
Abstract
OBJECTIVE:
To investigate the correlation of carotid intima-media thickness (IMT) with endothelial function and atherosclerosis degree in patients with type 2 diabetes mellitus.
METHODS:
A total of 80 patients with type 2 diabetes mellitus admitted and treated in our hospital from January 2017 to January 2018 were selected and randomly divided into two groups (n = 40). Patients who were definitely diagnosed with type 2 diabetes mellitus were selected as observation group, and individuals who received health examination and were excluded from type 2 diabetes mellitus were enrolled as control group. The diagnosed proportions of carotid plaque, Crouse scores, endothelial-dependent flow-mediated vasodilation (FMD) function and nitroglycerin-mediated dilation (NMD) function of the brachial arteries in the two groups were compared. The indexes related to vascular endothelial functions [vascular endothelial growth factor (VEGF), endothelin-1 (ET-1) and nitric oxide (NO) levels] in the two groups were detected. The correlations of Crouse score with brachial arterial FMD value, VEGF level, ET-1 level and NO level in observation group were analyzed.
RESULTS:
The diagnosed proportion of carotid plaque in observation group was significantly higher than that in control group (P < 0.05), and the Crouse score in observation group was higher than that in control group (P < 0.05). The brachial arterial FMD value in observation group was remarkably lower than that in control group (P < 0.05). Compared with control group, VEGF and ET-1 levels were significantly reduced in observation group (P < 0.05), with the statistical increase of NO level (P < 0.05). In observation group, the Crouse score was negatively correlated with the brachial arterial FMD value, VEGF level and ET-1 level, whereas positively correlated with the NO level (P < 0.05).
CONCLUSION:
Our data show that the carotid IMT is increased significantly among patients with type 2 diabetes mellitus, and the vascular endothelial function is impaired. Moreover, after the occurrence of atherosclerosis, we found the carotid IMT is negatively correlated with endothelial-dependent FMD, as well as levels of VEGF and ET-1, whereas shows positive correlation with the vasodilative factor NO.
Introduction
Macroangiopathy, as a relatively serious complication of diabetes mellitus, often represents a leading cause of life-threatening complications and even clinical death of the patients [1], of which the atherosclerosis-induced acute myocardial infarction or cerebral infarction is caused by macroangiopathy [2]. Clinically, it is too late for the treatment of atherosclerosis after the myocardial infarction occurs. Therefore, it is of great importance to discover and diagnose intimal lesions in the early stage and find mild and moderate early lesions [3]. Noninvasive color Doppler ultrasonography and contrast enhanced ultrasound (CEUS) developed in recent years present diagnostic means that can discover atherosclerosis in the early stage and effectively diagnose the increased intima-media thickness (IMT), thus providing a basis for clinical diagnosis of atherosclerosis [4–6].
The occurrence of macroangiopathy, especially atherosclerosis, is an essential cause of disability and death regarding to type 2 diabetes mellitus [7]. The red blood cell characteristics on diabetic retinopathy development and progression suggest prognostic value in type 2 diabetes mellitus [8]. It has been demonstrated that the detection of microcirculation disorders contributes to predictive value by using laser Doppler flowmetry in diabetes mellitus [9, 10]. Carotid IMT can efficiently predict the conditions of systemic atherosclerosis that is regarded as early characteristic changes. It was indicated [11] that carotid IMT was closely associated with the early macrovascular complications of diabetes mellitus. In addition, the vascular endothelial dysfunction occurs earlier than the anatomical changes in the carotid IMT. Therefore, it is believed [12] that the impairment of vascular endothelial function plays a crucial role in the occurrence and development of macroangiopathy of type 2 diabetes mellitus, especially the atherosclerosis. In order to improve the prognosis of patients with type 2 diabetes mellitus, ameliorate the value of clinical treatments, prevent and reduce the occurrence of macrovascular complications, particularly acute myocardial infarction and ischemic stroke, the correlations of carotid IMT with vascular endothelial functions in patients with type 2 diabetes mellitus were thus investigated in this study.
Patients and methods
General data
A total of 80 patients with type 2 diabetes mellitus admitted and treated in our hospital from January 2017 to January 2018 were selected. All the patients were definitely diagnosed with diabetes mellitus via fasting blood glucose test, random blood glucose test, glucose tolerance test, glycosylated hemoglobin level test, etc. before enrollment. The informed consent of this study was signed before enrollment. The study was approved by the Clinical Research Ethics Committee of Weihai Central Hospital (WCH-20161205). The patients were aged 45–75 years old, with duration of diabetes mellitus of more than 1 year. Exclusion criteria: 1) patients with severe insufficiency or dysfunction of heart, lung, liver or kidney, 2) patients diagnosed with type 1 diabetes mellitus, 3) patients complicated with other endocrine-associated diseases, hyperlipidemia or hypertension, 4) patients receiving treatment with neck surgery, 5) patients treated with anticoagulant therapy or antiplatelet therapy within 1 month before enrollment, 6) patients with mental aberration, 7) patients with past history of stroke, or 8) patients refusing to be enrolled. The patients were randomly divided into two groups (n = 40). The observation group included 21 males and 19 females aged 45–75 years old, with an average age of (66.3±2.0) years old. The duration of diabetes mellitus was 1–30 years, with average duration of (11.0±1.0) years, and the duration of atherosclerosis was 1–20 years, with average duration of (8.1±0.3) years. In the control group, there were 20 men and 20 women aged 45–75 years old, with an average age of (66.4±2.0) years old. The duration of diabetes mellitus was 1–31 years, with average duration of (11.1±1.0) years, and the duration of atherosclerosis was 1–21 years, with average duration of (8.1±0.3) years. Comparisons of gender, age, duration of diabetes mellitus and duration of atherosclerosis between the two groups showed that the differences were not statistically significant (P > 0.05).
Methods
Patients who were definitely diagnosed with type 2 diabetes mellitus were selected as observation group, and individuals who received health examination and were excluded from type 2 diabetes mellitus were enrolled as control group. Relevant clinical examinations were performed for all the enrolled subjects, of which indexes related to carotid atherosclerosis, as well as brachial artery-associated indexes [endothelial-dependent flow-mediated vasodilation (FMD) and nitroglycerin-mediated dilation (NMD)], were detected through carotid color Doppler ultrasonography. The diagnosed proportions of carotid plaque, Crouse scores, FMD and NMD of the brachial arteries in the two groups were compared. The indexes related to vascular endothelial functions [vascular endothelial growth factor (VEGF), endothelin-1 (ET-1) and nitric oxide (NO) levels] in the two groups were detected. Moreover, the correlations of Crouse score with brachial arterial FMD value, VEGF level, ET-1 level and NO level in observation group were analyzed.
Evaluation criteria
Carotid atherosclerosis detection criteria: GE Vivid 7 color Doppler ultrasonic apparatus, with an ultrasonic probe frequency of 4–8 MHz, was adopted. During examination, the patients kept in the supine position, with the head turned to the contralateral side. The bilateral carotid IMT was detected using color Doppler ultrasonography, of which the scanned positions were common carotid arteries, carotid bifurcations and 2 cm away from the proximal part of internal carotid arteries. Clinical diagnostic criteria of carotid atherosclerosis: the intima was smooth and complete, and the IMT < 1.0 mm was regarded as normal, IMT at 1.0–1.5 mm as thickened carotid intima, and IMT > 1.5 mm as formation of carotid plaque. Examinations of vascular endothelial functions included VEGF (solid-phase sandwich method enzyme-linked immunosorbent assay: 0–154 mg/L), ET-1 (radioimmunoassay: 43.50–58.38 ng/L) and NO (enzyme-linked immunosorbent assay). Crouse score of carotid ultrasound: IMT value indicated the sum of thickness of each independent plaque in bilateral carotid arteries of enrolled subjects with formed plaque. FMD and NMD were calculated via the following formula: [artery diameter detected at sudden deflation for 60 s (conducted at 5 min after compression test)—baseline artery diameter at resting state]/baseline artery diameter at resting state ×100%.
Statistical processing
Statistical Product and Service Solutions (SPSS) 13.0 was applied. Measurement data were presented as mean±standard deviation
Results
Comparisons of diagnosed proportion of carotid plaque and Crouse score between the two groups
The diagnosed proportion of carotid plaque in observation group was significantly increased compared with that in control group (P < 0.05), and the Crouse score in observation group was higher than that in control group (P < 0.05) (Table 1).
Comparisons of diagnosed proportion of carotid plaque and Crouse score between the two groups
Comparisons of diagnosed proportion of carotid plaque and Crouse score between the two groups
The brachial arterial FMD value in observation group was remarkably lower than that in control group (P < 0.05), but there was no statistically significant difference of the NMD value between the two groups (P > 0.05) (Table 2).
Comparisons of brachial arterial FMD and NMD functions between the two groups
Comparisons of brachial arterial FMD and NMD functions between the two groups
Compared with control group, VEGF and ET-1 levels were significantly decreased in observation group, with statistical elevating NO level (P < 0.05) (Table 3).
Comparisons of indexes related to vascular endothelial function between the two groups
Comparisons of indexes related to vascular endothelial function between the two groups
In observation group, the Crouse score was negatively correlated with the brachial arterial FMD value (r = –0.9716, P = 0.000 < 0.05) (Fig. 1).
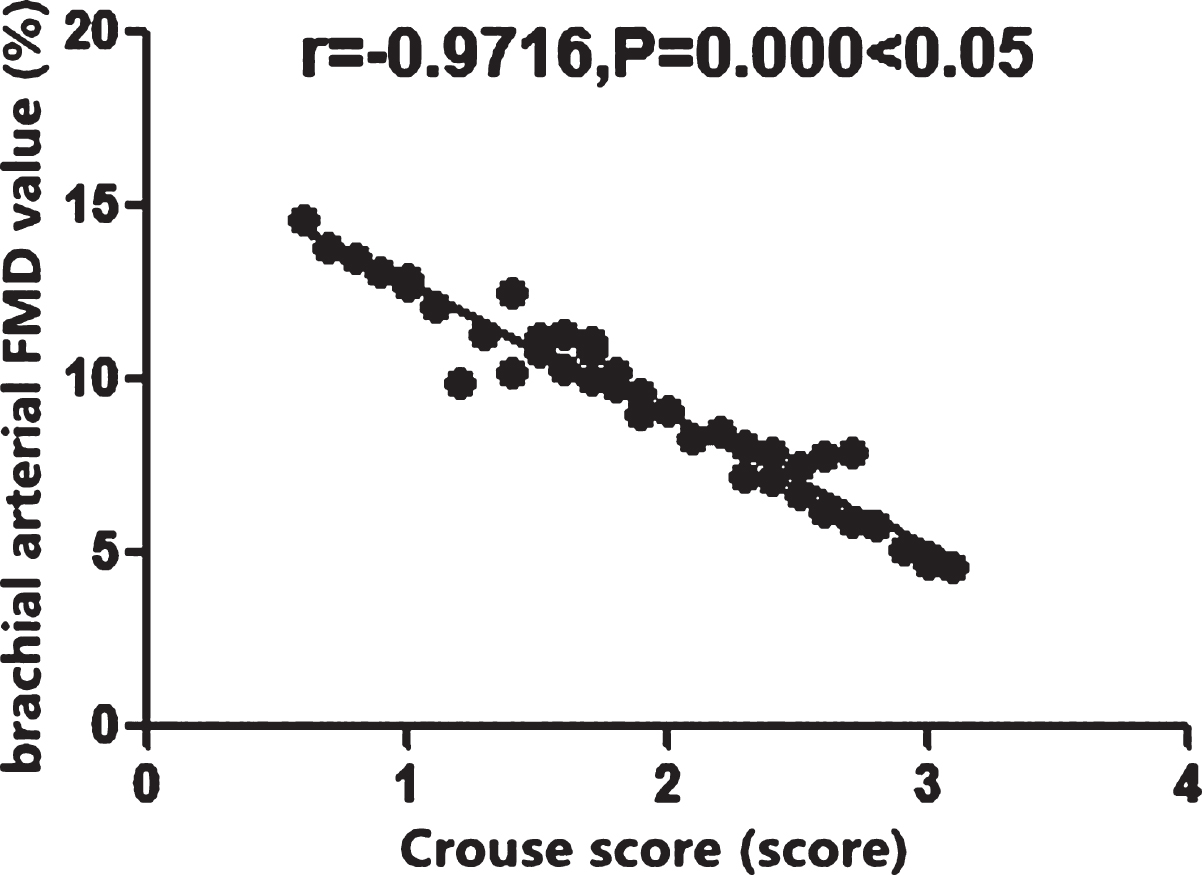
Correlation of Crouse score with brachial arterial FMD value in observation group. In observation group, the Crouse score is negatively correlated with the brachial arterial FMD value (P < 0.05).
The Crouse score in observation group was negatively correlated with the VEGF level (r = –0.9701, P = 0.000 < 0.05) (Fig. 2).
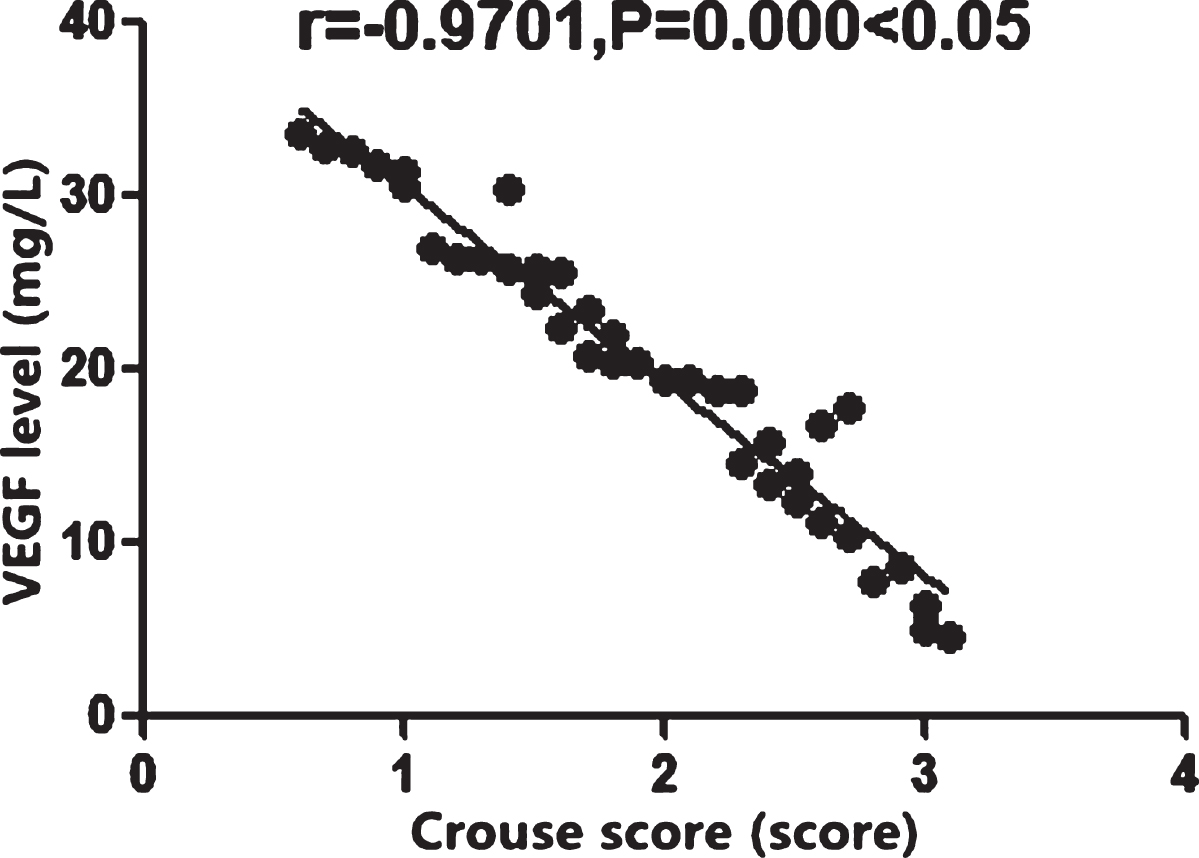
Correlation of Crouse score with VEGF level in observation group. The Crouse score in observation group is negatively correlated with the VEGF level (P < 0.05).
The Crouse score was negatively correlated with the ET-1 level in observation group (r = –0.9756, P = 0.000 < 0.05) (Fig. 3).

Correlation of Crouse score with ET-1 level in observation group. The Crouse score is negatively correlated with the ET-1 level in observation group (P < 0.05).
In observation group, the Crouse score was positively correlated with the NO level (r = 0.9428, P = 0.000 < 0.05) (Fig. 4).
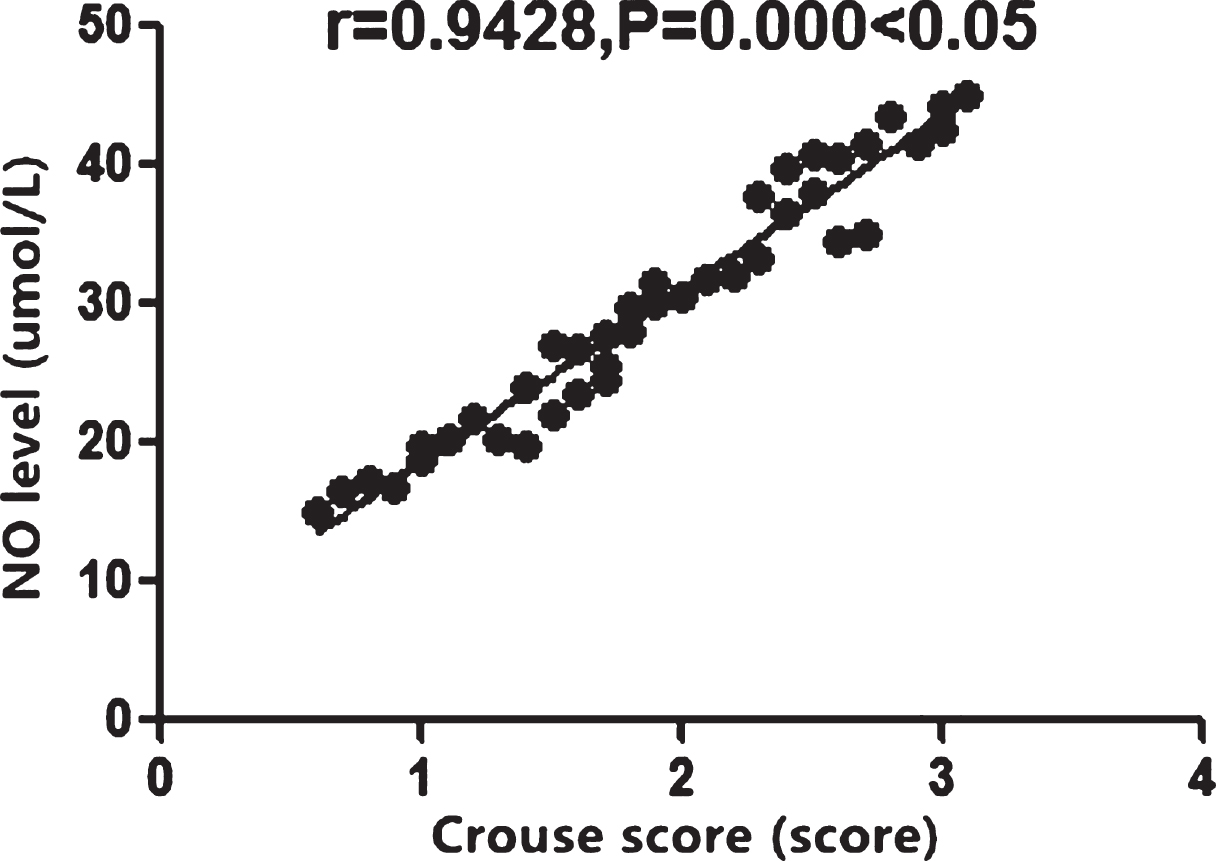
Correlation of Crouse score with NO level in observation group. In observation group, the Crouse score is positively correlated with the NO level (P < 0.05).
The incidence rate of diabetes mellitus is elevated remarkably with the multiple changes in people’s lifestyle and diet habit in recent years [13]. Previous study in an epidemiologic investigation with large samples conducted by Chinese Diabetes Society found that the prevalence of type 2 diabetes mellitus among adults aged 20 years or above is close to 10% [14]. In addition, the incidence rate of the disease rises obviously with the increasing age, and this proportion increases higher than 30% in patients aged more than 60 years old. The major hazard of diabetes mellitus is causing irreversible chronic complications in the body, which are more common and serious in kidney and great vessels [15]. The clinical application of color Doppler ultrasound can non-invasively detect the carotid IMT, identify the formation of atherosclerotic plaque and measure the endothelial dilatation function of brachial artery, thus effectively predicting the possibility of macrovascular complications in patients with type 2 diabetes mellitus [16]. Therefore, the carotid IMT examination combined with vascular endothelial function determination is of great value for predicting the progression of large artery atherosclerosis in patients with type 2 diabetes mellitus and judging their prognosis.
In this study, observation group consisted of patients definitely diagnosed with type 2 diabetes mellitus, and control group enrolled subjects who received health examination and were excluded from type 2 diabetes mellitus. The comparisons of diagnosed proportion of carotid plaque and Crouse score between the two groups indicated that the diagnosed proportion of carotid plaque, as well as Crouse score in observation group were significantly higher than that in control group. In addition, it was found by investigating the brachial arterial FMD and NMD functions as well as indexes related to vascular endothelial functions between the two groups that the brachial arterial FMD value in observation group was remarkably smaller than that in control group. In previous studies, flow-mediated vasodilation (FMD) function was shown improved after low-volume high-intensity interval training in type 2 diabetes, which was associated with the diet habit [17, 18]. Glycemic variability, along with certain types of medicines, fluvastatin and valsartan, affects the development of type 2 diabetes [19, 20]. Insulin resistance, subclinical atherosclerosis and vascular responsiveness are also implicated to type 2 diabetes mellitus [21, 22]. In our study, therefore, we tested the function of FMD. Since endothelin can in deed induce the aggregation of leukocytes, we thus evaluate the ET-1 level [23]. VEGF induces the formation of NO, leading to vasodilation and increased vascular permeability [24]. Of note, compared with control group, observation group was implicated with lower VEGF and ET-1 levels and higher NO level, indicating that the endothelial-dependent FMD function is decreased in patients with type 2 diabetes mellitus. The levels of vascular endothelial cell regulating factors (VEGF and ET-1) in the body decline, while the levels of vasodilative factors (NO, etc.) are elevated. Meanwhile, the correlations of Crouse score with brachial arterial FMD value, VEGF level, ET-1 level and NO level in observation group were studied, and it was revealed that the Crouse score was negatively correlated with the brachial arterial FMD value, VEGF level and ET-1 level, but positively correlated with the NO level. It indicates that the vascular endothelial function of the patients with type 2 diabetes mellitus is impaired, resulting in declined endothelial-dependent FMD function.
As for patients with type 2 diabetes mellitus, damage of vascular endothelial function caused by microcirculation dysfunction and chronic ischemia and hypoxia of tissue [25] can lead to decreased release of VEGF and ET-1 [26] and reactively up regulate the level of vasodilative factor NO. At the same time, the reduction of VEGF and ET-1 levels [27] can induce aggregation of leukocytes in capillaries and increase of vascular permeability, thereby causing hyperplasia of vascular smooth muscle and formation of thrombus in a feedback manner and further aggravating microvascular dysfunction [28]. The carotid IMT of the patients with type 2 diabetes mellitus is elevated, and the endothelial-dependent FMD function is decreased, which may be associated with the arterial intimal injury induced by long-term chronic hyperglycemia [29]. Moreover, the levels of inflammatory mediators, VEGF and ET-1 in the body are elevated, and the feedback release of vascular adhesion molecules is boosted [30], resulting in slower microcirculatory blood flow and further vasoconstriction [31]. Meanwhile, the thrombus is formed through platelet adhesion and aggregation, which may trigger growing levels of fibrinolysis inhibitors and declining antifibrinolytic substances [32], further exacerbating the carotid IMT and inducing disorders of the vascular endothelial structure and function [33].
In conclusion, for patients with type 2 diabetes mellitus, the carotid IMT is increased significantly, and the vascular endothelial function is impaired. After the occurrence of atherosclerosis, the carotid IMT is negatively correlated with endothelial-dependent FMD, VEGF and ET-1 levels, but positively associated with the vasodilative factor NO.
Disclosure of conflict of interest
None.