
Abstract
BACKGROUND:
Carotid stenting stimulates intimal proliferation through platelet and stem cell activation.
OBJECTIVE:
The aim of this study is to evaluate whether the administration before or after carotid stenting of clopidogrel loading dose may play a role on circulating endothelial progenitor cells, stromal cell-derived factor-1α (SDF-1α) and neointimal hyperplasia.
METHODS:
We recruited 13 patients (aged 74.52±7.23) with indication of carotid revascularization and in therapy with salicylic acid and statin. We blindly randomized them in two groups: pre-carotid angioplasty with stent (Pre-CAS group) receiving 300 mg of clopidogrel before stenting, and post-carotid angioplasty with stent (Post-CAS group) receiving 300 mg after stenting. At the admission, we valued endothelial progenitor cells, SDF-1α and prospectively we repeated blood samples and measured intima-media thickness to estimate neointimal hyperplasia on the stent at 3, 6 and 12 months.
RESULTS:
In the days following the CAS, we found a lower, statistically not significant, trend of endothelial progenitor cells in Pre-CAS group. The SDF-1α concentration tended to be lower at baseline in the pre-CAS group than in the post-CAS group and it did not show an increase in the observed time. On the contrary, in the Post-CAS group we observed a peak at six hours with a significant reduction (p < 0.001) at one day after stenting.
The intima-media thickness was significantly lower in the Pre-CAS group than the Post-CAS group both at six months and 12 months after stenting.
CONCLUSIONS:
Pre-stenting clopidogrel loading dose leaded to short-time modification of endothelial progenitor cells and platelets and to long-term a minor neointimal hyperplasia.
Abbreviations
acetylsalicylic acid
body mass index
carotid angioplasty with stent
confidence interval
diastolic blood pressure
ethylenediaminetetraacetic acid
endothelial progenitor cells
erythrocyte sedimentation rate
glycosylated hemoglobin A1c
high density lipoprotein-cholesterol
hierarchical generalized linear models
heart rate
intima-media thickness
low density lipoprotein-cholesterol
major adverse cardiovascular events
mean flow velocity
New York Heart Association
pulsatility index
pulse pressure
peak systolic velocity
quantile-quantile
systolic blood pressure
resistance index
standard deviation
stromal cell-derived factor-1α
vascular endothelial growth factor
vascular endothelial growth factor receptor 2
Introduction
Carotid angioplasty with stent (CAS) produces an insult on the vascular wall which represents an important stimulus to re-endothelialization of the vessel through neointimal proliferation [1]. After endothelial injury, the release of chemotactic and growth factors are crucial; generally for 28–69 days, the endothelium persists in an inflammatory phase after bare metal stenting [2]. Animal studies have shown a significant correlation between endothelial damage caused by metal body and subsequent neointimal hyperplasia [3, 4], leading to possible early in-stent restenosis. Circulating stem cells as endothelial progenitor cells (EPCs) provide a constant primary regeneration of endothelium following vascular damage, repairing the injured wall [5]. Inflammation, ischemia and trauma represent the main causes of cellular mobilization, EPCs homing and platelet activation [5, 6]. In normal conditions, EPCs count is low and variable; in marrow CD34+ represent only 3% of all cells, while circulating CD34+ are the 0.01 – 0.05% of mononuclear cells [7]. Furthermore, EPCs seem to be only 2% of all CD34+ cells [8] and several conditions as age, renal injury, common cardiovascular risk factors and drugs as clopidogrel and statin can change the number and functionality of these cells [9–11]. Mediators between endothelium and EPCs are represented by activated platelets that trigger release of one of the most important chemotactic known factors, Stromal Cell-derived Factor-1α (SDF-1α) within the first 30 minutes [12]. In contrast to other chemokines, SDF-1α signaling occurs mainly through CXCR4, EPCs membrane receptor, and their interaction regulates both the mobilization of EPCs from the bone marrow and the homing to ischemic tissues [13, 14].
Clopidogrel plus acetylsalicylic acid (ASA) has been shown to reduce adverse events, as peri-procedural embolic or thrombotic stroke and long-term stroke, without increasing bleeding [15], but the mechanisms underlying the benefits of dual therapy beyond anti-platelet aggregating effects to other atheroprotective processes underlying remain unclear [16]. Throughout the years, many scientific societies have proposed clopidogrel therapy beyond ASA in patients undergoing CAS [17, 18], there is not a strong evidence in the literature regarding the effect of optimal timing of antiplatelet therapy on the expression of EPCs, the release of SDF-1α and neointimal hyperplasia. The aim of our study was to evaluate the different role of clopidogrel loading dose (300 mg) before or after carotid stenting on circulating EPCs, SDF-1α and IMT.
Materials and methods
Study design
This was a prospective randomized no-profit double blinded study, approved by the local Ethics Committees on human experimentation of “Casa Sollievo della Sofferenza” Hospital on October 23, 2012 and following the Declaration of Helsinki [19], the guidelines for Good Clinical Practice [20] and the CONSORT 2010 Statement [21]. The study was conducted on patients admitted in the Cardiovascular Department of the “Casa Sollievo della Sofferenza” Hospital in San Giovanni Rotondo, Italy, from September 29, 2013 to March 29, 2014, as showed in Fig. 1.
Randomisation
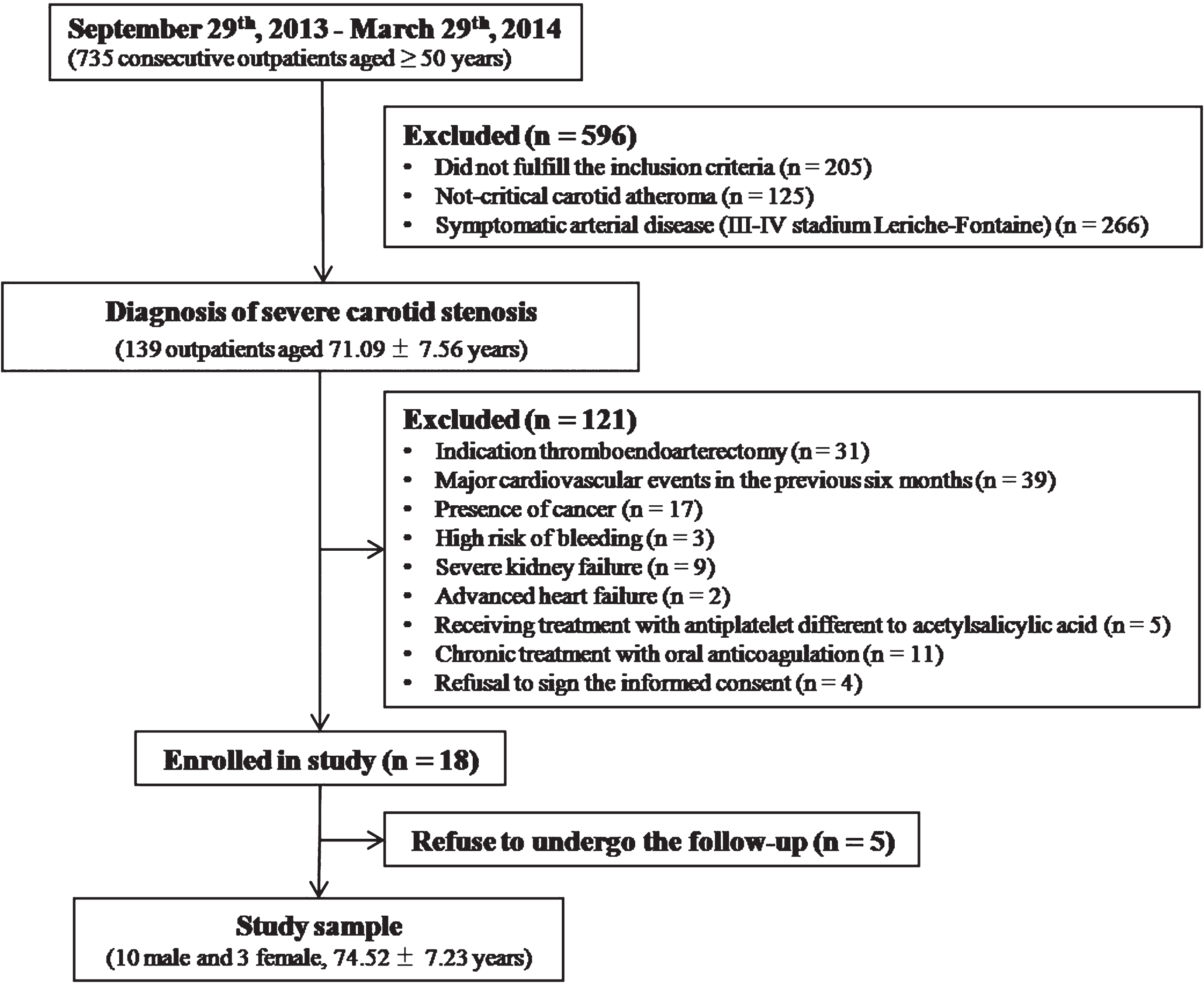
Summary of study design.
Prior to carotid stenting, patients were randomly allocated to clopidogrel loading dose before or after carotid stenting. The method used to implement the random allocation sequence was numbered sealed envelopes. An independent statistician prepared the sequence generation. Thus the patients were divided into two groups: Pre-CAS group received 300 mg of clopidogrel 12 hours before the carotid stenting and placebo immediately after the procedure; Post-CAS group received placebo 12 hours before the procedure and 300 mg of clopidogrel immediately after stenting.
We recruited 13 patients affected by severe carotid stenosis (>70% detectable by duplex ultrasound with NASCET method), clinically asymptomatic with indication to stenting after multidisciplinary team evaluation of comorbidities, bifurcation position, intracranial extension of atherosclerotic plaque, surgical access and risk of cerebral ischemia during carotid clamping [18]. All patients were defined asymptomatic and free from stroke, transient ischemic attack or monocular blindness for three months before stenting.
The inclusion criteria were: older than 50 years, candidates for self-expandable Nitinol-Rx stent, no major adverse cardiovascular events (MACE) in the previous six months.
MACE were defined as stroke, myocardial infarction, lower limbs’ acute ischemia and coronary or peripheral revascularization.
The exclusion criteria were: presence of cancer, high risk of bleeding as severe liver failure, peptic ulcer and proliferative diabetic retinopathy, severe kidney failure with glomerular filtration rate less than 30 ml/min, advanced heart failure with class III-IV of New York Heart Association (NYHA), known allergy to aspirin or clopidogrel, concomitant anticoagulant therapy, inadequate adherence to medical therapies.
Written informed consent for research was obtained at enrollment.
Clinical and biochemical characteristics of patients
Patients underwent a detailed clinical examination and history of cigarette smoking, obesity through measurement of body mass index (BMI), arterial hypertension (≥130/85 mmHg), dyslipidemia [high density lipoprotein-cholesterol (HDL-Ch) <40 mg/dl in male and <50 mg/dl in female and/or triglycerides ≥150 mg/dl] and type 2 diabetes mellitus, according to the World Health Organization’s criteria and ATP III [22]. Moreover, we assessed cardiovascular events as myocardial infarction, stroke, carotid or lower limb revascularization and myocardial reperfusion procedure in the past.
Variables such as heart rate (HR) and blood pressure were evaluated on admission to hospital (baseline) and after one day of stenting. Biohumoral evaluations of fasting glucose, triglycerides, cholesterol, serum creatinine, hemoglobin, platelet count and erythrocyte sedimentation rate (ESR) were performed at admission. Blood samples to detect biological clopidogrel resistance were collected only from a small number of study patients (data were not usable for adequate statistical analysis).
Pharmacological treatment
At the time of hospitalization, the vascular surgeon verified that patients were already taking appropriate medical treatment (e.g. ASA, statin, diabetes management and blood pressure-lowering medication) and suggested using pantoprazole as proton pump inhibitor. During the 30 days after CAS, all subjects were treated by daily double antiplatelet therapy with 100 mg of ASA and 75 mg of clopidogrel, according to guidelines.
The adherence to medical therapy was monitored for every patients to 1, 3, 6 and 12 months.
Determination of EPCs and SDF-1α
We considered EPCs as cells expressing CD34+, VEGFR-2 (receptor for vascular endothelial growth factor-2) or CD133. Moreover, for our study we considered CXCR4 and CXCR2, specific membrane receptors of EPCs expressed for different chemokines released after endothelial injury. After isolating lymph-monocytic cells from the peripheral venous blood, a panel of monoclonal antibodies was used for assessment of EPCs. Excluding CD45+ cells, resulting populations of cells identified by dual expression of CD34+ and VEGFR-2 (CD34+/VEGFR-2+) or CD133 (CD34+/CD133+) were evaluated. The panel for identification of cellular markers was constituted by monoclonal antibodies as anti-CD45 (APC-Cy7 Anti-Human CD45 Antibody, Becton Dickinson), anti-CD34 (PerCP anti-human CD34 Antibody, Becton Dickinson), anti-VEGFR-2 (APC anti-human CD309 Antibody, Miltenyi Biotec) and anti-CD133 (Anti-Human CD133 PE, Miltenyi Biotec). For the surface expression of CXCR4 and CXCR2 receptors anti-CXCR4 (Anti-Human CD184 Antibody, PE-cy5-conjugated, Becton Dickinson) and anti-CXCR2 (Anti-Human CD192 Antibody, Alexa fluor-conjugated, Becton Dickinson) antibodies were used. The analysis of flow cytometry was performed with the FACSCanto I of Becton Dickinson Biosciences. The frequency of peripheral blood cells positive for these reagents was recognized by fluorescence intensity of at least 100.000 events and analyzed using the FacsDiva of Becton Dickinson software. The number of EPCs was expressed as the absolute number of cells per 1μl as whole blood.
In all patients, the count of CD34+/VEGFR-2+, CD34+/CD133+, CXCR4 and CXCR2 was performed at admission (defined baseline) and after stenting (1, 7 and 14 days).
SDF-1α was the main mediator between endothelium and EPCs, released within the first 30 minutesby activated platelets. Expression of SDF-1α was determined on isolated platelets using SDF-1α Human ELISA Quantitative Kit (Abcam100637) distributed by Prodotti Giani S.p.A.
The blood samples for SDF-1α were got at baseline and at 30 minutes, 6 hours, 1 and 7 days after CAS.
All measurements of EPCs and SDF-1α were performed by two different biologists, respectively, who were both blind to the study.
Intima-media thickness measure
After 3, 6 and 12 months after CAS, the angiologist physician estimated neointimal hyperplasia by measure of the IMT. The evaluation of IMT on the stent was performed on the luminal side of the stent (excluding the plaque external to the stent) on the far wall of the common carotid artery from the first proximal centimeter of stent, by B-mode ultrasonography with 7–10 MHz linear probe of MyLab50 (Esaote). The value of IMT was represented by the average of six consecutive measurements, calculated semi-automatically by the QIMT program of echographer.
Moreover, the angiologist measured the systolic velocity peak (SVP), the medium velocity peak (MVP), the resistance index (RI) and pulsatility index (PI) of the middle cerebral artery before and 6 hours after stenting by transcranial doppler of MyLab50 (Esaote).
All measurements were derived by only one angiologist who was blind to the study.
Statistical methods
Patients’ characteristics were reported as mean±standard deviation (SD) or frequencies and percentages, for continuous and categorical variables, respectively. In case of log-normal distributions, medians (along with first-third quartiles) were reported instead of mean and statistical analyses were performed on logarithm-transformed values. Comparisons between the two treatment groups were assessed using two sample t-test or Fisher exact test for continuous and categorical variables, respectively.
To test changes in SBP, DBP, PP, HR, MFV, PVS, PI and RI before and after CAS, repeated measures ANOVA models were estimated for each outcome at issue, separately.
To test whether outcome means were different within and between each group, we looked at the statistical significance of suitable statistical contrasts defined within the models.
Similarly, to test changes in EPCs, SDF-1α and IMT at different and unequally-spaced follow-up times before and after CAS, hierarchical generalized linear models (HGLMs) for longitudinal data were assessed, for each outcome at issue. As in this case, suitable statistical contrasts were further defined within each HGLM to evaluate whether such means were different within and between each group. Estimated means were carried out from both models and were reported along with their 95% confidence interval (95% CI). Longitudinal plots of the estimated IMT over time were eventually reported for each group at issue, along with error bars which represented 95% CI.
Two-sided p-values <0.05 were considered for statistical significance. All analyses were performed using the software: SAS, Release 9.4 (SAS Institute, Cary, NC, USA) and R (package: ggplot2).
Results
We recruited 13 patients (ten males and three females, aged 74.52±7.23) hospitalized for carotid Nitinol-Rx stenting. Eight patients had severe stenosis on the left carotid and seven on the right carotid; the ecogenicity characteristics of carotid plaques have not been collected. Baseline clinical characteristics of randomized patients were reported in Table 1. The mean length of implanted stents was 36.92±4.80 mm, respectively 37.14±4.88 in Pre-CAS group and 36.67±5.16 mm in Post-CAS group (p = 0.867); the mean diameter was 7.31±0.75 mm with no difference in the two groups (7.57±0.98 mm in Pre-CAS group vs. 7.00±0.0 mm in Post-CAS group, p = 0.172). Furthermore, we have not observed difference in the duration of the procedure in the two groups (data not shown).
Baseline demographic and clinical characteristics of patients
Baseline demographic and clinical characteristics of patients
*For normally distributed values, data were reported as mean±SD and comparisons between the two groups were assessed using two sample t-test. For non-normally (skewed) distributed values, data were reported as median (along with first-third quartiles) and comparisons between the two groups were assessed using two-sample t-test using log-transformed values. For categorical variables, absolute frequency (percentage) was reported and comparisons were performed using Fisher exact test.
A significant overall decrease in systolic (from 127.31±12.85 mmHg to 112.69±18.72 mmHg, p = 0.019) and diastolic (from 79.62±5.94 mmHg to 58.85±8.78 mmHg, p < 0.001) blood pressure were found after positioning the stent, without difference among groups, as shown in Table 2.
Variables at baseline and 6 hours after CAS in patients. Data were reported as means±standard deviation
Abbreviations: DBP, diastolic blood pressure; HR, heart rate; MFV, mean flow velocity; PI, pulsatility index; PP, pulse pressure; PSV, peak systolic velocity; SBP, systolic blood pressure; RI, resistance index.
§this tested whether variables evaluated before the stenting were different between groups;
*this tested whether the absolute changes of variables before and after stenting were differential between groups;
#this tested whether the absolute changes of variables before and after stenting were significantly different from zero in all patients and within each group.
We observed different numerical count of EPCs between Pre-CAS group and Post-CAS group as reported in Table 3. At baseline, we did not find statistical significant differences of number of CD34+/CD133+ and CD34+/VEGFR-2+ (counts per 1000) in Pre-CAS group respect to Post-CAS group. A slight (but not statistically significant) trend to decrease over time of CD34+/CD133+ and CD34+/VEGFR-2+ counts was found in Pre-CAS group only [from 33.62 (95% CI: 21.13–53.50) at baseline to 13.08 (95% CI: 6.21–27.55) after 14 days, p = 0.072, for CD34+/CD133+ and from 16.57 (95% CI: 8.77–31.32) at baseline to 1.02 (95% CI: 0.08–13.28) after 14 days, p = 0.083, for CD34+/VEGFR-2+].
Results of EPCs, SDF-1α and IMT from repeated measures generalized linear models. Estimated means were reported along with 95% confidence interval (95% CI)
Abbreviations: CAS, carotid angioplasty with stent; EPCs, endothelial progenitor cells; IMT, intima-media thickness, SDF-1α, stromal cell-derived factor-1α
∧testing whether estimated means were different between time points.
#testing whether estimated means linearly increased or decreased over time. Pairwise comparison between the Pre-CAS group and the Post-CAS group for IMT (p-values: 0.080, 0.006, 0.007 at 3, 6, 12 months after stent, respectively).
The expression of CXCR2 was slightly lower in Pre-CAS group at the 14 days after stenting [1.02 (95% CI: 0.27–3.89) vs. 2.07 (95% CI: 0.79–5.41), Pre-CAS group vs. Post-CAS group, respectively]. A constant decrease in CXCR2 counts was suggested in Pre-CAS group only (i.e. from 2.35 at baseline to 1.02 mean counts after 14 days).
In the pre-CAS group, the concentration of SDF-1α tended to be lower at baseline respect to post-CAS group and did not show any increase in the observed time. Interestingly, in Post-CAS group we observed a peak at six hours [160.39 (95% CI: 134.53–186.25) vs 97.29 (95% CI: 73.35–121.23), Post-CAS group vs. Pre-CAS group, respectively] and was immediately succeeded by a drastically significant reduction (p < 0.001) at one day after stenting [86.77 (95% CI: 58.80–114.74)] (Fig. 2).
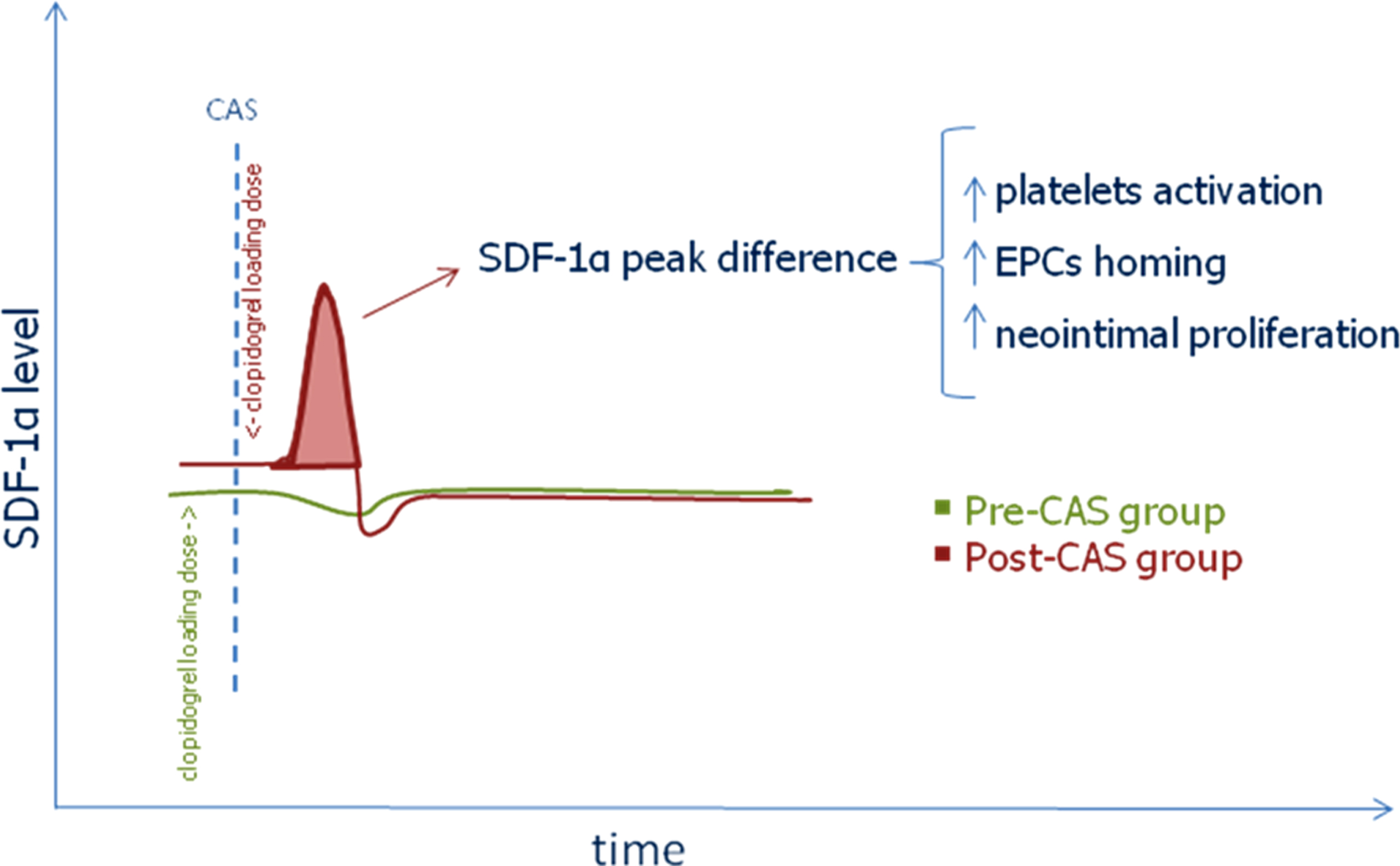
Interpretation model of relationship between SDF-1α blood level and clopidogrel loading dose in Pre-CAS group and Post-CAS group. Abbreviations: CAS, carotid angioplasty with stent; EPCs, endothelial progenitor cells; SDF-1α, stromal cell-derived factor-1α.
Ultrasound measurements showed a continuous lower IMT in Pre-CAS group during the observation time [466.43 (95% CI: 424.81–508.05) μm, 452.29 (95% CI: 410.67–493.91) μm and 462.57 (95% CI: 420.95–504.19) μm at 3, 6 and 12 months after CAS respectively] compared to what occurs in Post-CAS group [526.05 (95% CI: 476.60–575.50) μm, 545.83 (95% CI: 500.88–590.79) μm and 552.67 (95% CI: 507.71–597.62) μm at 3, 6 and 12 months after CAS respectively], with an overall statistical significance difference (p = 0.001) between the two mean profiles. When comparing IMT means between Pre-CAS group and Post-CAS group for each single time point, we found that, although no statistically significant difference was found at 3 months after CAS (p = 0.080), significant differences were found at 6 months (p = 0.006) and 12 months (p = 0.007) after CAS, respectively. P-values adjusted for multiple comparisons becomes 0.080, 0.016 and 0.016 for 3, 6 and 12 months after CAS, respectively (Fig. 3).
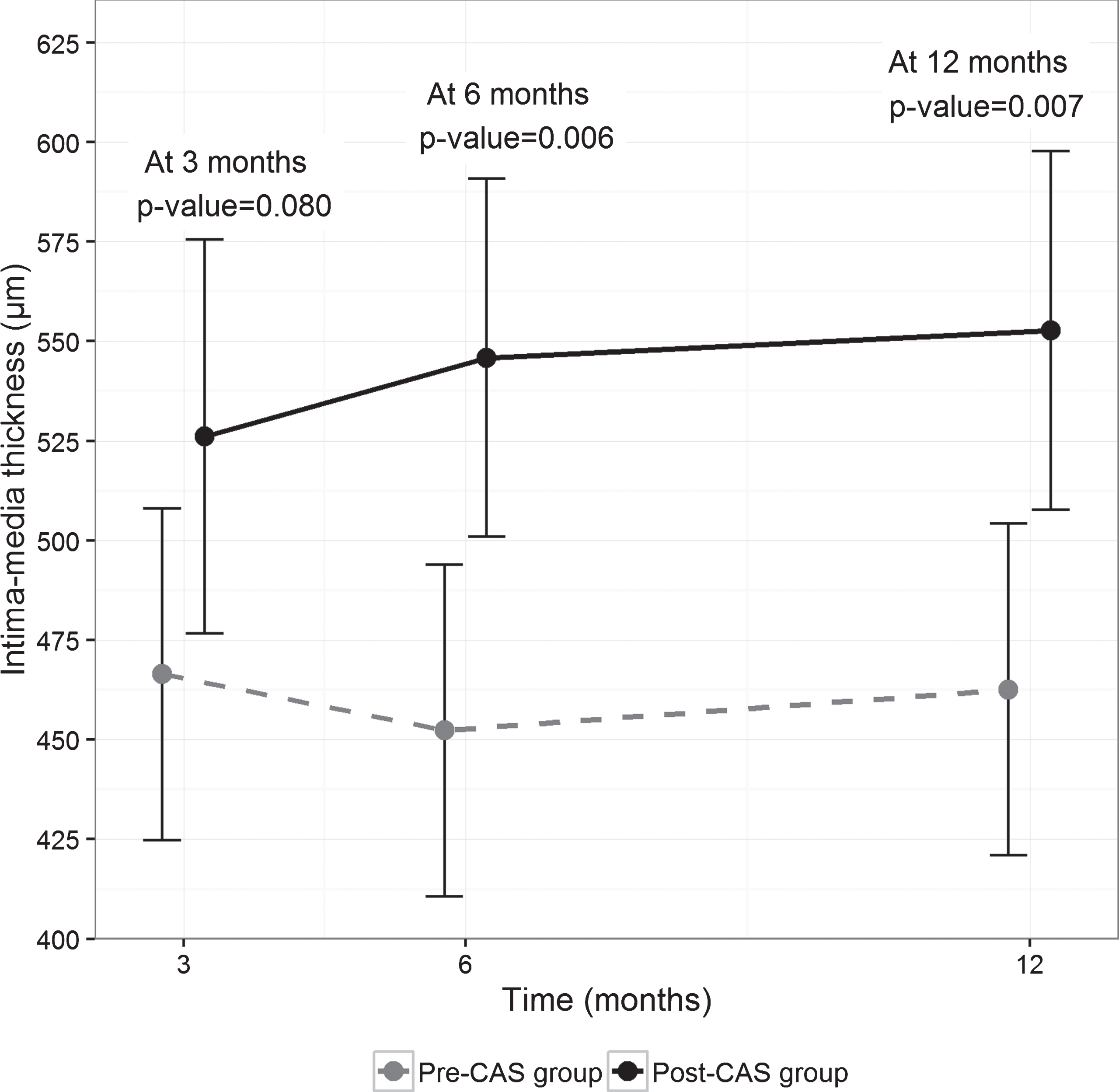
Intima-media thickness means between Pre-CAS group and Post-CAS group at 3, 6 and 12 months. Error bars represented 95% confidence interval around the estimated means.
In the present study, the circulating EPCs were quantified in carotid angioplasty with stent and were examined at different time-points. The data showed that there is a slight reduction of EPCs in peripheral blood in Pre-CAS group, as indicated by the several EPCs’ counts during the short follow up.
Some studies focused on a novel mechanism of vascular repair involving mobilization of EPCs after coronary angioplasty, although involving small and different groups of patients (i.e. anginous subjects), not comparable owing to differences in study design and timing of blood sampling in relation to stent implantation [23–25]. A placebo-controlled crossover study conducted on 41 subjects with stable ischemic heart disease analyzed the role of clopidogrel on circulating progenitor cells, as EPCs, at baseline and at the end of the treatment period [26]. The progenitors remained unchanged in the two groups, and Ronnie Ramadan hypothesed the pleiotropic effects of clopidogrel as reduction of inflammation.
Although CAS is considered a traumatic procedure for the arterial wall, its actual effect on cells is not yet well known for heterogeneous clinical results related to different vascular territories, a small number of patients, various assessments of EPCs [27–30]. The EPCs identification is difficult for their ability to express a wide variety of typical endothelial markers, with different intensity and time expression [31, 32]. Furthermore, the comparison is not always feasible because many patients may exhibit different stem cell mobilization for the presence of several comorbidities [33]. In our pilot study, we tried to reduce common factors influencing the EPCs number and mobilization, such as major cardiovascular events occurred in the previous 6 months, the presence of cancer, severe kidney failure and advanced heart failure (class III-IV NYHA). We observed that high doses of clopidogrel administration before CAS influenced CD34+/CD133+ and CD34+/VEGFR-2+ cells, in order to have a reduction to 14 days compared to baseline. This observation could imply a less EPCs homing due to a reduction of available circulating pool.
Previous examinations focused on the angiogenic chemokine receptor as CXCR2, expressed on EPCs and causing homing arrest to sites of arterial injury [34]. Furthermore, SDF-1α/CXCR4 axis triggered adhesion and appeared more crucial in mediating EPCs transmigration, as confirmed in mouse carotid arteries after wire-induced denudation [35].
In our study, the expression of CXCR2 receptor tends slightly to decrease over time. In particular, it is lower at 14 days in the group with a loading dose of clopidogrel before CAS.
The concentration of SDF-1α remains quite stationary in the Pre-CAS group without observing the concentration peak at six hours as in the Post-CAS group. We hypothesize that high doses of clopidogrel before the procedure could be able to reduce the release of SDF-1α into the bloodstream.
The known correction of common risk factors such as diabetes, hypertension, dyslipidemia and smoking reduces the incidence of late atherosclerotic in-stent restenosis but it has not significant effect on early neointimal hyperplasia, suggesting that other factors can play a key role, especially in the first months [2, 36]. Andreas Schober hypothesized that changes in the EPCs, defined as CD34+, due to the vascular trauma associated with stenting implantation could predict the risk of coronary in-stent restenosis due to neointima proliferation in spite of chronic stent thrombosis [37]. He found a positive correlation between the post-procedural increase of EPCs and late lumen loss at follow-up in 17 patients, suggesting that changes in circulating CD34+ cells could be a predictive marker for the development of coronary in-stent restenosis in humans.
A prospective multicenter study, performed by Bonello, showed how mobilization of EPCs is responsible for neointimal hyperplasia on stent, in-stent restenosis and consequent lesion revascularization [38]. A subanalysis of the IN-PACT CORO trial supports a dual role for EPCs to induce stent endothelialisation, but also in promoting intimal hyperplasia [39].
In our study, the Pre-CAS group showed a lower intima-media thickness since the first control at 3 months, and stable reduction at 6 and 12 months. We hypothesize that high doses of clopidogrel before stenting have a clear implication in SDF-1α reduction, avoiding the early peak observed in the Post-CAS group, with reduction of local inflammation and platelet adhesion, subsequent decline in circulating endothelial cells mobilization and homing, influenced by a slightly reduced expression of CXCR2 and CXCR4 receptors in the following period, associated with a decrease neointimal hyperplasia on carotid stent.
Considering that 82% of patients undergoing CAS used dual antiplatelet therapy with ASA and clopidogrel [15], the adequate timing for the loading dose of clopidogrel is of paramount significance for clinical management and adequate treatment.
The significant decrease in blood pressure observed immediately following CAS was already described in a previous study [23], as a consequence of the vascular wall stretching and baroreceptors stimulation. The hypotension occurs in 19–51% of patients but is usually transient and rarely symptomatic. Also bradycardia is common, a reported incidence of 2.3–37% and in a study population we reported a trend [18].
We believe that the main limitation of our study is the sample size, but we have taken into account many factors as exclusion criteria that negatively influence production, mobilization and activation of EPCs such tumors, cardiovascular events, renal failure, medical treatments and material used for the stent. We do not have IMT data on common carotid free to atherosclerotic process before stenting; we think that, in future studies, it would be important to a possible correlation of intrastent neointimal hyperplasia. We also believe that, as for coronary angioplasty, it would be useful to know the clopidogrel resistance of each patient to undergo carotid stent in order to adjust the loading dose. In light of this, we believe that our investigation is a pilot study that requires further investigation on a larger number of patients to confirm the data obtained on cells and to replicate the association found on carotid intima-media thickness.
Conclusions
In this study, we have considered the vascular damage induced by CAS evaluating in vivo cellular changes. Clopidogrel loading dose before stenting modifies both acute mobilization of EPCs and platelet activation, with a significant reduction of intimal proliferation on carotid stenting at 12 months. In our opinion, this investigation, although small, offers the starting point for further research in vitro and in vivo cell-cell interaction modulated by antiplatelet agents currently used in clinical practice.
Funding
This study was partially funded by the units of Cardiology and Onco-hematology of the Research Hospital “Casa Sollievo Della Sofferenza” of San Giovanni Rotondo, Italy. The sources of funding had no involvement in the research or preparation of this article.
Conflict of interest
The authors report no relationships that could constitute a conflict of interest.
Footnotes
Acknowledgments
The authors would thank Mr Luigi Di Carlo, Mr Antonio Cursio, Mr Michele Libergolis, Mr Antonio D’Ambrosio and nurses of the unit of cardiology, vascular surgery and laboratory analysis units of the Research Hospital “Casa Sollievo Della Sofferenza” for their valuable work.