the first two years [6–10], an observation which dramatically tempered the enthusiasms for these devices.
Early scaffold thrombosis
The incidence of scaffold thrombosis shows a bimodal distribution, with one peak early after implantation (<30 days), covering about 50% of the risk over the first two years, and another, more gradually distributed over time, increased incidence after the first year, possibly associated with the withdrawal of dual antiplatelet therapy. As of early phenomena, as previously described [11], the scaffold’s thick struts may interrupt the laminar flow, create microdomains in which blood recirculates, reversal of the flow behind the struts and subsequent fibrin deposition.
Such rheological alterations are potentiated in cases of incomplete scaffold deployment, for instance when the vessel is too small, or it is relatively smaller than the scaffold implanted, or when the scaffold is incompletely deployed, all conditions which lead to a relative high footprint of the scaffold and a relatively high scaffold/vessel ratio [12].
The evidence on late events
Several Occurrences of scaffold beyond 1 year after implantation have however also been reported in single cases and clinical studies [1, 14–16]. In recent meta-analyses, the risk for very late thrombosis was higher in the BVS group than in the EES group [17].
Poly-L-lactic acid–based scaffolds require 12–36 months before they are completely resorbed, leaving no foreign materials in the vessel wall. Even though evidence suggestive of inflammatory reactions has also been reported [18], this resorption of the polymeric scaffold is generally thought to be a benign process when it occurs inside the proliferating neointima. In contrast, it represents a safety hazard when it occurs inside the lumen. Before the struts disappear, however, their loss of structural integrity might lead to intraluminal dismantling of the scaffold, evidence of which has been observed at optical coherence tomography imaging. Dismantling (Fig. 1) might lead to disruption of the laminarity of flow, turbulence, and shear-induced activation [19] of thrombocytes. As such, dismantling has been associated with very late scaffold thrombosis [13, 20]. Similar phenomena were originally reported with first-generation DES, in cases in which inflammatory/hypersensitivity reactions lead to evaginations and DES thrombosis [21]. In a recent series malapposition, incomplete lesion coverage, and underdeployment were the most frequent findings in 17 early scaffold thromboses, whereas malapposition (35%), late discontinuities (31%), both associated with peristrut low-intensity areas suggestive of inflammation (19%) were associated with late/very late cases [20, 23].
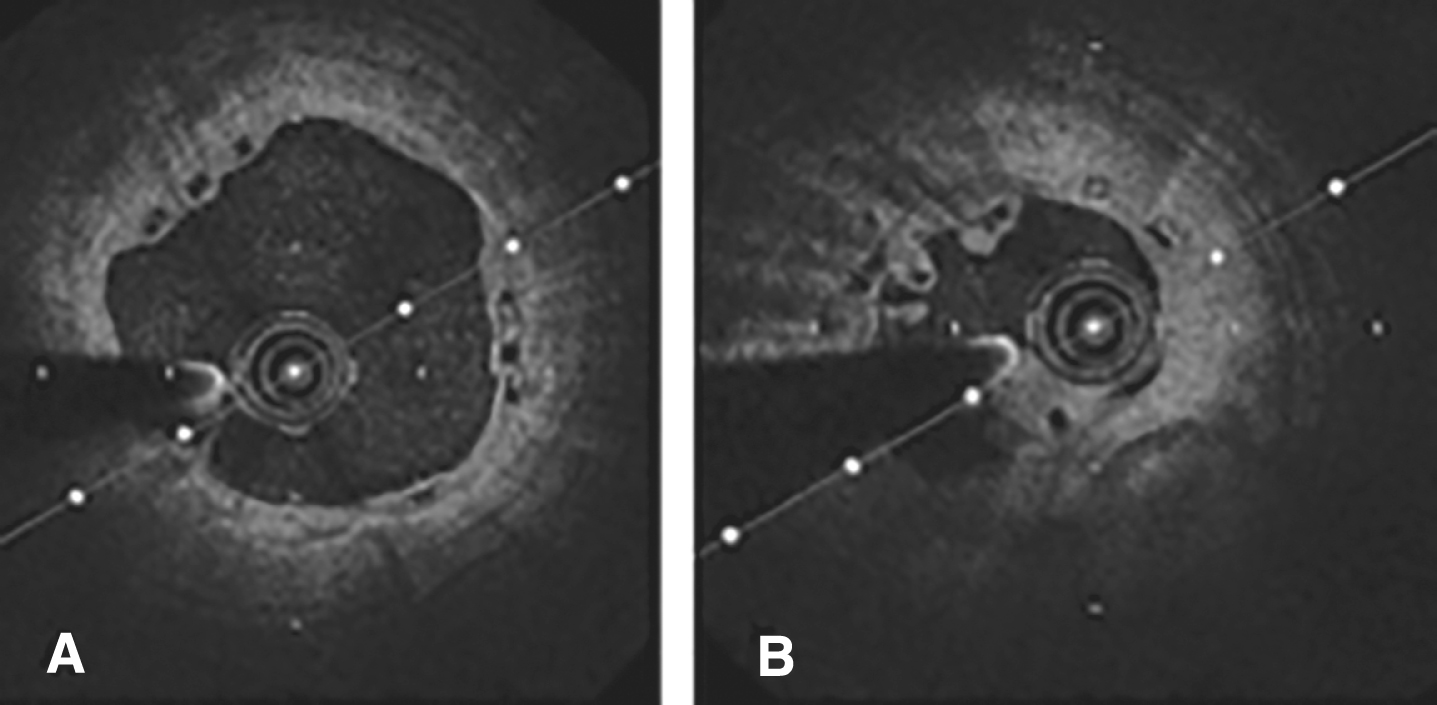
(A) a well apposed scaffold (black boxes). (B) evidence of scaffold dismantling and formation of endothelial bridges.
In sum, persistent strut malapposition of the scaffold might be an important mechanism of very late scaffold thrombosis, which could then possible be avoided by precautions aimed at reducing the risk of malapposition, including careful device sizing and meticulous implantation technique guided by intracoronary imaging.
While most lines of evidence emphasize the role of strut thickness and incomplete deployment, a propensity-matched analysis demonstrated that BVS implantation is associated with a higher risk of periprocedural myocardial infarction as compared with first-generation sirolimus-eluting stents, which have a similar strut thickness [23]. As well, early discontinuation of dual antiplatelet therapy could contribute to the increased risk of late scaffold thrombosis. In line with this, some authors suggested that the discontinuation of dual antiplatelet therapy after BVS implantation might be associated with late events [23–25].
Conclusions
A recent recommendation of a working group of the European Society of Cardiology states that “bioresorbable scaffolds should not be favored over metallic stents” for the treatment of coronary artery disease. Evidence from clinical studies shows that a balance between the known thrombotic risk of scaffolds, especially when incorrectly implanted, and the yet unknown but potential benefits after complete scaffold resorption should be done. The evidence that applying a meticulous implantation technique leads to a significant reduction in both early and late events is there. Scaffolds remain an excellent alternative to permanent implants, but the safety of newer generations of these devices in the hands of unexperienced operators must first be demonstrated.
Footnotes
Acknowledgments
Tommaso Gori received speaker’s honoraria from Abbott Vascular.