
Abstract
The objective of this research was to investigate the clinical value of contrast-enhanced ultrasound (CEUS) for prediction of cervical lymph node metastasis (CLNM) in papillary thyroid cancer (PTC).
One hundred and eighty-six patients with PTC confirmed by fine needle aspiration (FNA) were preoperatively performed CEUS.A multivariate analysis was performed to predict CLNM by 15 independent variables. Receiver operating characteristic (ROC) curve analysis was used to evaluate the diagnostic performance.
There were totally 37 patients with CLNM confirmed by pathology. Multivariate analysis demonstrated that intensity at peak time, capsule contact and size on CEUS were the three strongest independent predictors for CLNM. ROC analyses of these characteristics showed the areas under the curve (Az), sensitivity, and specificity were 0.650, 48.6 %, 79.8 %; 0.586, 67.6%, 49.7%; and 0.612, 56.8%, 64.4% for intensity at peak time, capsule contact, and size, respectively.
The CEUS patterns of PTC are relative to not only the size of PTC but also the possibility of CLNM after thyroidectomy. CEUS seem to be a tool to predict CLNM in PTC patients.
Keywords
Introduction
Papillary thyroid cancer (PTC) is the most common endocrine cancer of the thyroid. During the past few decades, its incidence has increased in Shanghai by more than 432% from 1997 [1] to 2009 [2]. Most PTC have excellent prognosis. However, 30–40% of patients also experience cervical lymph node metastasis (CLNM) [3]. CLNM increases the risk of recurrence of PTC, and it has been found to be associated with PTC-related death [4]. For these reasons, assessment of the CLNM state is important for the treatment planning and prognostic evaluation of PTC patients [5].
The new American Thyroid Association guidelines recommend ultrasound as the first imaging method used for the assessment of CLNM in patients with PTC [6]. However, cases of microscopic CLNM with false-negative ultrasound characteristics have been reported: A recent meta-analysis [7] showed the sensitivity of ultrasound to be 63% (95% CI, 47–76%), the specificity to be 93% (95% CI, 73–99%), and the area under the curve to be 0.81 by level-by-level analysis. This suggests that we need a novel ultrasound (US) technique to predict CLNM, especially for cases not detectable by conventional US in patients with PTC.
Contrast-enhanced ultrasound (CEUS) can clearly display microvessel blood flow in tumors, and it can accurately evaluate the sequence and intensity of tumor perfusion and vascularity [8–11]. Several studies have reported that CEUS had a good performance in differentiating malignant from benign thyroid nodules [12–14]. To our knowledge, there have been few reports on the ability of CEUS to predict CLNM in patients with PTC. For this reason, the aim of this study was to expand upon these previous investigations to select the best predictors of malignant thyroid nodules based on CEUS.
Materials and methods
Patients
Informed consent was obtained from all patients, and the study design was approved by Ethics Committee of Huadong Hospital, Fudan University (20140144) and performed in accordance with the ethical guidelines of the Helsinki Declaration. From November 2014 to May 2017, 186 patients with 186 thyroid cancers (42 men and 144 women) were involved in the study. The mean age of the examined patients was 49.0±14.1 years (age range, 17–84 years). The median size of the nodules was 1.0×0.8×0.9 cm (range, 0.6×0.5×0.5 cm to 2.8×2.0×2.5 cm).
A flowchart showing the patient selection is given in Fig. 1. The inclusion criteria for the patients were as follows: (1) The patients with nodules underwent fine needle aspiration (FNA), and the cytology analysis revealed TBSRTC (the Bethesda System for Reporting Thyroid Cytopathology) level V or VI; (2) Patients were confirmed to have only one nodule of PTC by histopathological examination; (3) There were no abnormal cervical lymph nodes (ACLN) detected by conventional US before operation; (4) Patients underwent a total thyroidectomy combined with central neck dissection (CND). Lateral neck dissection (LND) was recommended during thyroidectomybased on clinical conditions in patients diagnosed with cervical LNM other imaging studies. The extent of thyroid surgery was determined mainly in accordance with the guidelines of the American Thyroid Association (6); (5) Nodule size greater than 0.5 cm (nodules smaller than 0.5 cm are difficult to image with CEUS examination because of breathing and arterial pulsations). The exclusion criteria were as follows: (1) PTC with coarse calcifications. (2) Nodules were confirmed benign by histopathological examination. (3) Patients with more than one nodule confirmed to be PTC. (4) Pregnancy.
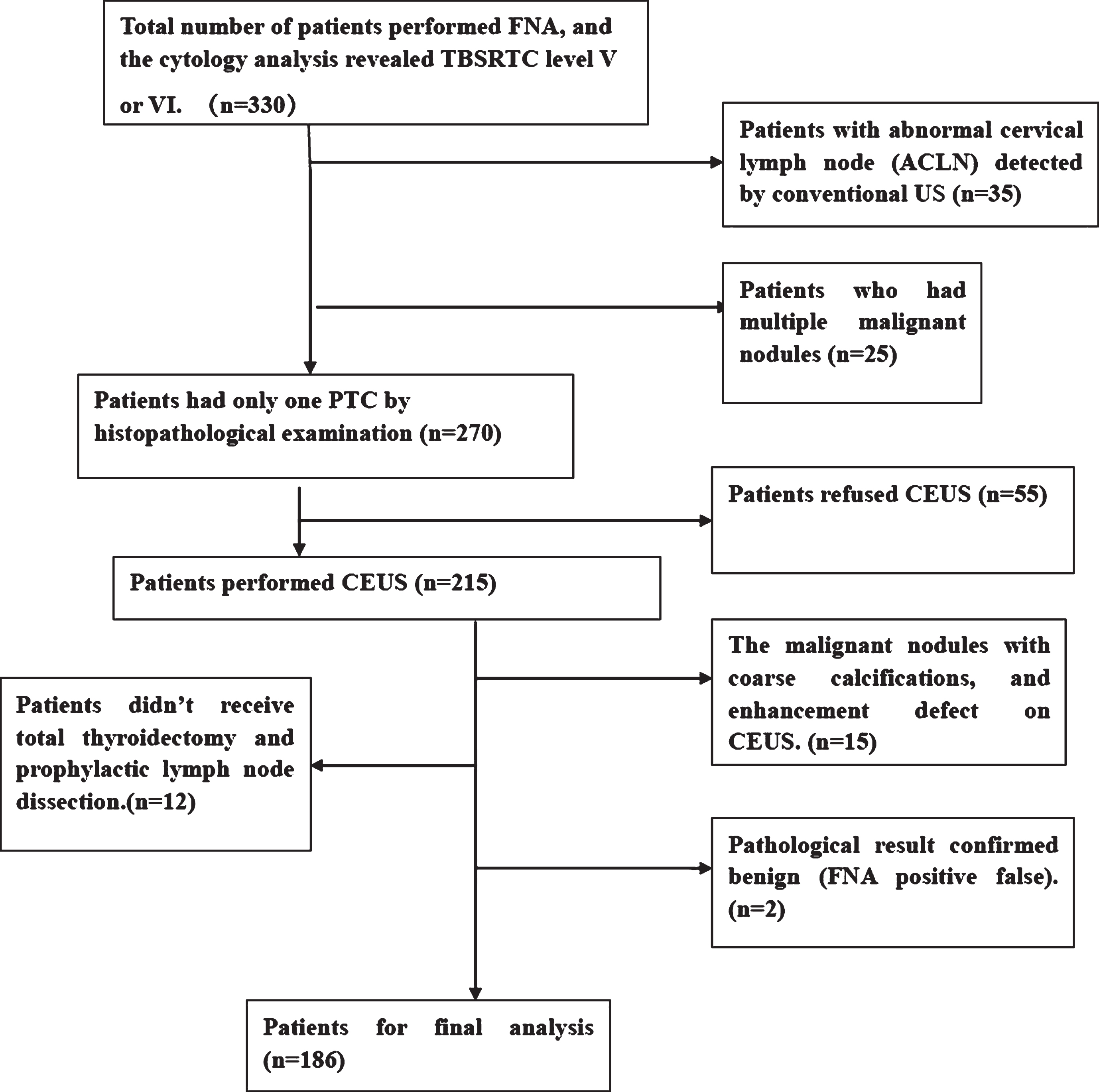
Flowchart showing patient selection.
All conventional ultrasound were performed with a 9 MHz transducer (Acuson S2000 or S3000, Siemens, Germany). The ultrasound examination was performed by ten years experienced operators. Thyroid cancers were evaluated for: size (largest diameter, subgrouped as small nodule group: >5 mm and < 10 mm; middle nodule group: 10–20 mm; and big nodule group: >20 mm), shape (regular or irregular), margin (well or poorly defined), internal nodule components (solid, or mixed), presence or absence of halo sign, capsule shape taller than it is wide, presence or absence of capsule contact, echogenicity (hypoechogenicity), calcifications (microcalcification or not),abnormal cervical lymph node (ACLN) (presence or absence). Lymph node showing at least one following suspicious feature was defined as ACLN: taller than width shape, absence of fatty hilum, presence of calcification or cystic change, and peripheral vascularization [5].
Moreover, the color Doppler flow patterns were classified as four types [15]: (type I, absence of blood flow; type II, mainly periphery and absent interior blood flow; type III, mainly interior and absent periphery blood flow; type IV, both periphery and interior blood flow),perforating branches (presence or absence), resistance index (RI) (≥0.75 or < 0.75).
Contrast-enhanced ultrasound (CEUS) examination
All CEUS imaging of thyroid nodules was performed by two seasoned clinical ultrasound examiners (J.Z. and X-H.D.), with more than 5 years of experience in ultrasound thyroid examination. After the conventional ultrasonography examination, the largest view of the nodule was chosen before the CEUS mode was switched. The focus zone was always placed at the bottom level of the nodule, and CEUS was performed using low mechanical index (MI < 0.10). Contrast agents (SonoVue, Bracco International, Milan, Italy) was injected intravenously as a bolus at a 2.0 mL dose, followed by a 5 mL saline flush. The timer on the US machine were started during the CEUS process, and the images lasted at least 2 min were digitally stored as raw data.
The thyroid nodules on CEUS were evaluated relative to a normal thyroid parenchyma. The time of appearance and disappearance of microbubbles was classified as early, middle, or late; peak intensity was classified as hyper-, iso-, or hypo-enhancement; homogeneity of enhancement was classified as homogeneous or heterogeneous and relative washout time classified as early or not early.
Rescan of conventional ultrasound for cervical lymph nodes metastasis (CLNM)
According to CEUS, patients with the thyroid cancer with iso-enhancement or hypo-enhancement were considered at high risk for CLNM, so a clinical ultrasound physician rescanned the anatomical neck level I to VI to search ACLN.
Statistical analysis
Patients were divided into groups according to the size, the pattern of enhancement, and presence or absence of CLNM. Continuous quantitative data are here expressed as the mean±standard deviation (SD). The χ2 test was used to compare the categorical variables of clinical characteristics. The Cochran-Mantel-Haensel (CMH) χ2 tests were used in the analysis of stratified or matched categorical data. A multivariate logistic regression analysis was performed to determine the independent factors associated with CLNM. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated and receiver operating characteristic (ROC) curves were analyzed for factors with significance on multivariate logistic regression analysis.
All statistical tests were performed using commercially available software (Stata, version 10.0; Stata Corp, College Station, TX, US). For all tests, a P-value < 0.05 was considered indicative of statistical significance.
Results
Histological results
All 186 patients were diagnosed as PTCs by histopathological examination, and everyone had only one carcinoma. Fifty-eight CLNM were found in 37 patients (19.9 %), among whom 30 (16.1 %) had central LNM and 7 (3.8 %) had lateral LNM.
Valuable indicators of US, color Doppler flow imaging, and CEUS
Basic characteristics of the patients and conventional ultrasound features of PTCs are shown in Table 1. Mean age, size, taller than wide, and capsule contact were significantly different between the CLNM group and without CLNM group (P < 0.05). Gender, multiple nodules, shape, margins, internal components, halo sign, echogenicity, and calcification in patients did not show significant differences between the two groups (all P > 0.05). With regard to the color Doppler flow imaging (CDFI) patterns and CEUS features, CDFI patterns and intensity at peak time were significantly associated with CLNM, whereas resistance index (RI), perforating branches, earlier arrival time, homogeneity and earlier washout time were not statistically (Table 2).
Basic characteristics of the patients and conventional ultrasound features of papillary thyroid carcinoma
Basic characteristics of the patients and conventional ultrasound features of papillary thyroid carcinoma
CDFI and CEUS indicators of PTCs
CDFI, color Doppler flow imagine; CEUS, contrast-enhanced ultrasound; PTC, papillary thyroid carcinoma; RI, resistance index. *RI can be detected in total 76 PTCs.
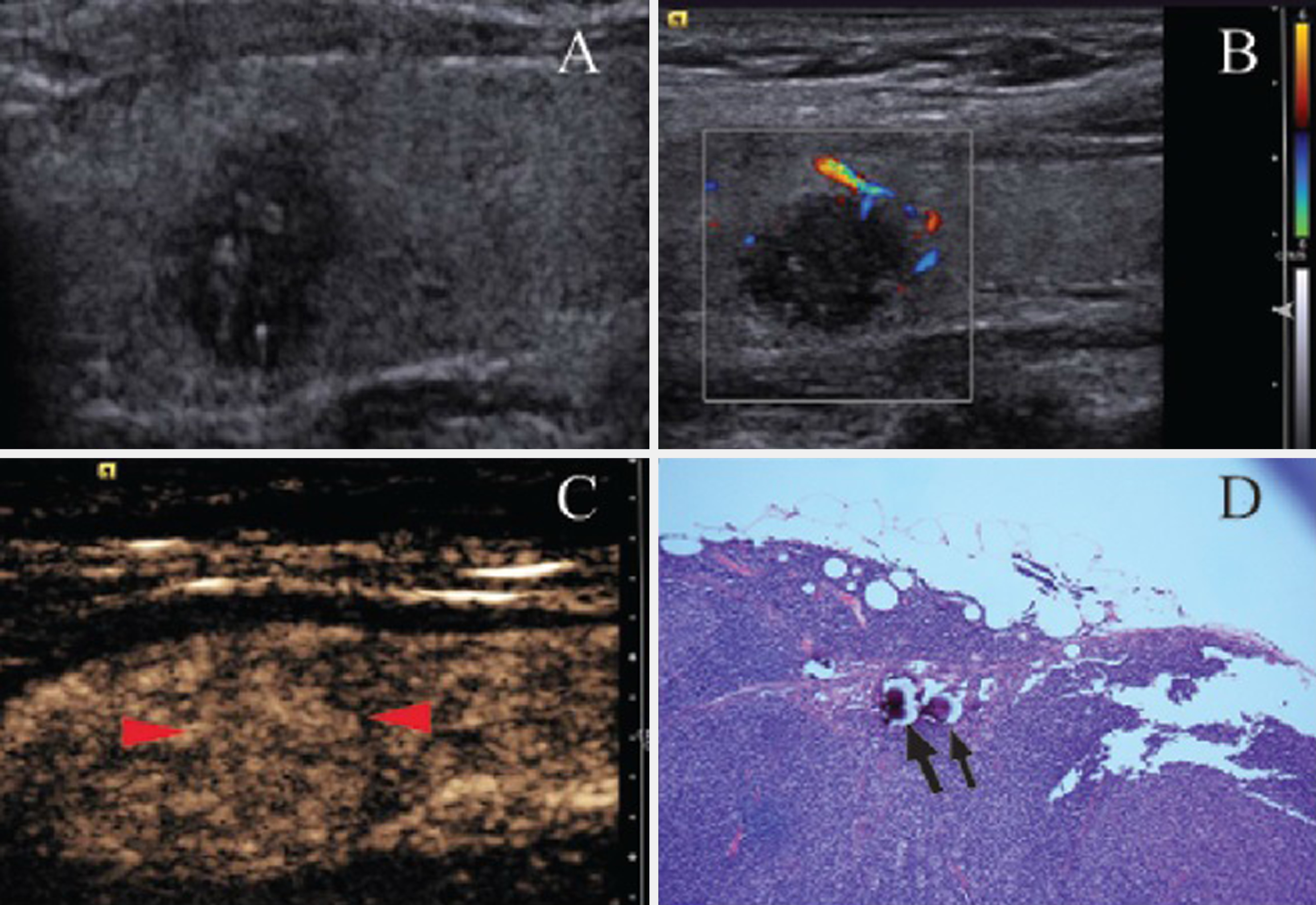
After CEUS was performed, total 14 PTC were identified as hypo-enhancement and 34 showed iso-enhancement. For this reason, we rescanned 48 patients for cervical lymph node metastasis by conventional ultrasound. As a result, new cases of ACLNM not diagnosed after the first scan were found in two patients, and these diagnoses were confirmed by histopathological examination (Fig. 2).

A 27-year-old woman (A) With a hypoechoic, poorly defined margin, microcalcification thyroid nodule in right lobe (17×13 mm) and negative findings for ACLN by US. FNA revealed TBSRTC level VI. (B) Both periphery and interior blood flow in CDFI (type IV). (C) Heterogeneous, hyper-enhancement on CEUS (16 s after Sono Vue injection) which indicate high risk for CLNM. (D) The neck was rescanned from level I to VI using US, and new ACLN was observed on ipsilateral upper neck (8×6 mm), and histopathologic examination confirmed cervical lymph node metastasis.
Multivariate logistic regression analysis showed that intensity at peak time, capsule contact, and nodule size were the three strongest independent predictors of CLNM, followed by calcification, earlier washout time, and echogenicity (OR > 1);whereas homogeneity, shape, multiple nodules, CDFI patterns, perforation of the branches, margin, earlier arrival time, capsule being taller than wide, and internal components were not significantly associated with CLNM (OR < 1) (Table 3).
Multivariate logistic regression analysis in predicting CLNM
Multivariate logistic regression analysis in predicting CLNM
The overall diagnostic performance of intensity at peak time (Az:0.650; 95% CIs: 0.559–0.740) was better than other predictors such as size (Az: 0.612; 95% CIs: 0.518–0.705), capsule contact (Az: 0.586; 95 % CIs: 0.500–0.673), calcification (Az: 0.563; 95% CIs: 0.475–0.650), earlier washout time (Az: 0.536; 95% CIs:0.452–0.620), homogeneity (Az: 0.530; 95% CIs:0.484–0.576) echogenicity (Az: 0.516; 95% CIs: 0.453–0.580), shape (Az: 0.488; 95% CIs: 0.397–0.579), multiple nodules (Az: 0.486; 95% CIs: 0.412–0.560),internal components (Az: 0.483; 95% CIs: 0.444–0.522), perforating branches (Az: 0.477; 95% CIs: 0.401–0.553), margins (Az: 0.464; 95% CIs: 0.375–0.554), earlier arrival time (Az: 0.423; 95% CIs: 0.339–0.508), CDFI patterns (Az: 0.423; 95% CIs: 0.325–0.521), and capsule taller than it is wide (Az: 0.391; 95% CIs: 0.302–0.480) (Table 4).
ROC analyses for the characteristics in prediction of CLNM from patients with PTCs
ROC analyses for the characteristics in prediction of CLNM from patients with PTCs
Ultrasound examination is the preferred first-line modality of imaging in the evaluation of thyroid nodules, allowing detection of signs associated with malignant nature, such as microcalcifications, hypoechogenicity, irregular margins or absent halos, intranodular vascularization greater than the perinodular, and a shape taller than it is wide [16]. However, these characteristics are not suitable for prediction of CLNM (P > 0.05) (Table 1), except for the nodule having a shape taller than it is wide and capsule contact.
Although lymph node involvement of lateral and central levels is very common in PTC [17], these metastases are barely visible under conventional ultrasound, in most cases because some of them are microscopic while others are blocked by the clavicle (Fig. 2). For this reason, new complementary sonographic techniques are needed to improve the predictive and diagnostic evaluation of CLNM.
CEUS techniques can be used to visualize the microvessels of tumor and offer the details of tumor vascularity. This method can be applied to the evaluation of tumor angiogenesis in vivo. Currently, CEUS is regarded as a promising tool for diagnosis of malignant thyroid tumors [19–22].
Angiogenesis plays an important role in the development, growth, and metastases of cancer. PTC can spread to regional lymph nodes through newly formed or preexisting vessels [23], and LNM of thyroidtumors showed increased microvessel expression with respect to the primary tumor [24]. Immunohistochemical analysis showed the microvessel density of PTC to be significantly higher than that of surrounding tissue. Therefore, the PI on CEUS was significantly closely relevant to MVD [25]. In the present study, there was a significant difference in peak intensity between the CLNM group and the group without CLNM (P < 0.05), and peak intensity was the strongest independent predictor of CLNM (Table 2). It was here hypothesized that the peak intensity of CEUS may be relative to CLNM: the more enhancements at peak time, the greater the microvessel density in tumor tissue, and the greater the possibility that CLNM will take place.
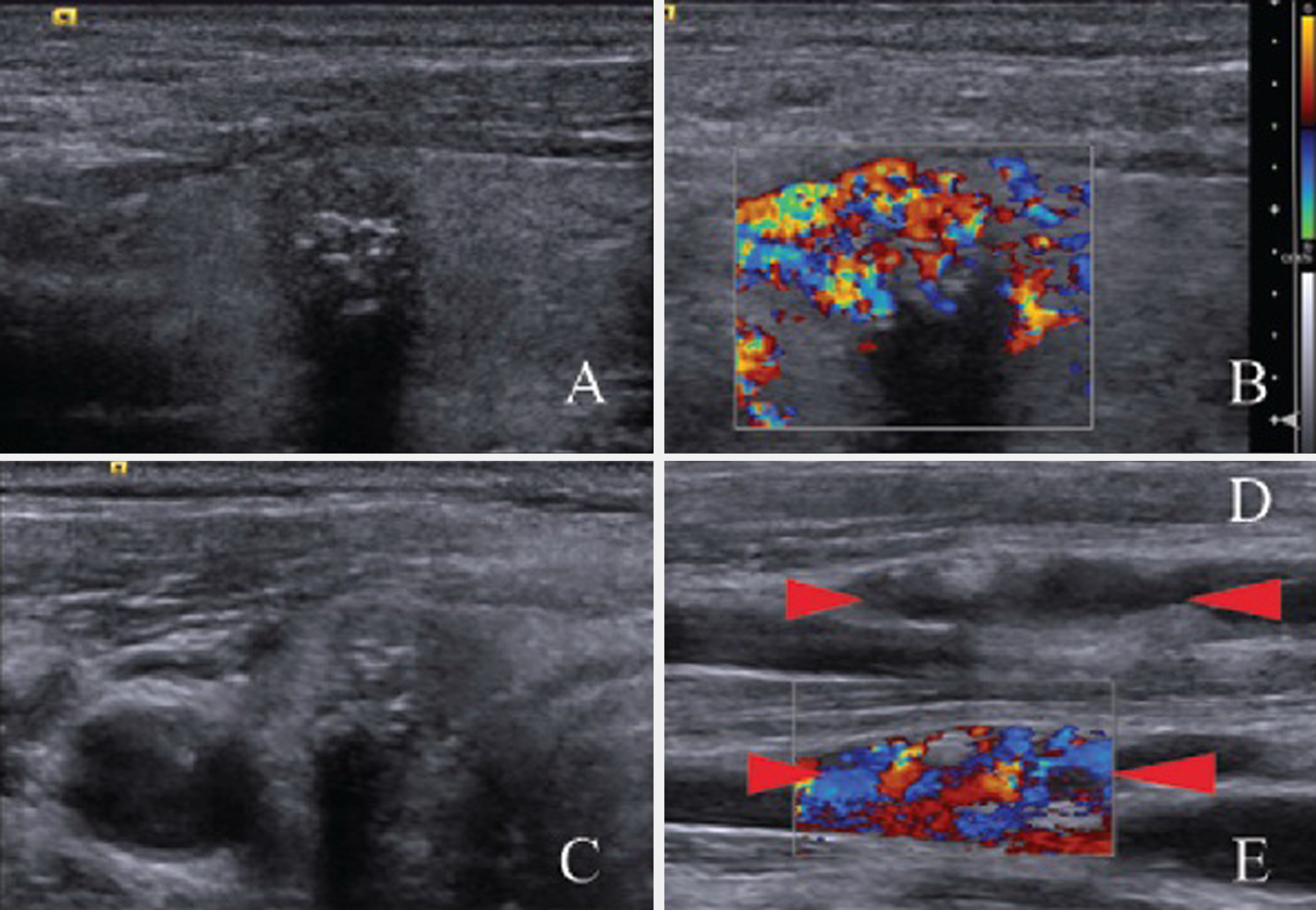
The CEUS patterns of PTC were first reported by Bartolitta, and the enhancement of PTC was concluded to be associated with the size of the tumor: Thyroid nodules that were less than 1 cm in diameter indicated that vascularization was mainly absent; those between 1 and 2 cm showed faint dotted contrast enhancement; and nodules with a diameter larger than 2 cm presented diffuse contrast enhancement [26]. These findings have repeatedly been cited in previous works. However, this theory fails to explain the iso-enhancement or hyper-enhancement of small PTC (Fig. 3).
A 45-year-old woman (A) With a hypoechoic, solid, microcalcification thyroid nodule in right lobe (8×6 mm), FNA revealed TBSRTC level VI. (B) Mainly periphery and absent interior blood flow (type II). (C) Heterogeneous, iso-enhancement on CEUS (15 s after Sono Vue injection) which was supposed to be hypo-enhancement according to Bartolitta’s classical theory. (D) Histopathologic examination shows cervical lymph node metastasis on central level (5×4 mm), thyroid follicular epithelium was found near the microcalcifications in lymph node (arrow).
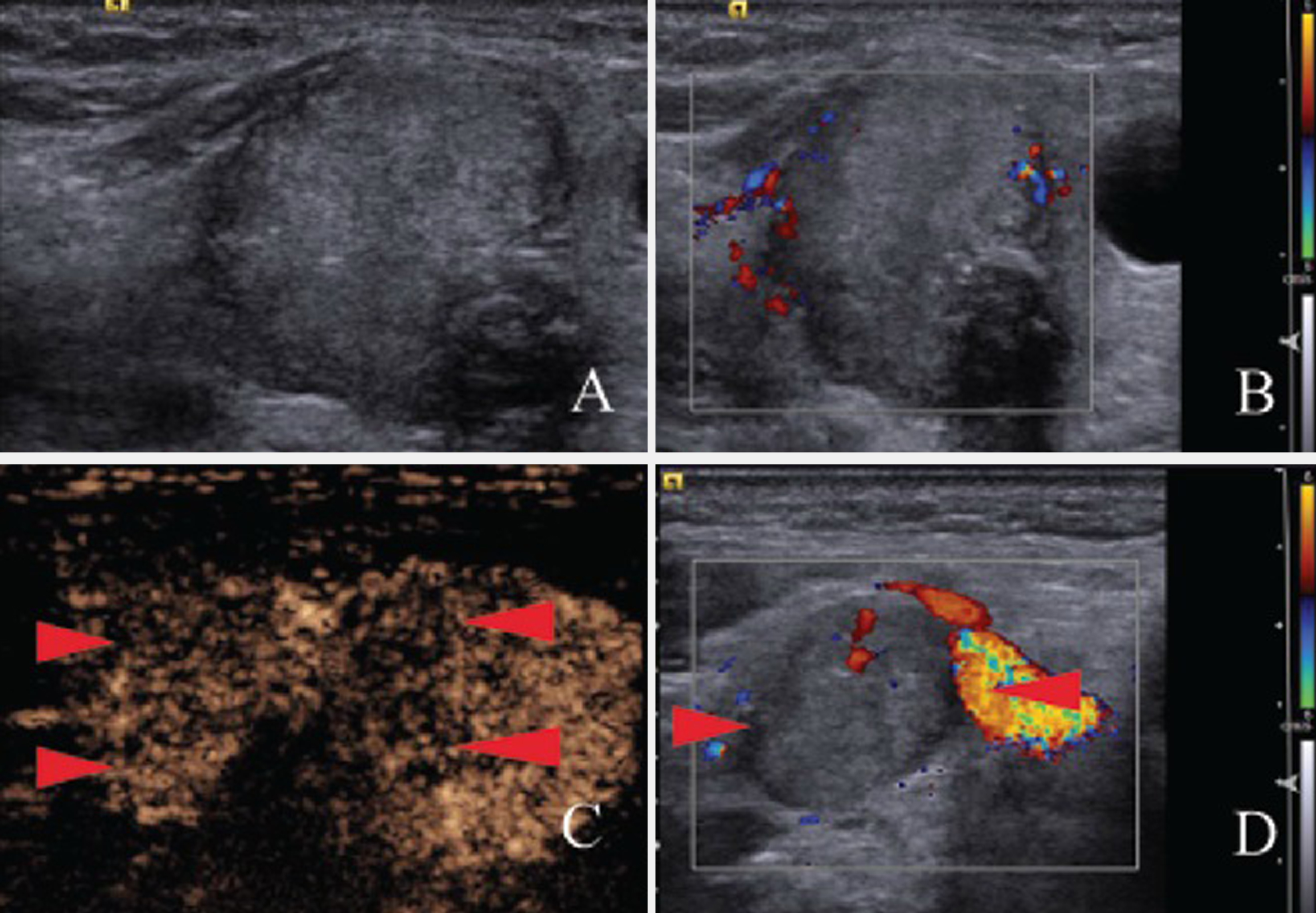
The advantages of this new hypothesis are as follows. First, it explains the different CEUS patterns of PTC, even for nodules of the same size; second, the consensus amongst the world’s physicians is that overdiagnosis of PTC occurs, and they suggest that screening be banned [27]. Against, this background, nodule diagnostic FNA is not recommended at < 1 cm in the novel management guidelines for adult patients with thyroid cancers [6]. However, in clinical practice, some PTC < 1 cm have been observed in CLNM for short periods (Fig. 4).CEUS may be a new screening tool for highly aggressive PTC, while most such cancers proceed more indolent [28]. Third, CEUS was always considered a tool for diagnosing malignant thyroid tumors, but it is significantly less accurate than FNA and lacks clear and unified diagnostic criteria. In the present study, the rate of misdiagnosis was 34.4 (64/186) due to PTC < 1 cm showing hyper- or iso-enhancement (45/64)and PTC > 1 cm showing hypo-enhancement (19/64);only two cases were ruled out because of the false-positive FNA result (Fig. 1). CEUS may be a more suitable tool for prediction of CLNM for PTC patients than differential diagnosis tools. Finally, the new hypothesis seemed consistent with existing classical theory: the larger the PTC, the greater the area of capsule contact, the greater the enhancement on CEUS, and the greater the possibility of CLNM (Fig. 5) (Table 3).
(A) A 66-year-old woman with a solid hypoechoic, microcalcification and nodule taller than it is wide in the right lobe (9×7 mm), high risk for malignant thyroid nodule. (B) Both periphery and interior blood flow in CDFI (type IV). The patient declined the FNA or CEUS proposal on Feb 2013. (C) 42 months later, the nodule was observed again during a scan of the carotid. This nodule was slightly enlarged (9×7 mm). (D) ACLN was observed on the ipsilateral upper neck (14×5 mm). (E) Both periphery and interior blood flow in CDFI. The patient submitted to total thyroidectomy with prophylactic lymph node dissection. Histopathologic examination confirmed PTC and cervical lymph node metastasis. (All patients included in the present study were assessed for FNA and CEUS).
A 73-year-old woman (A) With an isoechoic, solid, irregular thyroid nodule in right lobe, 25×20 mm in size, 25% capsule contact, FNA revealed TBSRTC level VI. (B) Slightly periphery and absent interior blood flow (type II). (C) Mainly homogeneous, hypoenhancement on CEUS (14 s after SonoVue injection), and there is an enhancement defect on lower right (arrow). (D) ACLN was found on level II (12×8 mm. Histotpathologic examination confirmed PTC and cervical lymph node metastasis. (The patient was not included in present study because ALCN could be detected by US before operation). The three elements: big size, hypoenhancement and cervical lymph node metastasis were consistent.
The present study has several limitations: First, no single conventional ultrasonography or CEUS characteristics were able to conclusively distinguish metastatic thyroid nodules from indolent ones. The three most valuable conventional ultrasonography and CEUS characteristics for prediction of CLNM were found to be intensity at peak time, size, and capsule contact. However, the AUC values of these three characteristics were still below 0.7, so the combination of several elements may have better predictive power. Second, the sample size of the population was small (37 patients with CLNM in 186). Moreover, patients with multiple PTC nodules were excluded because it is not clear which PTC nodule caused cancer metastasis. Third, patients who did not undergo total thyroidectomy were excluded, which may have introduced selection bias.
In summary, the CEUS patterns of PTC are relative to not only the size of PTC but also the possibility of CLNM after thyroidectomy. Iso- or hypo-enhancements at peak time seem to predict CLNM prognoses in PTC patients.
Footnotes
Acknowledgments
Xue-hong Diao contributed equally to this work and should be considered co-first authors. This study was funded by the Medical Guide Project of the Shanghai Science and Technology Commission (grant No.14411970400).