
Abstract
BACKGROUND:
Negative pressure wound therapy applied over closed incisions (ciNPT) has been shown to influence wound healing. Therefore, the aim of this study was to examine the short-term effects of ciNPT on skin perfusion patterns in postbariatric wounds.
METHODS:
17 patients were included. Patients from the study group received a ciNPT dressing with a continuous negative pressure of – 125 mmHg for five days. Two intra- and two postoperative measurements were performed using both a combined laser Doppler spectrophotometry and an ICG angiography system to determine oxygen saturation (sO2), hemoglobin content (rHb) and perfusion patterns.
RESULTS:
Three days postoperatively the sO2 was significantly higher in the study group compared to the control group and also compared to the end of the operation. Concerning the rHb, there was no statistical significant alteration in or between the groups, but a trend towards a correlated alteration of sO2 and rHb. ICG angiography showed an earlier and stronger enhancement of perfusion parameters in the study group.
CONCLUSION:
CiNPT has a positive effect on oxygen saturation and tissue perfusion, which are both associated with the wound healing process. The use of ciNPT could therefore possibly reduce the risk of wound healing complications in this high-risk patient group.
Keywords
Introduction
Along with a dramatic increase of obesity, the number of bariatric surgery, as an effective strategy for long-acting weight loss is increasing steadily [1, 2]. Due to the massive weight loss, a large population of postbariatric patients remains with the problem of excessive skin and fat, which not only affects their body image but also involves functional health issues, such as chronic skin irritations and reduced quality of life [3]. Consequently, those patients are more frequently requiring body contouring procedures, where abdominoplasty is the most commonly performed one [4]. Besides the positive influences of body contouring surgery on patients’ self-image and functional recovery, self-confidence and satisfaction as well as their weight loss maintenance, those procedures are still associated with a high rate of postoperative complications [5]. Obesity (Body Mass Index (BMI) >30 kg/m2) in particular is well known as a significant risk factor for postoperative wound-related complications with seroma, skin dehiscence, infection and hematoma [6–8].
Multiple surgical techniques as well as improvements in the postoperative management have been used with the aim to decrease the rate of wound complications [9]. One of those strategies includes the use of closed incision negative pressure wound therapy (ciNPT) dressings. Negative pressure wound therapy (NPWT) is known to improve oxygen saturation, perfusion and lower the rate of postoperative infections and wound dehiscence, which might indicate a more effective wound healing [10–12]. A similar observation including a significant reduction of exudate and hence an abbreviation of hospitalization has been made in studies about the application of ciNPT on postbariatric wounds [13, 14]. Still there is just few literature about the use in this high-risk patient population [15]. Physiological data undermining a visual alteration of the skin perfusion under ciNPT in clinical patients are lacking. Therefore, the aim of this study was to further examine a possible influence of ciNPT on skin perfusion patterns in postbariatric patients after massive weight loss.
Patients and methods
A prospective study was performed, including 17 patients who underwent an inverted T abdominoplasty between November 2016 and November 2017 in the Department of Plastic and Hand Surgery, University Hospital Erlangen, Germany. Exclusion criteria were Iodine-allergy, patient’s disagreement, loss of patients during the measuring period as well as pre-existing skin lesions as eczema or specific allergies. The protocol was approved by the institutional Review Board (registration number 4207). All patients provided written informed consent. The study adhered to the ethical principles of the Declaration of Helsinki and the International Conference on Harmonization Good Clinical Practice guideline.
Those 17 patients were randomly allocated to either the study or the control group. All surgeries were performed by two plastic surgeons, both with the same level of knowledge and operation technique. The wounds were closed by subcuticular and intracutaneous sutures and three drains were used in each case. Patients from the control group received a conventional wound dressing including Steri-Strip dressing and dry gauze. In the study group a closed incision negative pressure therapy dressing (ciNPT; PREVENA Incision Management System, KCI Medizinprodukte GmBH, an Acelity Company, Wiesbaden, Germany, Fig. 1) was applied. The ciNPT was left on the wound for 5 days with a continuous negative pressure of – 125 mmHg and was only removed twice for measurements one hour (t3) and three days postoperatively (t4). A compressing garment was recommended for 10 weeks postoperatively in both groups.
Application of the closed incision negative pressure therapy (ciNPT) dressing.
During the operation two measurements were performed: t1 = before surgery and t2 = after wound closure. Postoperatively the measurements were repeated at one hour (t3) and three days after surgery (t4). All measurements (t1 – t4) were performed with both a combined laser Doppler spectrophotometry (O2C - Oxygen to See, LEA Medizintechnik, Giessen, Germany) to examine post-capillary oxygen saturation (sO2) and relative hemoglobin content (rHb) as well as with a laser-assisted Indocyanine Green (ICG) angiography (SPY, Novadaq Technologies Inc, Mississauga, Ontario, Canada) to visualize the perfusion pattern [16, 17]. The O2C-device is a reliable und valid method for noninvasive measurement of the parameters mentioned before, which has been verified in a variety of studies with different indications [18–20]. In our study 4 points of measurement were defined that are located at the lateral (M1 and M4) and the medial (M2 and M3) edges of the resection region and were not modified during all measurements pre- and postoperatively (Fig. 2). For the O2C-examination all measured data were averaged and t1 was set as baseline value. T2 is the measurement at the end of the operation and before the application of the different wound dressings and t4 describes the difference of the conventional versus the ciNPT three days after they have been applied. Likewise, the ICG angiography is well known in clinical routine as a reliable tool to visualize perfusion in a real-time surface angiographic imaging system [21–26]. For our purposes 5 ml (2.5 mg/ml) Verdye (Indocyanine Green, Diagnostic Green GmbH, Aschheim-Dornach, Germany) were applied through a peripheral venous line and followed by 20 ml sodium chloride for each measurement. All videos were pseudonymized by an independent third party and the perfusion patterns along the resection line were assessed subjectively by the two surgeons. Therefore, the measurement at the end of the operation (t2) was set as baseline and the alterations at t3 = one hour postoperatively and t4 = three days postoperatively were assessed regarding the distribution of the contrast agent (+1 = faster, 0 = unaltered, – 1 = slower), the intensity of the fluorescence (+1 = higher, 0 = unaltered, – 1 = lower) as an indicator for dye uptake, and the homogeneity (+1 = consistent, 0 = unaltered, – 1 = inconsistent).

Measurement points for the combined laser Doppler spectrophotometry with an example picture of the ICG angiography measurement. Black dots M1’– M4’: preoperative measurement points. Gray dots M1– M4: measurement points after resection.
Statistical analysis was done using GraphPad Prism 7 Version 7.0 d (GraphPad Software, Inc. La Jolla, USA) and Microsoft Excel 2010 (Microsoft Corporation, Redmond, Washington, USA). Data were standardized by setting the first measurement of each measurement point as baseline (t1 = 1) and calculating a ratio for t3/baseline and t4/baseline (O2C), respectively setting t2 as baseline and assessing the alteration at t3 and t4 (SPY). A P value <0.05 was considered significant.
General patient characteristics
A total of 17 patients, who underwent an inverted T abdominoplasty between November 2016 and November 2017 were included in the study. 11 patients were randomly allocated to the study group and 6 patients to the control group. Patients’ characteristics are summarized in (Table 1). Of those patients, there were 4 males and 13 females. The mean age in general was 41 years (30–55 years), while the mean age in the study group was 38.1 years and 46.3 years in the control group. The mean BMI before weight loss amounted to 50.9±9.6 kg/m2 with a minimal BMI of 36.7 kg/m2, a maximum of 67.2 kg/m2 and a mean weight of 152.8±35.5 kg (94–217 kg). At the time of the postbariatric plastic surgery the mean BMI was 28.5±3.7 kg/m2 (21–33.4 kg/m2) and the mean weight was 85.7±17.1 kg (55–107 kg), with no significant difference between the groups, neither before nor after weight loss. The weight loss averaged 67.1±24.8 kg with a range from 30 kg to 110 kg of lost weight. There was no significant difference between the study (68.2±22.3 kg, range 30–100 kg) and control group (65.2±31.1kg, range 35–110 kg), nor between those patients who underwent bariatric surgery before (10 patients; 71.7±9.8 kg, range 35–110 kg) and those, who lost weight through lifestyle changes (7 patients; 60.6±23.9 kg, range 30–100 kg). In each group a mean relative weight loss of 43% (28–59%) of the initial weight has been calculated. In average 2500±1430 g tissue was resected, with a range from 900 g to 5650 g and no significant difference between the groups. Concerning risk factors and comorbidities there was one patient with diabetes mellitus Type II and 6 patients were smokers. Further risk factors were not considered.
General patient characteristics of both groups (n = 17)
General patient characteristics of both groups (n = 17)
The measured relative oxygen saturation (sO2) at the different time points varies in the study (ciNPT) and the control group (control), as can be seen in (Fig. 3a). Unpaired t-test shows that there is no significant difference between the groups during the intraoperative measurements (t1 and t2). Three days after the application of the different wound dressings (t4) the oxygen saturation is significantly higher in the study group than in the control group (*p = 0.0187). Despite the random allocation of the patients to the two groups, there is a discrepancy of the sO2 between study and control group at time point t2, which is due to the fact that the sO2 varies interindividually.
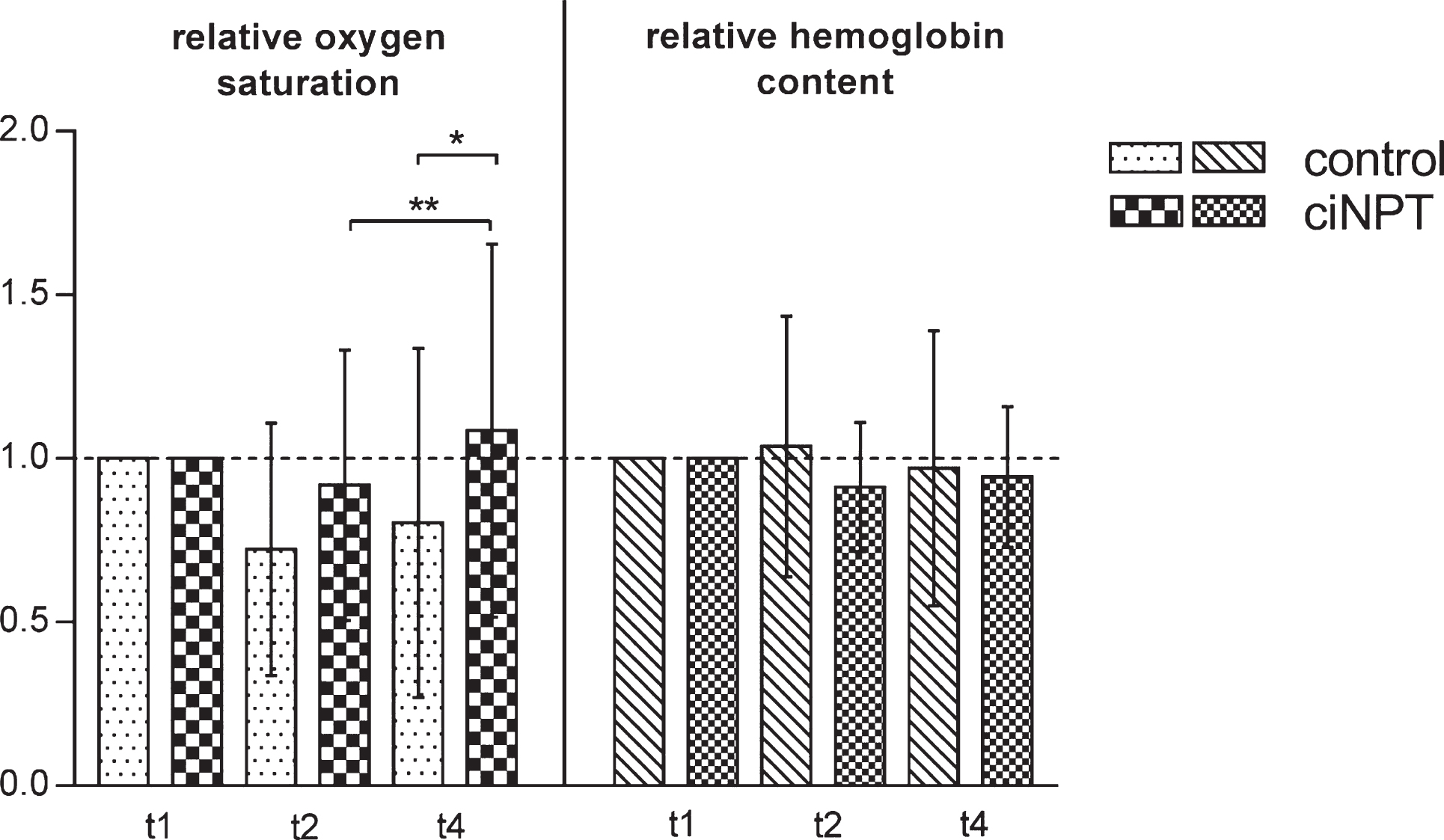
Examination of the combined laser Doppler spectrophotometry measurements. Left: Relative oxygen saturation at the different measuring time points comparing study (ciNPT) and control group (control) with t1 set as baseline. Control: 1 outlier removed. CiNPT: 3 outliers removed. *p = 0.0187 (unpaired t-test) **p = 0.0088 (paired t-test). Right: Relative hemoglobin content at the different measuring time points comparing study (ciNPT) and control group (control) with t1 set as baseline. Control: 0 outliers removed. CiNPT: 4 outliers removed.
The alteration of the measured relative oxygen saturation over the course of time comparing study and control group shows a less strong initial decrease and a faster increase in the study group. As can be seen in Figs. 3 and 4 the oxygen saturation decreases from the baseline and is still inferior to the initial value three days postoperatively in both groups. Despite no statistical significance, there is a trend that the oxygen saturation is increasing faster again in the study group, as can be seen in t2 ⟶ t4. To validate this observation a paired t-test was performed comparing the relative oxygen saturation at t2 and t4 in each group. In the study group there was a significant difference (**p = 0.0088), while no statistical significance could be seen in the control group (Fig. 3, left side).
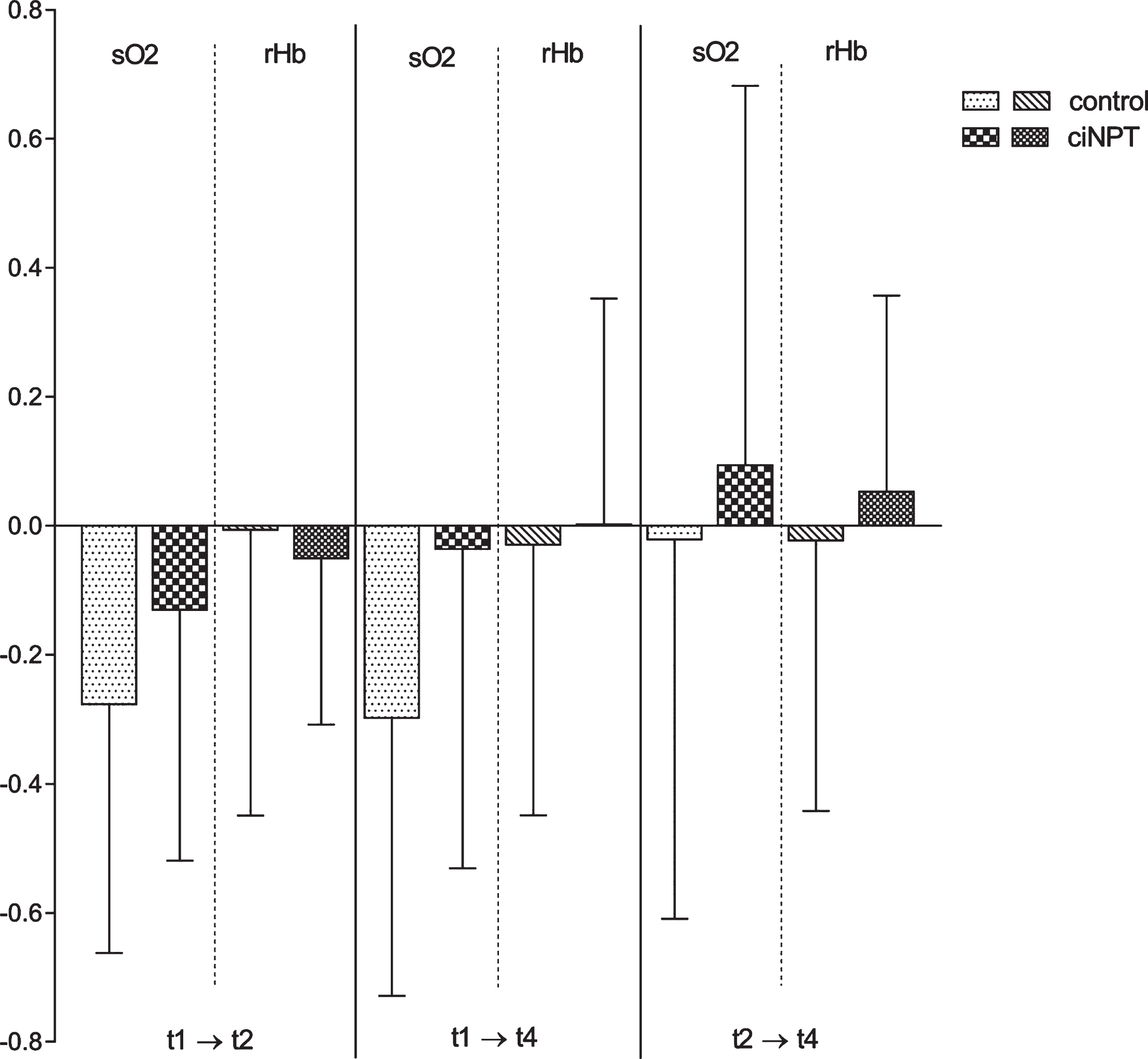
Examination of the combined laser Doppler spectrophotometry measurements. Alteration of the measured oxygen saturation (sO2) and the relative hemoglobin content (rHb) over the course of time: from the baseline value (t1) to the measurement at the end of the operation but before the application of the wound dressing (t2); from t1 to the last measurement three days postoperatively (t4) and from t2 to t4 comparing study (ciNPT) and control group (control).
The evaluation of the measured values for the relative hemoglobin content did not reveal any significant differences between the groups, nor within a group (Fig. 3, right side). Figure 4 shows the alteration of the relative oxygen saturation (sO2) and the relative hemoglobin content (rHb) in the course of time comparing the two groups suggesting a correlation between sO2 and rHb, as they trend to alter aligned at all measurement dates. For the study group a strong correlation between sO2 and rHb was calculated at t4 (r = 0.487), but only a moderate correlation for the control group at t2 (r = 0.291) and a weak correlation for the study group at t2 and the control group at t4 (data not shown).
Improved perfusion patterns in the ICG angiography in the study group
The statistical evaluation of the ICG angiography-measurements is shown in Fig. 5. At t3 = one hour postoperatively there is nearly no change in the control group, while the distribution of the contrast agent is faster, the intensity of the fluorescence is higher, and the homogeneity is more consistent in the study group compared with the baseline at t2 (Fig. 5a). Three days postoperatively this development is affirmed in the study group but there is also an enhancement of the parameters in the control group, although to a lesser extent (Fig. 5b). The strongest improvement in both groups was seen for the intensity of the fluorescence three days postoperatively with a significant difference between the groups (p = 0.016). There is no statistical significance between the study and the control group concerning the distribution of the contrast agent and the homogeneity, but the alteration to a faster distribution and a more consistent homogeneity is more distinct in the study group.
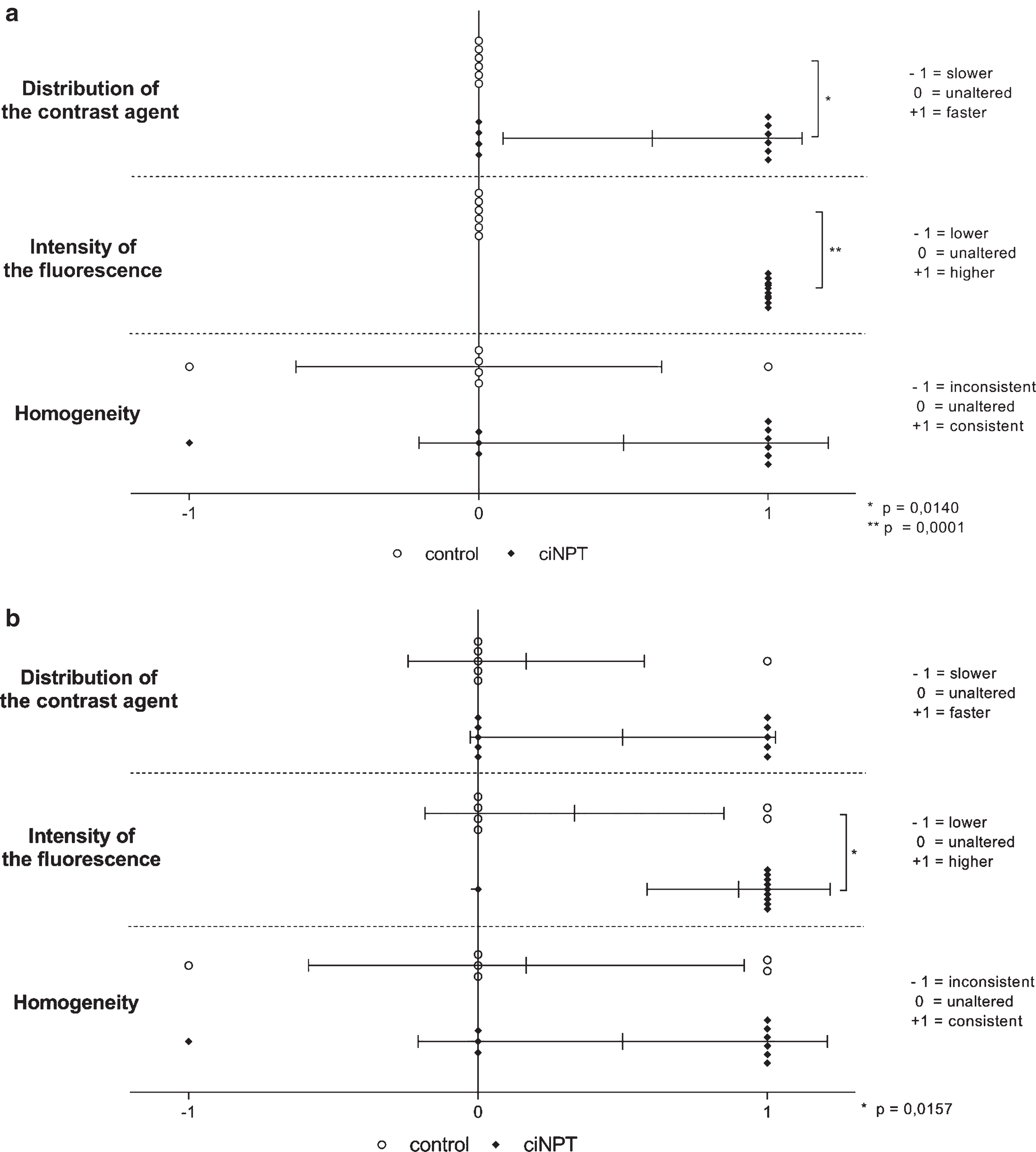
Examination of the ICG angiography measurements. Alteration of the distribution of the contrast agent, intensity of the fluorescence and homogeneity
Abdominoplasty is one of the most commonly performed plastic surgeries and its popularity is still increasing steadily. This is due to the fact that it is the most effective method to reduce excessive skin and consequently to restore the body contour in patients who have lost a great amount of their body weight (Fig. 6). Despite the frequency of abdominoplasties, those procedures still have a high rate of postoperative complications with rates varying from 30% to 70% in the literature [5, 27]. Hence, there are multiple studies assessing risk factors with the aim of lowering the complication rates. Two of the most frequently described risk factors for postoperative complications, such as seroma, skin dehiscence, hematoma or wound infections, are frequently a high pre-operative BMI (>30 kg/m2) and smoking [28, 29]. Therefore patients, seeking body contouring surgery according to literature should be recommended to quit smoking at least 4 weeks pre- and 4 weeks postoperatively as well as to keep a stable weight since at least 6 months.
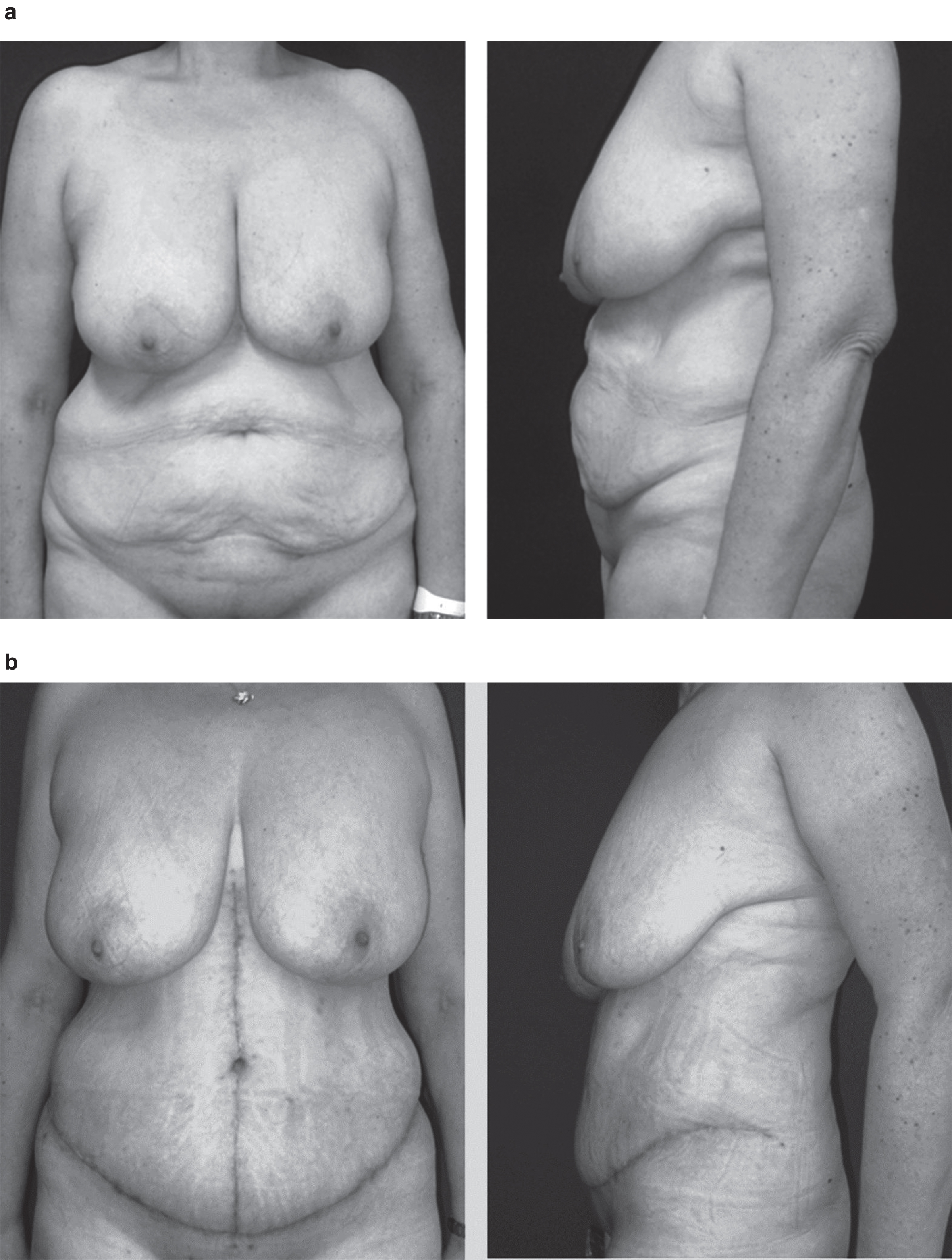
Example of a 53 year old patient from the control group with an initial weight of 112 kg and a weight loss of 35 kg through gastric bypass (2014), resection weight: 900 g. a Preoperative examination. b Five weeks after abdominoplasty.
There is also extensive literature about operative techniques and postoperative management to improve the complication rate in body contouring procedures [30]. Araco et al. state that raising the abdominoplasty flap with a diathermocoagulation instead of with a cold knife reduces the development of postoperative hematomas and wound infections with delayed healing [31]. According to Bercial et al. quilting sutures and suction drains are effective methods to prevent seroma formation, while Pollock et al. describe positive effects of progressive tension sutures on postoperative local complications [32, 33]. In 2013, Conde-Green et al. described the application of a negative pressure wound device on the closed incision after ventral hernia repair and reported of a decreased rate of wound complications compared with conventional dressings. Likewise, Dragu et al. as well as Horch et al. related of the use of ciNPT in high-risk wounds, specifically in postbariatric patients and observed an abbreviated length of hospitalization due to a decreased exudate formation which enables earlier drain removal [13, 14].
Validated effects of NPWT on wounds and wound environment
Aside from the utilization of NPWT on closed wounds (ciNPT), negative pressure wound therapy for the management of a wide variety of complex acute and chronic wounds is a revolutionary and well-established method since the 1990s. Consequently, there are numerous studies investigating the mechanisms of action of the vacuum-assisted closure on physiological, microbiological and clinical levels.
On the one hand the application of sub-atmospheric pressure to airtight dressed wounds supports the drainage of excess fluid and debris, which helps to reduce wound edema and bacterial count colony that is essential for a curative wound environment [34]. Especially a high continuous negative pressure leads to an effective fluid removal and despite some reports on the occurrence of pain and ischemia in the bandaged area, a continuous pressure of – 125 mmHg for five days was used in our study [35]. No cases of patients complaining about pain or ischemia were observed. On the contrary, patients claimed to feel safe and comfortable with the NPWT and therefore felt less anxious to get out of bed early and move cautiously after the operation.
On the other hand, the suction force created by the NPWT equipment increases blood flow perfusion (measured with a laser Doppler blood perfusion imager) in the wound environment and also promotes micro- and macrodeformation on the wound surface [36]. Xia et al. described the positive effect of the NPWT on blood flow perfusion by using a laser Doppler blood perfusion imager and thus an increased expression of angiogenesis associated growth factors [37].
Observed effects of ciNPT on oxygen saturation, relative hemoglobin content and perfusion patterns in our study
The aim of this study was to analyze and objectify the influence of a closed incision negative pressure therapy dressing (ciNPT) on tissue perfusion parameters such as sO2, rHb and perfusion pattern in postbariatric patients. To the best of our knowledge this is the first randomized controlled and prospective study that investigates the short-term effects of ciNPT on above mentioned parameters in this specific patient population.
Adequate blood flow perfusion and subsequently a sufficient oxygen supply in the tissue are essential for a satisfactory wound healing. We observed a decrease of the oxygen saturation during the operation (t1 ⟶ t2) (Figs. 3, left side, and 4) which is presumably due to the vascular anatomy of the abdominal wall, considering the caudal transversal resection line that disrupts the course of the inferior epi-gastric artery [38]. Dragu et al. examined the intra-operative abdominal wall perfusion in postbariatric abdominal dermolipectomy and found that oxygen saturation, relative hemoglobin content and blood flow increase during abdominoplasty specifically along the caudal wound margin, but decrease in the cranial median line, which correlates with our findings [12]. We hypothesized that those patients, receiving the ciNPT will have enhanced perfusion as well as increased oxygen saturation as indicators for an improved wound healing.
The analysis of the results supports the assumption of an increase of oxygen saturation after the application of the ciNPT on the wound (Figs. 3 and 4). SO2 is significantly higher in the study group compared to the control group three days postoperatively, likewise there is a highly significant alteration in the study group from t2 to t4. This finding correlates with the observations from the ICG angiography-measurements. As can be seen in (Fig. 5a) there is a significantly faster distribution of the contrast agent, a significantly higher intensity of the fluorescence and a more consistent homogeneity in the study group than in the control group, comparing one hour postoperatively (t3) to the measurement at the end of the operation (t2). This might indicate an improved perfusion due to the ciNPT, which is affirmed through the follow-up measurement three days postoperatively (Fig. 5b). Due to the fact that this was the first study using the ICG angiography in this context, there is no literature to compare those findings. Although not reaching statistical significance in all cases, it can be assumed that a closed incision negative pressure therapy dressing has a positive effect on perfusion and oxygen saturation in postbariatric patients, thus having a possible positive influence on complications and/or the cosmetic result. The aim of this study was to examine the short-term effects of ciNPT on sO2, rHb and perfusion pattern. To assess the influence of those parameters on postoperative wound complications like wound dehiscence, infections, seroma, hematoma or scar quality, larger sample sizes and a long-term observation period are required.
Conclusion
Abdominoplasty is one of the most frequently performed plastic surgical procedures but is still associated with a significant rate of postoperative complications, especially in postbariatric and obese patients. Those patients would particularly benefit from a wound dressing that supports the wound healing procedure and avoids wound healing complications. CiNPT is an easy and fast method that not only prevents patients from painful dressing changes in the early postoperative period, but also has a measurable influence on perfusion patterns in the wound environment. The present study provides evidence that a ciNPT device improves local skin perfusion and oxygen saturation in postbariatric patients, which are fundamental conditions for an uneventful wound healing.
Disclosures
This is an investor-initiated study. KCI Medizinprodukte GmBH, an Acelity Company (Wiesbaden, Germany) donated all ciNPT devices but did not make any other payment or grant to the institution and did not have any influence in study design, data collection, statistical analysis or writing the final manuscript. The study was not influenced by any other party than the authors themselves.
One author received once-only an honorary for a lecture by Novadaq but has no conflict of interest concerning this study.
Another author has received grants for scientific studies from KCI-Acelity, Wiesbaden, Germany and Baxter AG Vienna, and has acted as a lecturer and as an advisor for KCI-Acelity Wiesbaden and San Antonio, and has acted as an invited speaker for Novadaq, Germany.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in this study.
Footnotes
Acknowledgments
This work was performed in fulfillment of the requirements for obtaining the degree Dr. med.