
Abstract
BACKGROUND:
Natural and synthetic estrogens seems to have opposite effects on thrombosis and female cardiovascular system, since natural estrogen was supposed to be protective against cardiovascular diseases and synthetic estrogen has been related to thrombosis and cardiovascular diseases. In this work we have investigated if these differences could be related with the effects on those hormones on some hemorheological parameters.
OBJECTIVE:
The objective of this work was to investigate the hemorheological changes of different concentrations of beta-estradiol and ethinylestradiol, on RBC aggregation and RBC deformability.
METHODS:
Samples of blood of healthy donors were added with different concentrations of natural beta-estradiol or synthetic ethinylestradiol and were analyzed for red blood cell (RBC) aggregation and RBC deformability.
RESULTS:
There were no significant changes in RBC aggregation. Both beta-estradiol and ethinylestradiol increase the RBC deformability in shear stresses above 3.0 Pa accordingly with the hormone’s concentration.
CONCLUSIONS:
Beta-estradiol and ethinylestradiol enhance RBC deformability dependent of their concentration. These findings may explain the different patterns of thrombotic and cardiovascular effects in different phases of the menstrual cycle or different dosages of oral contraceptive or hormonal replacement therapy.
Keywords
Introduction
Ovary hormones are very important to the women’s health. Estrogen is a steroid hormone which regulates the women reproductive system and is responsible for the secondary sex characteristics [1]. Beyond the action on the reproductive system, estrogen is being accepted as protective against cardiovascular diseases and other organs not primarily related to the reproduction system. The term “estrogen” refers to a group of steroid hormones, and the predominant hormone is 17-β-estradiol, also known as beta-estradiol [2].
A lack of ovarian hormones, as seen in ovarian insufficiency and menopause, lead to several diseases, venous thromboembolism and cardiovascular diseases among them [3]. Paradoxically, oral contraceptives are related with venous thrombosis. A systematic review shows that several combined oral contraceptive increase the risk of venous thrombosis [4]. Thromboembolism is also associated with hormone replacement therapy [5]. These studies lead us to believe that there are differences between natural produced hormones and the synthetic hormones from oral contraceptives and hormone replacement therapy.
Hemorheology is a science of the deformation and flow of blood [6]. The viscoelasticity of flowing blood is related to the behavior of red blood cells (RBC) suspended in plasma and dependent of the shear rate. Deformability and aggregation of RBC interfere with the rheology of blood [7], and are, at the same time related with cardiovascular diseases [8, 9] and aging [10]. The natural producing ovary hormone, beta-estradiol decreases RBC aggregation and increases RBC deformability in certain shear stresses [11]. On the other hand, RBC aggregation is increased in women taking oral contraceptives containing ethinylestradiol [12]. Taking this into account we hypothesized if the hemorheological differences are related with the molecular structure of estrogens or with their concentrations in blood.
The objective of this work was to investigate the hemorheological changes of different concentrations of beta-estradiol and ethinylestradiol, on RBC aggregation and RBC deformability.
Material and methods
Samples
Blood samples were collected into tubes with lithium heparin (17 UI/mL) as an anticoagulant (BD Vacutainer, Portugal). The study was performed in accordance with the guidelines for hemorheological laboratory techniques and under the protocol established with the Portuguese Institute of Blood and Transplantation in Lisbon, Portugal. All donors were males and duly informed and, also, signed their agreement.
Hormones addition
Each blood sample was divided into ten aliquots of 1 mL and centrifuged at 11,000 rpm in Biofuge 15 Centrifuge (Heraeus, Germany) during 1 min at room temperature. One aliquot is used as control and in the others10μL of plasma were removed. In one aliquot the plasma removed was replaced by 10μL of DMSO (Sigma-Aldrich, Germany). The others 8 aliquots were divided in two groups, 4 for beta-estradiol (Sigma-Aldrich, USA) testing and 4 for ethinylestradiol(Sigma-Aldrich, USA), and an amount of each hormone were added with DMSO in order to entire 10μL. Blood aliquots were gently mixed by inversion, and RBC aggregation and RBC deformability were assessed. The final concentration of beta-estradiol added in each one of the 4 tubes was: 50, 100, 150 and 200ρg/mL. The final concentration of ethinylestradiol added in each one of the 4 tubes was: 25, 50, 75 and 100ρg/mL. Further in discussion the difference of concentrations used between the two estrogens will be explained.
Erythrocyte aggregation index (EAI)
RBC aggregation was determined using the MA1 aggregometer (Myrenne GMBH, Germany). The MA1 aggregometer consists of a rotating cone plate chamber which disperses the sample by high shear rate of 600 s–1 and a photometer that determines the extent of aggregation. The intensity of light (emitted by a light emitting diode) is measured after transmission through the blood sample. The aggregation will be determined in stasis for 10 seconds after dispersion of the blood sample.
RBC deformability determination by laser diffractometry
RBC deformability was assayed by using a Rheodyn SSD laser diffractometer (Myrenne GMBH, Germany). Twenty μL of each blood sample were diluted in 2 mL dextran solution (Pharmacia, osmolality 0.300, pH 7.4, viscosity 0.24 mPa.s). This suspension was introduced into a measuring chamber formed by two glass disks, one static and other connected through a rotational arm to a synchronized step motor. A 1 mV helium-neon laser beam is passed through the blood suspension, and the diffraction pattern analyzed at following shear stress forces values: 0.3, 0.6, 1.2, 3.0, 6.0, 12.0, 30.0, 60.0 Pa. In the static position at rest, the laser diffraction pattern is circular, becoming elliptic as the erythrocyte were deformed by application of increasing shear stress. Light intensity and the diffraction pattern were measured in two orthogonal axes and the erythrocyte elongation index (EEI) calculated from the length (L) and width (W) by the following formula EEI = 100×(L–W)/(L +W). EEI values are expressed as percentage.
Statistical analysis
Data are presented in graphics. Differences between the mean values were evaluated by using software GraphPad Prism 4.0 Version and analysis test used ANOVA followed the test of multiple comparison of Dunnet. Values were considered statistically significant for p < 0.05.
Results
RBC aggregation
DMSO, which was used as hormone’s solvent, decreased the EAI. Therefore, we could compare only the DMSO group with the hormone + DMSO groups. The obtained results showed no significant differences between EAI of both ethinylestradiol (Ee) and beta-estradiol (β-E) when compared with DMSO control group (Fig. 1).
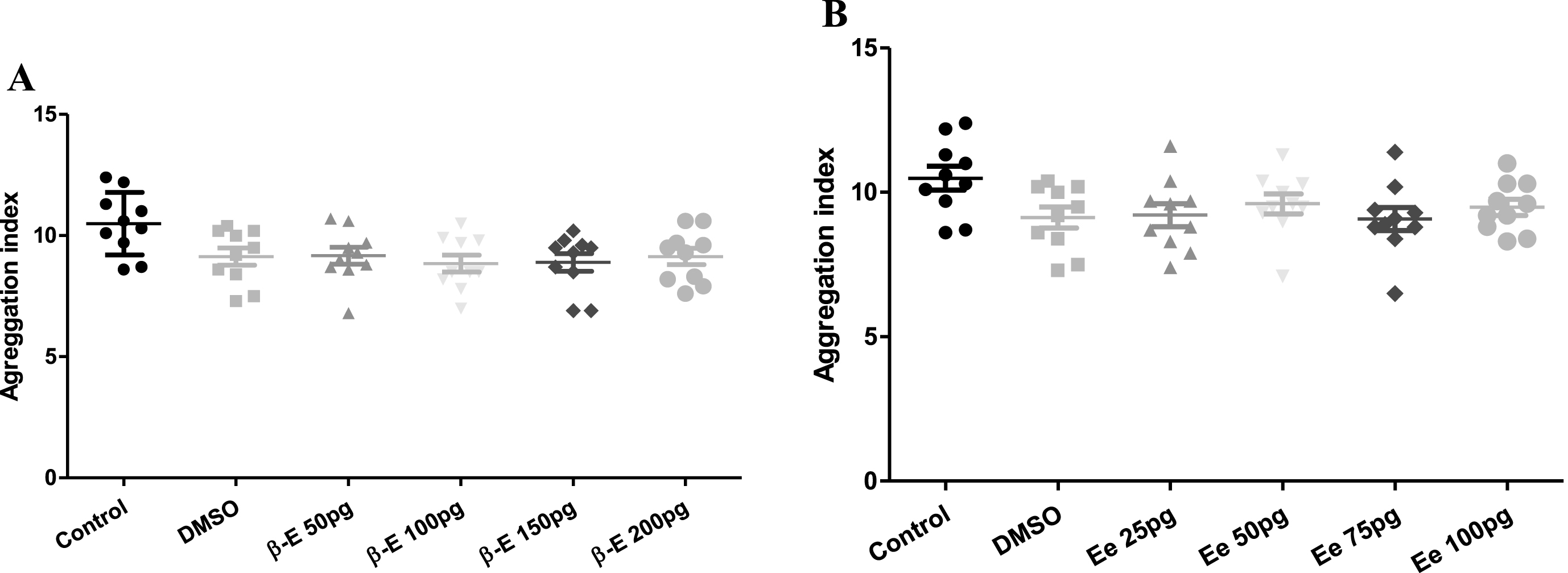
Aggregation indexes of control and experimental groups of (A) beta-estradiol (β-E) and (B) ethinylestradiol (Ee). No statistical differences were obtained between the DMSO and the experimental groups of beta-estradiol or ethinylestradiol.
DMSO did not change significantly the EEI when compared with control.
Effect of Beta-estradiol on the EEI
Beta-estradiol modified the EEI for some shear stress values according to the concentration. These results are summarized in Table 1 and Fig. 2.
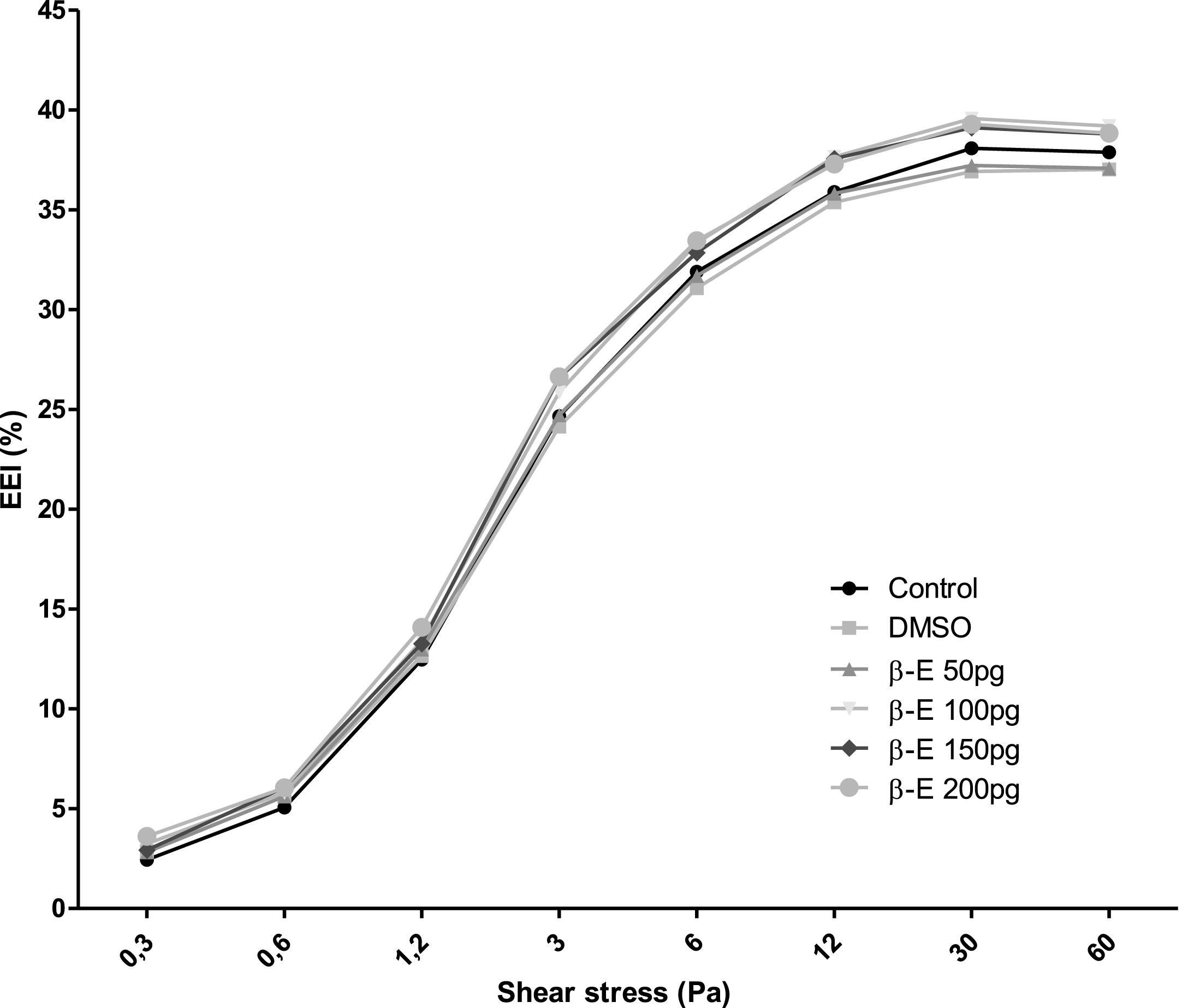
Erythrocyte Elongation indexes (EEI) of control and beta-estradiol (β-E) experimental groups measured at shear stresses between 0.3 and 60 Pa.
Statistically significant changes in the EEI with different beta-estradiol concentrations
*p < 0.05 and **p < 0.01 in relation to the DMSO group.
Ethinylestradiol also modified the EEI in some shear stress according to the concentration. These results are summarized in Table 2 and Fig. 3.
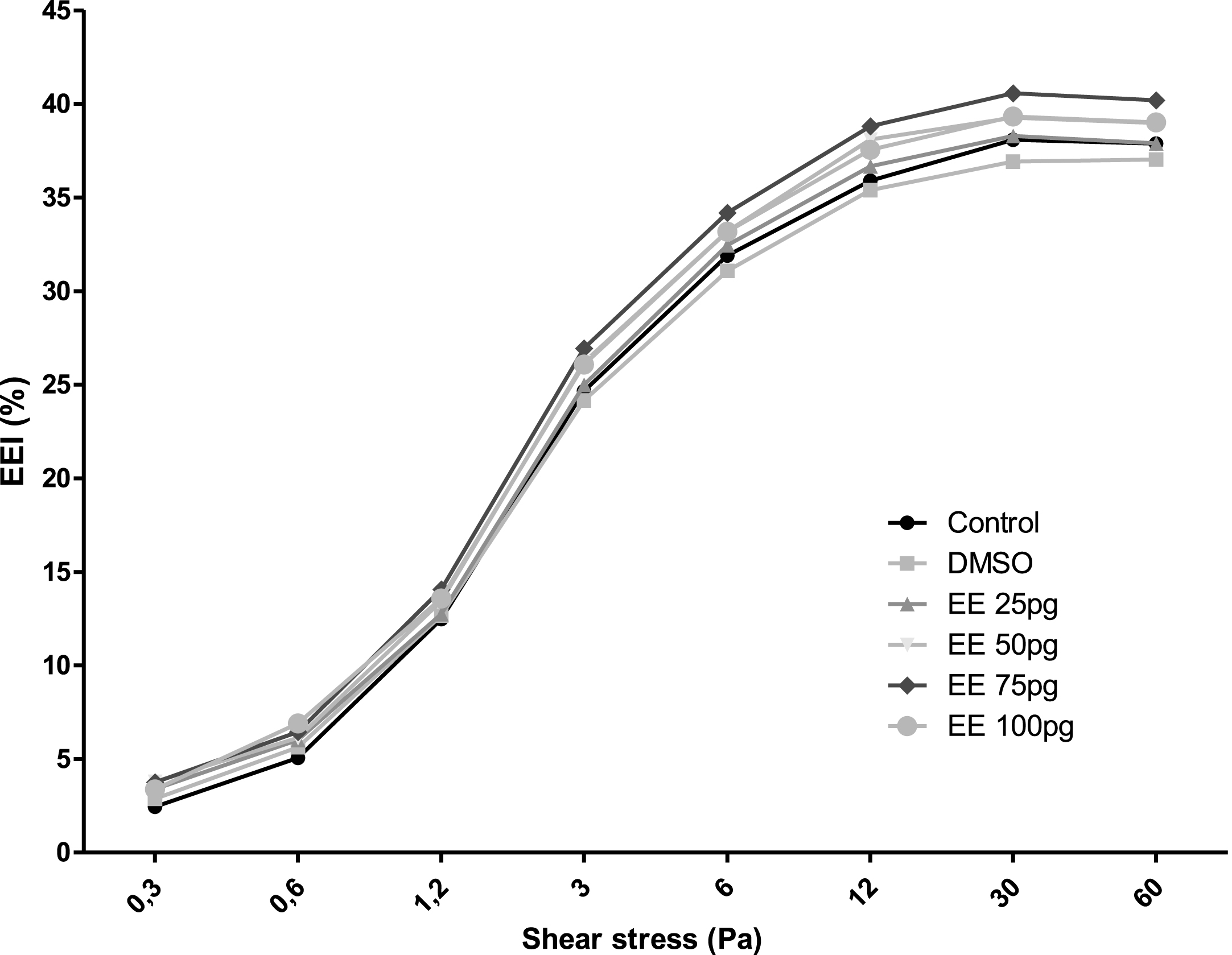
Erythrocyte Elongation indexes (EEI) of control and ethinylestradiol (EE) experimental groups measured at shear stresses between 0.3 and 60 Pa.
Statistically significant changes in the EEI with different ethinylestradiol concentrations
*p < 0.05, **p < 0.01 and ***p < 0.001 in relation to the DMSO group.
The influence of hormones in women’s health has been a concern in the scientific community. Hormonal replacement therapy for relieve of vasomotor symptoms has been associated with an increase in incidence of coronary events, venous thromboembolism, stroke, breast cancer, death of lung cancer and gallbladder disease [13]. Oral contraceptive pills are related with pulmonary and venous thromboembolism [4]. These results are in contrast with women’s natural hormones, which seem to protect against some of listed diseases [2]. We developed an in vitro model in order to replicate various concentrations of both natural and synthetic estrogens in blood to verify if the influence in the blood would be from the quality of estrogen or the concentration in blood. There are some biases in our model. Firstly, we use male’s blood in order to avoid exogenous hormones taken by women. Secondly, men have different hormonal profile, as higher testosterone levels [14, 15]. Thus, this different hormonal balance can interfere in the results. On the other hand, plasma levels of beta-estradiol in males are lower than in females [16] and not subject to cyclic changes or exogenous estrogens. We have used beta-estradiol concentrations to match the references in various phases of menstrual cycle in normally cycling women [17]. Also we have used concentrations of ethinylestradiol matching the concentrations in the blood of women taking contraceptive pills [18]. But apart the hormonal profile, we could not be certain about the total free hormone level after dropping the hormones in blood samples. Hormones can bind receptors and proteins as sex hormone-binding globulin [18]. Beta-estradiol also binds fibrinogen modifying this structure and consequently its effect on erythrocyte aggregation [19, 20].
Our results didn’t show any differences in RBC aggregation index in both beta-estradiol and ethinylestradiol. Previous research made in our laboratory have shown a significantly decrease of EAI in blood of women taken either transdermic beta-estradiol or hormonal replacement therapy [10]. The different result could be from different hormonal profile of the subjects or from free blood hormones. Maybe the aggregation can have the same behavior of deformability, but our model could not elucidate this subject. The same study has shown an increase of EEI at 30 Pa with beta-estradiol, which corroborate with our findings.
We found that both beta-estradiol and ethinylestradiol increase RBC deformability, but these effects are non-linear and dose-dependent, showing up only in shear stress above 3.0 Pa. Beta-estradiol at 100 and 200ρg/mL were the most effective concentrations in increase EEI for different shear stress values. The final concentration of 50 ρg/mL of beta-estradiol didn’t show changes in the EEI which may indicate that low concentration of beta-estradiol, as observed in the start of the menstrual cycle, acts different from higher concentrations of other cycle’s phases.
In our study, ethinylestradiol behaves similarly to beta-estradiol. At 75 ρg/mL of ethinylestradiol we observed an increase in EEI values in all shear stresses above 3.0 Pa which is different from other concentrations of the hormone, higher or lower.
RBCs are the most “flexible” cells of the mammalian organism and RBC deformability is the determinant of blood viscosity at high shear rates. RBC deformability is affected in various aging related diseases, as circulatory disorders and diabetes [9]. RBCs deformability improves flow in the microvessels and in large arteries at high shear rate [21, 22]. Red blood cell geometry and the rheological properties of erythrocyte intravascular fluid and of erythrocyte membrane are factors that can interfere in the deformability of RBCs [23, 24]. RBCs with impaired deformability are less able to squeeze through the capillaries and can cause margination of platelets, increasing the propensity of thrombosis [25].
RBC deformability, measured by filterability, is significantly lower in post-menopausal women than in the menstruating women which can be explained by lack of beta-estradiol [26]. Also, the risk of thrombosis is higher in oral contraceptives with higher levels of ethinylestradiol [4]. It is possible that this effect is due to the concentrations of serum ethinylestradiol.
Therefore, we found that hemorheological properties of RBCs, particularly deformability, vary as a result of the amount of blood estrogens, natural or synthetic. However the interference of the hormones is not linear; possibly because there are specific concentrations in blood which lead a higher deformability. These findings contribute for the research of physiology and physiopathology of women’s sexual hormones. Hormone’s effects can be explained also by the hemorheological interferences. The same rationality may be applied for oral contraceptives and hormone replacement therapy, finding a hormone concentration that cannot harm, or even is beneficial for health.
In conclusion, both estradiol and ethinylestradiol increase RBC deformability in shear stress above 3.0 Pa accordingly with the hormone’s concentration.
Footnotes
Acknowledgments
The main author would like to acknowledge Frank Hartman whose contribution to this work was of great significance.
This work was funded by Fundação para a Ciência e Tecnologia:
LISBOA-01-0145-FEDER-007391, project cofunded by FEDER, through POR Lisboa 2020 - Programa Operacional Regional deLisboa, Portugal 2020.