
Abstract
PURPOSE:
To retrospectively evaluate the role of intraoperative ultrasonography (IOUS) and contrast-enhanced IOUS (CE-IOUS) for the patients with hepatocellular carcinoma (HCC) undergoing hepatic resection (HR).
METHODS:
Twenty-one consecutive patients who had undergone HR for HCC were included in this study. The patients were subject to preoperative imaging modalities including preoperative ultrasonography (Pre-US) and preoperative contrast-enhanced ultrasonography (Pre-CEUS). All the patients then underwent intraoperative ultrasonography (IOUS) and contrast-enhanced intraoperative ultrasonography (CE-IOUS) during surgery. The visualization of primary HCC and additional lesions of all patients were analyzed.
RESULTS:
Twenty-one HCCs were detected during Pre-US and the remaining six lesions (28.6%) were detected during IOUS and CE-IOUS. Thus the treatment plan was changed in 28.6% of patients. Twenty-one HCCs (diameter, 0.6–3.0 cm; mean±SD, 1.98±0.85 cm) were measured on Pre-US and remeasured on IOUS (diameter, 0.9–3.3 cm; mean±SD, 2.19±0.84 cm) (p < 0.001). The 6 additional lesions consisted of three moderately differentiated HCCs, one cholangiocarcinoma (ICC), and two high-grade dysplastic nodules (DNs). The mean maximal diameter of the 6 additional lesions was 0.83 cm (range: 0.6–1.1 cm). The malignancy associated features such as capsule interruption, echo heterogeneity, hypo-echoic rim, and a nodule in nodule pattern were more often depicted on IOUS than on Pre-US (all p < 0.01). On CEUS, 19 (90.5%) of 21 HCCs were hyper-enhanced in the arterial phase and washed out from the portal phase to the late phase; the remaining two (9.5%) were hypoenhanced. On CE-IOUS, tumor vasculatures were classified as four patterns: 11 (52.4%) exhibited netlike pattern, 7 (33.3%) annular pattern, 2 (9.5%) mixed pattern, and 1 (4.8%) radial pattern. 3 mHCCs and 2 DNs of six additional nodules had similar greyscale imagining features on IOUS, but they showed different enhancement patterns on CE-IOUS. The ICC showed slightly heterogeneous enhancement during the arterial phase and hypo-enhancement during the portal phase.
CONCLUSIONS:
IOUS detects more lesions and the treatment plan is changed in 28.6% of patients. HCCs were larger on IOUS than on Pre-US. The typical imaging features of HCCs were better depicted on IOUS in comparison with Pre-US. CE-IOUS can catch the details of microcirculation perfusion of HCCs more sensitively than CEUS. Both IOUS and CE-IOUS were able to provide more decision information during surgery.
Keywords
Introduction
Hepatocellular Carcinoma (HCC) is an epithelial tumor with high malignancy in the liver and is the third most common cause of cancer-related death worldwide [1]. In China, chronic hepatitis B virus (HBV) infection is the leading cause of cirrhosis, liver failure and HCC [2]. Hepatic resection (HR) is the first-line treatment for hepatic malignancy in patients with sufficient liver function reserve conditions. During surgical process, the management strategy of HCC largely depends on the accuracy of the imaging diagnosis. Intraoperative ultrasonography (IOUS) of the liver has been considered to be a fundamental step in HR, which supplies additional information in up to 38% of surgical procedures [3–5]. IOUS also remains the best real-time imaging technique for the evaluation of HCCs during laparoscopic and open surgery [6]. With these data that can make changes in surgical management, HR exhibits additional efficacy and safety.
In general, various scanning techniques may be used before and after operational managements, such as computed tomography (CT), Magnetic Resonance Imaging (MRI), baseline ultrasonography (BUS), and contrast-enhanced ultrasonography (CEUS). Among these, BUS examination is the most widely applied imaging tool for preoperative, intraoperative, and postoperative screening and surveillance of HCC. The ability of dynamic contrast enhanced ultrasound (DCEUS), visualizing dynamic perfusion changes, might be of advantage in displaying significant differences between malignant liver tumors [7] and residual tumor tissue [8]. During surgery, IOUS and contrast-enhanced intraoperative ultrasonography (CE-IOUS), based on the technology of BUS and CEUS, are the most commonly used and these are convenient imaging tools. CE-IOUS offered the advantage of locating extra liver nodules (27%) when comparing with preoperative MRI and preoperative CEUS(Pre-CEUS) [9].
These preoperative examinations are helpful to evaluate the whole of lesion and liver disease, but they are a bit difficult to detect and identify the tiny lesions. The IOUS and CE-IOUS can overshadow the preoperative ultrasound because they are more sensitive in identifying the small structure of these lesions. However, that requires inspectors to have more comprehensive abilities. Even when the surgical administration is not modified by IOUS and CE-IOUS, it is likely to result in a correction of disease staging [10]. The purpose of this study is to retrospectively assess the role of IOUS and CE-IOUS for the patients with HCC undergoing HR.
Patients and methods
Patients
From February 2014 to January 2016, 21 consecutive patients (mean age±SD, 54.0±8.3 years; range, 34–67 years; 3 females and 18 males) who underwent HR together with IOUS and CE-IOUS for imaging of HCC at Nantong Third Hospital of Jiangsu Province, China, were included for this retrospective study. A multidisciplinary group, which consisted of surgeons, sonographers, radiologists, and hepatologists, determined the diagnosis and treatment method for the patients with HCC. The imaging diagnostic and staging workup for HCCs were built on the appropriate imaging regimen, including CT and/or MRI, Preoperative US(Pre-US), and Pre-CEUS. Histological assessment was required in all cases. Fifteen patients were associated with cirrhosis and six had chronic hepatitis. Inclusion criteria were as follows: diagnosis of HCC, with a diameter≤3 cm; liver nodule with availability of Pre-US and Pre-CEUS, CT, and/or MRI findings; and availability of IOUS and CE-IOUS findings. The baseline characteristics of the enrolled patients were summarized as in Table 1. A change in operative stage was defined as one in the type of HR on the basis of IOUS and CE-IOUS findings, compared with the pre-operative strategic resection. The pre-operative plan documented at the multidisciplinary team (MDT) took place several weeks before the operation. The surgical strategy was classified as similar, extended, limited or cancelled. When additional malignant lesions were found on IOUS and CE-IOUS, the manner was responsible for a change in the operative strategy. Written informed consent were obtained from all the enrolled patients and the approval of the institutional ethics committee was obtained for this study. The number of the approval from the ethics committee wasE20150016.
Clinical characteristics of enrolled patients with HCC who underwent surgery
Clinical characteristics of enrolled patients with HCC who underwent surgery
The US system iU-Elite (Philips, USA) was utilized in all the cases for Pre-US exams and a convex array probe of 5–1 MHz was used. Before contrast agent injection, the baseline Pre-US scanning plane of the whole liver, including the HCC, was obtained. For the previously diagnosed patients, the liver parenchyma was also scanned carefully.
Pre-CEUS was then performed with the same 5–1 MHz convex array transducer. This transducer has the capacity for CEUS on preoperative studies. SonoVue (Bracco Imaging, Milan, Italy) was used as the US contrast agent, which comprised sulphur hexafluoride microbubbles stabilized by a phospholipid shell before administration within 5 mL sterile saline. For each exploration, 2.4 mL of SonoVue was injected intravenously as a bolus through the central venous line, followed by a 5.0 mL saline flush. A low mechanical index (MI) of 0.11 was set. During the CEUS procedure, a real-time fundamental mode image was shown synchronously with a pulse inversion harmonic image side-by-side for contrast. Lesion characterization and new nodule were detected by CEUS scan. After intravenous injection of the contrast agent, the contrast enhancement pattern was determined by evaluating the behavior of the contrast agent throughout the CEUS examinaton. The whole vascular phases of contrast enhancement, including arterial phase (10–20 s to 25–35 s following the injection), portal phase (30–45 s to 120 s), and late parenchymal phase (>120 s) phases, were recorded and analyzed.
IOUS and CE-IOUS examination
Two linear array probes of 12–5 MHz and 9–3 MHz were used for IOUS and CE-IOUS. These transducers have the capacity for CEUS on intraoperative studies. Before contrast agent injection, the baseline IOUS scanning plane of the whole liver, including the HCC, was obtained. The liver parenchyma was scanned carefully, as were new lesions, for any major vascular or biliary involvement on IOUS.
For each CE-IOUS exploration, 4 mL of SonoVue was injected intravenously as a bolus through the central venous line, followed by a 5.0 mL saline flush. A low mechanical index (MI) mode (MI = 0.11) was set and a dual-display mode was used in that a real-time gray scale image was shown synchronously with a contrast image side-by-side. Lesion characterization and new nodule were detected by CE-IOUS scan. After intravenous injection of the contrast agent, the contrast enhancement pattern was determined by evaluating the behavior of the hepatic tumor throughout the CE-IOUS examination.
Image analysis
The preoperative and intraoperative scans were performed by two senior board-certificated sonographists of over five-year experience the abdominal US. The image evaluation was performed independently by two US experts of fewer than five-year experience using IOUS and CEUS, both of whom assessed the images recorded on videotape and disks. In cases of differences, the experts reviewed the saved images together and re-evaluated their findings for the final diagnosis. They were blinded to the US report and pathologic data during image evaluation.
The following characteristics were requested to record regarding the Pre-US and IOUS patterns according to diameter, echogenicity (hypoechoic or hyperechoic), echotexture (homogeneous or heterogeneous), nodular margin (well-defined or infiltrative), hypo-echoic rim, capsular interruption, mosaic pattern, a nodule-in-nodule (NIN) pattern, satellites (identification of small nodules within 2 cm from the major HCC lesion) (Fig. 1) and vascular/biliary micro-infiltration. Microinvasive hepatocellular carcinoma (MI-HCC) was defined as a neoplasm with vascular/biliary infiltration and/or the existence of satellites [11]. For Pre-CEUS and CE-IOUS, the whole vascular phase of contrast enhancement was recorded and analyzed.
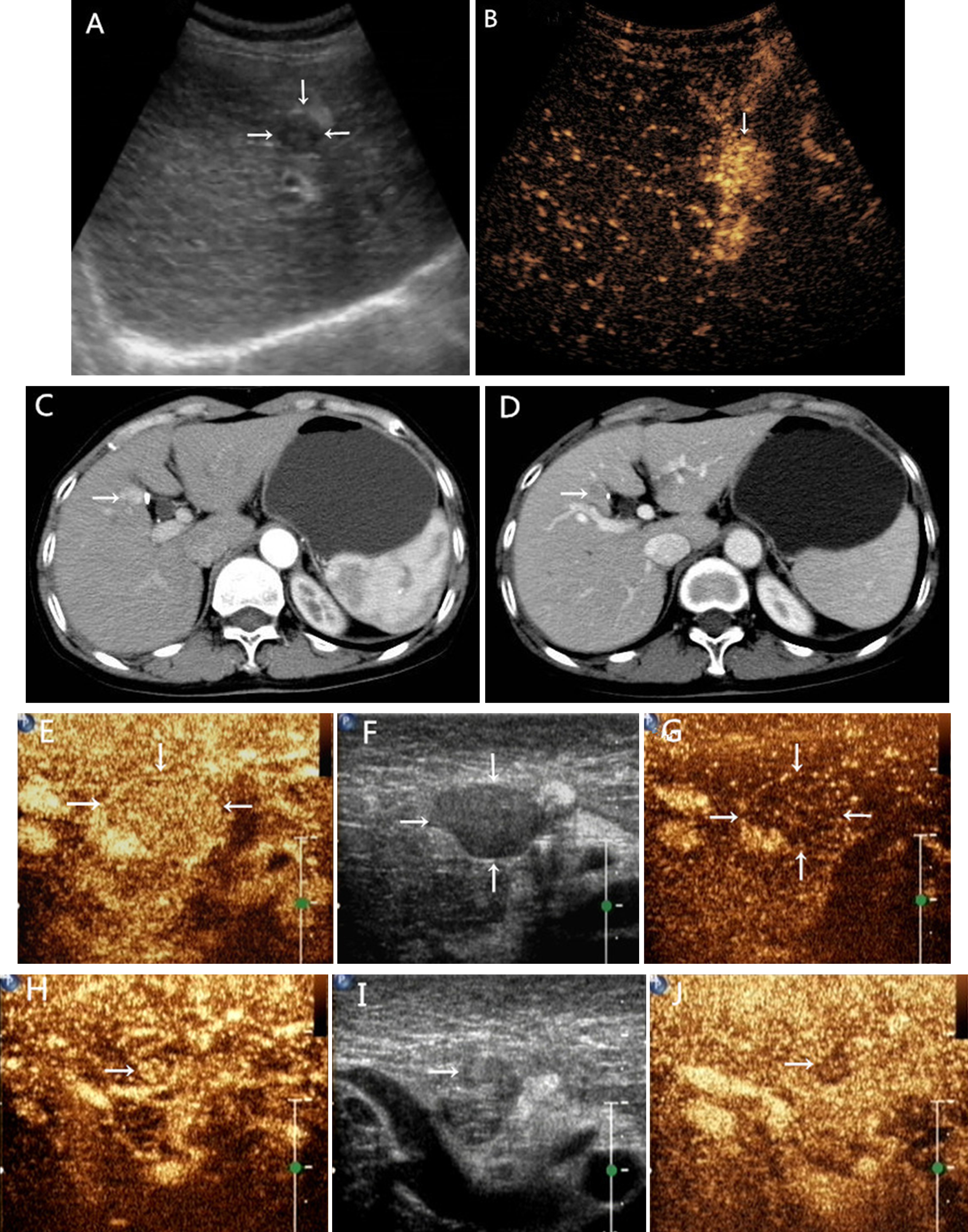
A 50-year-old woman with hepatitis B-related liver cirrhosis and a small HCC (maximum diameter, 1.8 cm) in segment V. A. Pre-US image shows a hypoechoic HCC nodule with a thin tumor encapsulation (arrow). B. On CEUS, 18 seconds after contrasting agent administration, homogeneous hyperenhancement of the nodule (arrow) is observed. C-D. Computed tomography scan in the arterial phase shows a small lesion with arterial hypervascularity and venous phase washout. E-G. IOUS shows hyperechoic nodule with a thin tumor encapsulation. Serial contrast-enhanced images obtained 20 seconds (E) and 48 seconds (G) after contrast agent administration show hyper-enhancement of the lesion in arterial phase(E) and hypo-enhancement in the venous phase(G). H-J. CE-IOUS shows an additional 0.6 cm isoechoic nodule with thick hypoechoic rim (arrow) near the HCC not identified at preoperative US, CEUS, and CT. The lesion (arrows) shows slight hyper-enhancement 21 seconds (H) and hypo-enhancement 40 seconds (J) after contrast agent administration.
SPSS version 19.0 (SPSS, Chicago, USA) was used to create a database for statistical analysis. Comparisons of pathological characteristics and imaging features for significance were performed with a χ2 test or t-test to analyse the data; a value of p < 0.05 was considered to be statistically significant.
Results
Findings of Pre-US and IOUS
Twenty-seven malignant lesions in the 21 patients were observed during pathologic examinations. A total of 21 nodules (diameter, 0.6–3.0 cm; mean±SD, 1.98±0.85 cm) were measured on Pre-US and remeasured on IOUS (diameter, 0.9–3.3 cm; mean±SD, 2.19±0.84 cm) (p < 0.001). The 21 nodules were confirmed to be HCCs, which appeared as hypoechoic nodules in 16 (76.2%) on Pre-US and 15 (71.4%) on IOUS (Fig. 1A, F), and as hyperechoic nodules in 5 (23.8%) and 6 (28.5%) respectively (Fig. 6A, B) (p = 1.00) (Table 2). Sixteen HCCs (76.2%) exhibited tumor encapsulation and 3 (14.3%) exhibited posterior acoustic enhancement on both Pre-US and IOUS (p = 1.00).
Tumor features of HCC on Preoperative and Intraoperative US
Tumor features of HCC on Preoperative and Intraoperative US
*Six of 27 lesions only detected intraoperatively are not summarized in statistics and analyses in this table.
However, capsule interruption was more frequently observed on IOUS (93.7%) than on Pre-US (31.2%) (p = 0.002 and χ2 = 8.1) (Fig. 2A-B). The mosaic pattern on IOUS was slightly higher than on Pre-US (28.6% vs 9.5%, p = 0.125 and χ2 = 2.75). The imaging features of HCCs on Pre-US and IOUS examinations, such as the echo heterogeneity, hypo-echoic rim, and a NIN pattern were respectively described and recorded. The frequency of occurrence for these features of HCCs detected on IOUS [18 (85.7%), 15 (71.4%) and 11 (52.4%)] was significantly higher than on Pre-US [eight (38.1%), five (23.8%), and three (14.3%) (p < 0.01) (Table 2). Compared with Pre-US, the hypo-echoic rim and tumor encapsulation on IOUS were not only clearer, but also thicker, irregular, and incomplete (Figs. 2A-B, 5A-B). In addition, with more frequent detection of mosaic patterns, more echo heterogeneous phenomena were seen (Fig. 2B). During surgery, vascular micro-infiltrations were detected in two (9.5%) of 21 HCCs by IOUS, and satellites in two (9.5%)(Fig. 1H-J). MI-HCC was defined by the presence of vascular micro-infiltration and satellites in four (19.0%) (p = 0.125 and χ2 = 2.25) (Table 2).

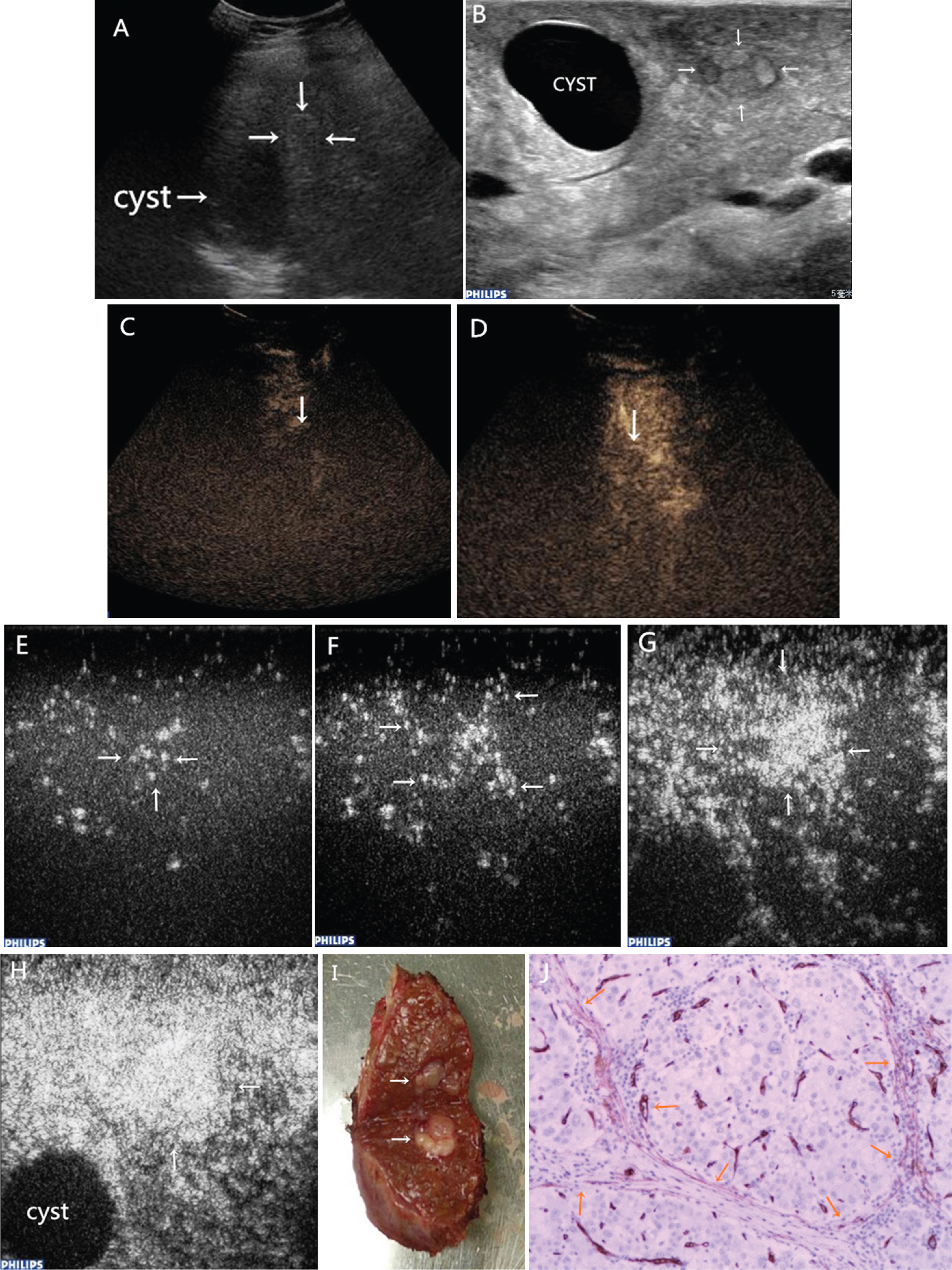
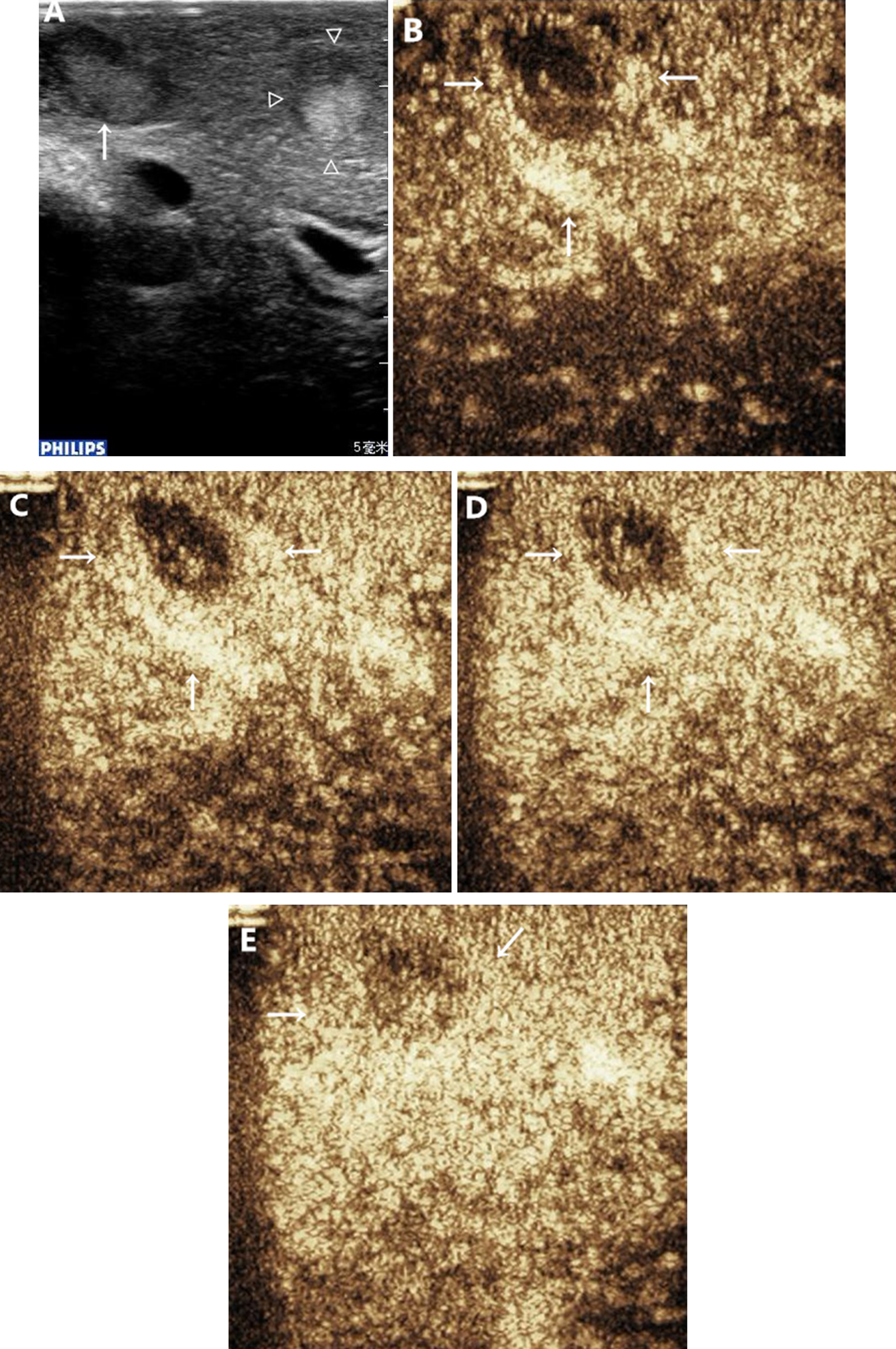
A 51-year-old man with hepatitis B-related liver cirrhosis and a small HCC (maximum diameter, 1.0 cm) in segment V. A. Pre-US image shows a hypoechoic HCC nodule with posterior acoustic enhancement (arrow). B. IOUS image shows a heterogeneous lesion with thick, irregular and incomplete hypo-echoic rim and tumor encapsulation. C. CEUS shows hyper-enhancement 19 seconds (C) after contrast agent administration. D-G. Serial contrast-enhanced images obtained 16 seconds (D), 18 seconds (E), 20 seconds (F), and 22 seconds (G) after contrast agent administration show hyper-enhancement with a netlike enhanced pattern on CE-IOUS. H. Postoperative specimens. I. Immunohistochemical staining of anti-CD34 in sinusoid-dominant type (100×200).
The images of CEUS and CE-IOUS were respectively evaluated and classified during the arterial phase. On CEUS, 19 (90.5%) of 21 HCCs were hyper-enhanced in the arterial phase and washed out from the portal phase to the late phase; the remaining two (9.5%) were hypo-enhanced. The hyper-enhanced group included two patterns: homogeneous and annular hyper-enhancement. Thirteen (61.9%) were homogeneous (Figs. 1B, 2C) and six (28.6%) were annular hyper-enhancements, which began with the early arterial phase of the transient annular hyper-enhancement and fulfilled the precedent pattern by rapidly filling in a cyclic shape (Fig. 4C-F). The hypo-enhanced group showed two patterns: one exhibited hypo-enhancement from arterial phase to portal phase (Fig. 3C-D) and the other exhibited hypo-enhancement in arterial phase and peripheral enhancement in portal and delayed phase (Fig. 6C-F).
A 63-year-old man with hepatitis B-related liver cirrhosis and a small HCC (maximum diameter, 1.0 cm) in segment IV. A cyst is near it. A. Pre-US image shows a hypoechoic HCC nodule with capsula (arrow). B. IOUS image shows a heterogeneous isoechoic lesion with a NIN pattern surrounded with thin, irregular and incomplete hypo-echoic rim and interruptive capsula. C-D. CEUS shows hypo-enhancement 19 seconds (C) and 47 seconds (D) after contrast agent administration. E-H. Serial contrast-enhanced images obtained 17 seconds (E), 19 seconds (F), 21 seconds (G), and 25 seconds (H) after contrast agent administration show hyper-enhancement with radial enhanced pattern in the arterial phase. I. Postoperative specimens appears a NIN pattern. J. Immunohistochemical staining of anti-CD34 in sinusoid-dominant type (100×200).
According to CE-IOUS findings, tumor vasculatures were classified as four patterns: 11 (52.4%) exhibited netlike pattern (Fig. 2D-G), 7 (33.3%) annular (ring-shaped) pattern (Figs. 5D-G, 6G-J), 2 (9.5%) mixed pattern (consisting of netlike and annular patterns) (Fig. 4G-J), and 1 (4.8%) radial pattern (Fig. 3E-H). Except for the annular pattern, the others were not observed preoperatively by Pre-CEUS. Eleven (84.6%) of 13 homogeneously hyper-enhanced HCCs on Pre-CEUS appeared as netlike patterns on CE-IOUS, while the others (2/13, 15.4%) showed mixed pattern. Six (100%) annular hyper-enhanced HCCs on Pre-CEUS were also annular on CE-IOUS. The remaining two hypo-enhanced HCCs on Pre-CEUS showed two patterns on CE-IOUS, incompletely annular and radial patterns.
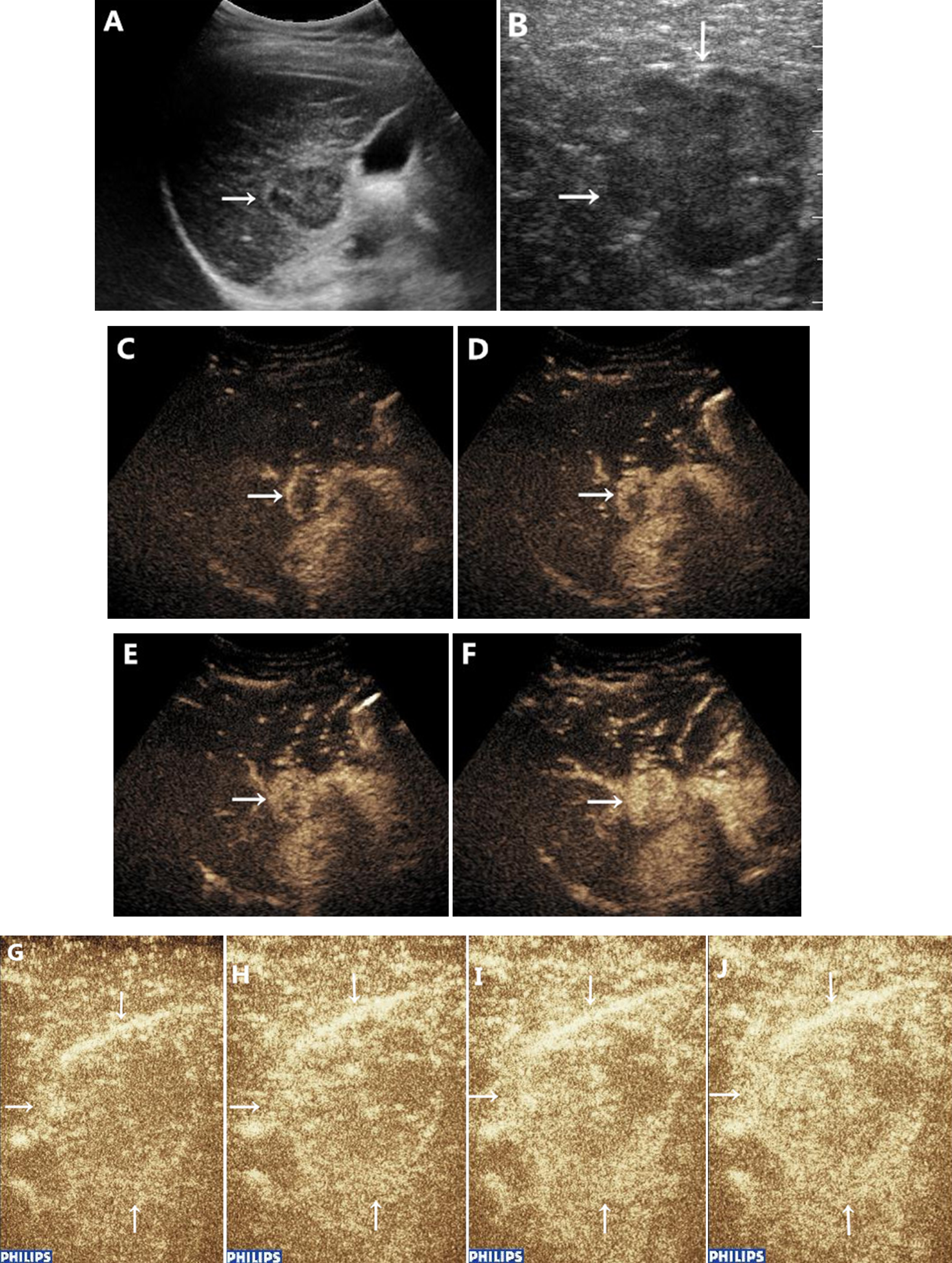
A 42-year-old woman with hepatitis B-related liver cirrhosis and a small HCC (maximum diameter, 3.0 cm) in segment V. A. Pre-US image shows a heterogeneous hypoechoic HCC with irregular capsula (arrow). B. IOUS image shows an irregular hypoechoic nodule with interruptive capsula. C-F. Serial contrast-enhanced images obtained 15 seconds (C), 16 seconds (D), 17 seconds (E) and 19 seconds (F) after contrast agent administration show annular hyper-enhancement in the arterial phase. G-J. CE-IOUS shows hyper-enhancement with mixed enhanced pattern 12 seconds (G), 14 seconds (H), 16seconds (I) and 21 seconds (J) after contrast agent administration.
A 57-year-old man with hepatitis B-related liver cirrhosis and a small HCC (maximum diameter, 2.0 cm) in segment VII. A. Pre-US image shows a heterogeneous hypoechoic HCC with NIN pattern and capsula (arrow). B. IOUS image shows a NIN nodule with thick, irregular and incomplete hypo-echoic rim and capsula. C. CEUS shows hypo-enhancement 28 seconds after contrast agent administration.. D-G. CE-IOUS shows annular hyper-enhancement 19 seconds (G), 21 seconds (H), 25seconds (I) and 30 seconds (J) after contrast agent administration.

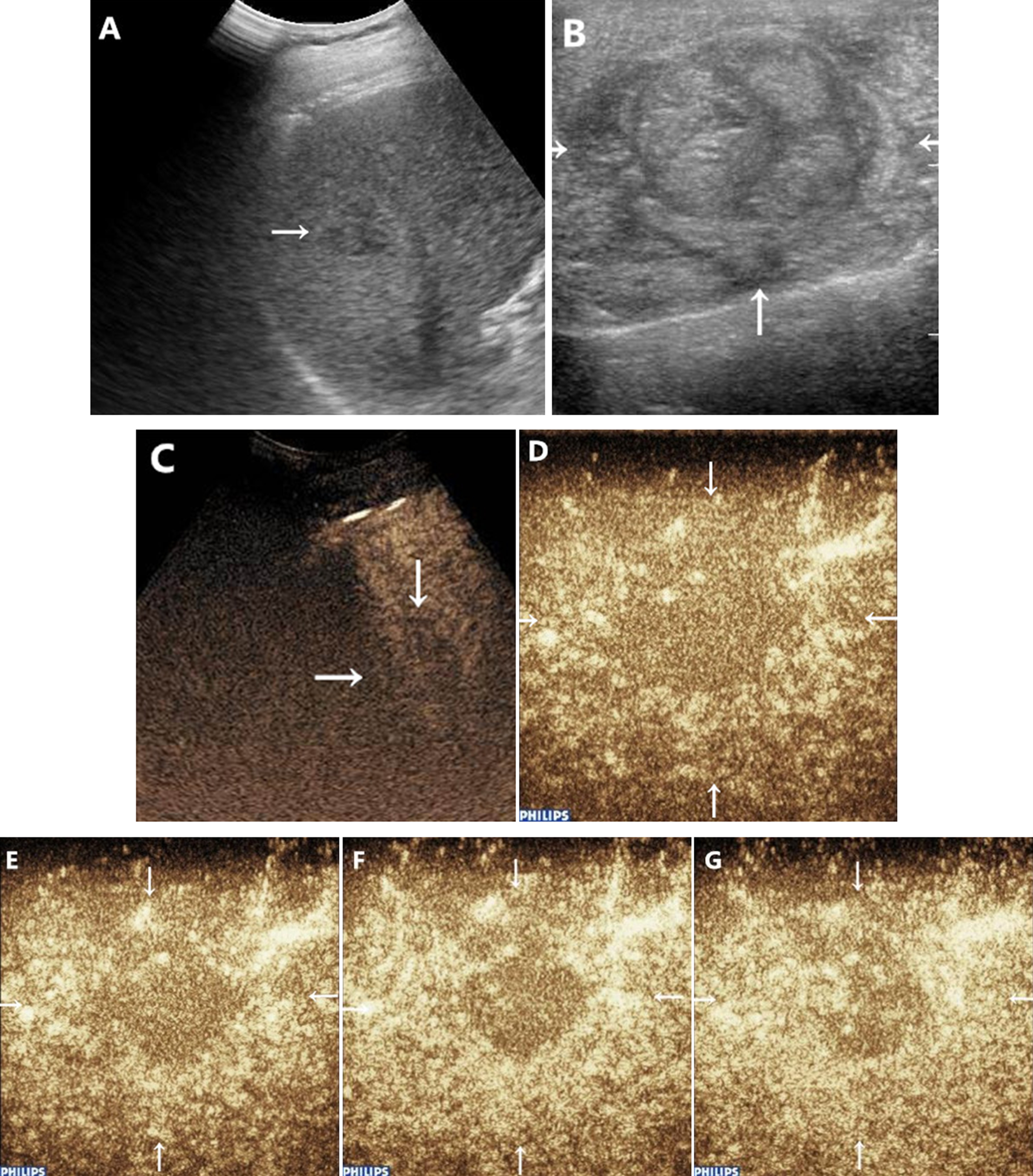
A 56-year-old woman with hepatitis B-related liver cirrhosis and a small HCC (maximum diameter, 1.0 cm) in segment VII. A. Pre-US image shows a hyperechoic HCC with hypo-echoic rim (arrow). B.IOUS image shows a homogeneous hyperechoic nodule with irregular hypo-echoic rim. C-F. Serial contrast-enhanced images obtained 19 seconds (B), 26 seconds (C), 35 seconds (C), and 42 seconds (D) after contrast agent administration show hypo-enhancement in the arterial phase and annular hyper-enhancement in the portal and late phases. G-J. CE-IOUS shows annular hyper-enhancement 15 seconds (G), 18 seconds (H) and homogeneous hyper-enhancement 21 seconds (I), and 23 seconds (J) after contrast agent administration.
During IOUS and CE-IOUS imaging studies, six additional nodules were detected in six (28.6%) of the 21 patients, including 3 mHCCs, 1 intrahepatic cholangiocarcinoma (ICC), and 2 high-grade dysplastic nodules (DNs). Surgical managements were altered on the basis of the IOUS and CE-IOUS findings in six of 21 patients (28.6%). Surgeries were extended in all of these 6 patients detected additional nodules. None of these 21 surgeries was limited, or cancelled.
The mean maximal diameter of those nodules was 0.83 cm (range: 0.6–1.1 cm) (Fig. 1H-J). One satellite HCC was found behind the major HCC, one HCC and two DN were within 2 cm of the major HCC lesion, and the remaining mHCC and ICC were located in other segments. One of the three mHCCs and one DN exhibited hyperechoic nodule with a thick hypo-echoic rim on IOUS (Figs. 1I, 7A), while the remaining two mHCCs, DN, and cholangiocarcinoma exhibited homogeneous hypoechoic nodules on IOUS.
A 51-year-old man with hepatitis B-related liver cirrhosis for 10 years and a small HCC (maximum diameter, 2.5 cm) in segment V (triangle). During surgery, a DN within 2 cm around the HCC lesion was detected in segment V (maximum diameter, 1.0 cm) (arrow). A: IOUS image shows that the DN was a hyperechoic nodule with hypo-echoic rim (arrow). A part of HCC shows a heterogeneous hyperechoic nodule with thick, irregular, hypoechoic rim (triangle). B-E: Serial contrast-enhanced images obtained 14 seconds (B), 17 seconds (C), and 20 seconds (D) after contrast agent administration show peripheral hyper-enhancement and heterogeneous iso-enhancement (arrow) 33 seconds (E)after contrast agent administration.
The three mHCCs showed rapidly overall hyper-enhancement during the arterial phase and hypo-enhancement during the portal phase on CE-IOUS (Fig. 1H-J). One of two DNs showed peripheral hyper-enhancement (arrows) in the arterial phase and heterogeneous iso-enhancement in the portal phase of CE-IOUS (Fig. 7B-E). The remaining DN showed delayed enhancement during the arterial phase, iso-enhancement during the portal phase, and washed out in the late phase. The three mHCCs had different greyscale manefestations on IOUS but showed the same enhancement pattern on CE-IOUS. Two DNs had different greyscale manifestations on IOUS and the enhancement patterns were also different on CE-IOUS. Although mHCCs and DNs had similar greyscale imagining features on IOUS, they showed different enhancement patterns on CE-IOUS. The ICC showed slightly heterogeneous enhancement during the arterial phase and hypo-enhancement during the portal phase.
Preoperative hepatic imaging examinations, such as CT, MRI and positron emission tomography (PET), have improved considerably in recent years. Sahani et al. [12] reported that MRI was as sensitive as IOUS in depicting hepatic lesions before HR (86.7% and 94.3%, respectively). There was no statistical significance of CEUS and MRI regarding the general differential diagnosis for hepatic tumor [9]. However, classical features of HCC on BUS, such as ring sign, a nodule in nodule, septum and posterior echo enhancement, are often observed in advanced HCC [13] and not available for those <2 cm in diameter [14]. It is difficult to determine whether these lesions are HCCs, especially those which measure≤2 cm in diameter [15]. During the long process of the carcinogenesis of HCC, the neovascularization in small lesion may be invisible with the current imaging approaches [16, 17]. Xu et al. [18] showed that diagnosing HCCs≤2.0 cm diameter by CEUS needs further investigation. In our study, six additional malignant nodules (28.6%) of 21 patients were detected and confirmed by IOUS and CE-IOUS during surgery (Figs. 1, 7).
The 6 additional lesions in six patients who had underwent MRI or CT, US and CEUS before surgery, while were invisible on all of them. Five (83.3%) of them were <1.0 cm and the remaining one (16.7%) was 1.1 cm. Although mHCCs and DNs had similar greyscale imagining features on IOUS, the CE-IOUS patterns of these HCCs were hyper-enhancement in the arterial phase and washout in the portal phase, which was different from those of ICC and DN (Fig. 7B-E).
The intralesional vascularity determined primarily the nature of small lesions. The contrast-enhancement patterns of 21 HCC on CE-IOUS were also different from Pre-CEUS. The HCC in Fig. 3 showed radial enhancement on CE-IOUS while hypo-enhancement on Pre-CEUS. The pattern on CE-IOUS was due to that the vessel was wedged into the centre of the nodules (a NIN pattern). These two patterns, the NIN pattern and radial enhancement, exhibited difficulty on Pre-US and Pre-CEUS in nodule diameter≤1 cm. Compared with the pattern of homogeneous hyper-enhancement on Pre-CEUS, CE-IOUS could appear netlike patterns, the detail of the tumor angiogenesis, which was due to that the tumor was surrounded by the globular vascular network (Fig. 2D-G). Annular hyperenhancements are frequently observed in haemangiomas, the most common benign tumor found in the liver. Centripetal fill-in enhancement was a positive finding to diagnose hemangioma [19]. When the enhanced pattern presents in HCC (Fig. 4), it should be differentiated from hemangioma.
The study of Numata et al. [20] showed that 83 early HCCs detected by BUS showed hypo-echoic rim in two (1.9%) and NIN pattern in three (3.6%); none of them exhibited mosaic pattern. Besides, HGDN (0/6) had no hypo-echoic rim. Compared with the results from Numata’s study, 21 HCCs in this study showed hypo-echoic rim in 15 (71.4%) on IOUS, mosaic pattern in 6 (28.6%), and NIN pattern in 11 (52.4%); one of two HGDNs (50%) showed hypo-echoic rim which was higher than that seen on Pre-US, similar with Numata’s findings. The infiltrative aspects of nodules on IOUS, such as hypo-echoic rim, capsular interruption, and NIN pattern were all significantly higher than on Pre-US. These changes may explain why the diameters measured by IOUS were larger than Pre-US. Mosaic and NIN pattern were detected in nodule diameter≥1 cm on Pre-US, but on IOUS, they could be detected in nodule diameter <1 cm (Fig. 3B, I).
The early detection of small HCC allows new chance for a successful surgery [21, 22]. In fact, the typical imaging features, lead to highly specific diagnosis of HCC and closely relative to HCC, have existed in the period of small HCCs (even if diameter <1 cm), but it is difficult to be found in small HCCs on Pre-US. With the limit of preoperative diagnostic imaging criteria, the Transplantation Network (OPTN) /United Network for Organ Sharing (UNOS) [23, 24] and the Liver Imaging Reporting and Data System (US LI-RADS) [25] suggested not to diagnose HCC <1 cm in diameter. Our study found that homogenous hypoechogenicity (76.2%) with tumor encapsulation (76.2%) was frequently observed during imaging of small HCCs with a low-frequency probe on Pre-US. In our study, the livers were scanned with the high-frequency probe instead of low-frequency probe during HR. The high-resolution pictures had shown that the imaging characteristics of 21 HCCs on IOUS were different from Pre-US (Table 2). In contrast to Sahani’s opinion [12], our study showed that IOUS examination could identify the typical imaging signs of small HCC (even if diameter <1 cm), which were associated with histologicfeatures.
A major limitation of this study was that it was a retrospective study. Furthermore, there was no enough investigation for the additional lesions detected during surgery of HCC and DN in diameter≤1 cm, and lack of comparison with RN. Because the exploration of HCCs in the context of cirrhosis was more complicated, because the diagnoses from IOUS and CE-IOUS protocols in these patients may be influenced by operator’s experiences and the extent of hepatic cirrhosis.
In summary, IOUS not only detected additional lesions and changed the management plan, but also showed more typical aggressive growth signs of HCC than preoperative the examination. CE-IOUS could more sensitively catch the details of microcirculation perfusion and display more plentiful enhanced patterns of HCCs than CEUS. The imaging features on IOUS and CE-IOUS of HCC provided more confidence to the operators to diagnose the HCC rapidly and accurately during surgery.