
Abstract
Uterine arteriovenous malformation (AVM) is an extremely rare condition characterized by abnormal connections between veins and arteries. The atypical clinical manifestations and relatively low morbidity of AVM are conducive to missed diagnosis. The present study describes a case of a 47-year-old female patient with congenital uterine AVM followed by iatrogenic AVM. The diagnosis was established by contrast-enhanced ultrasound combined with contrast-enhanced CT (CECT). Because the symptom of vaginal bleeding was severe, trophoblastic disease or neoplasia could be preferred. The manifestations on various imaging examinations were carefully assessed, and the relevant literature was also reviewed.
Keywords
Introduction
Uterine arteriovenous malformation (AVM) is a rare but life-threatening disease[1–3] that occurs frequently in women of reproductive age and is classified as either acquired or congenital. Acquired uterine AVM is mostly caused by previous uterine surgery [4, 5]. Congenital AVM is caused by a vascular malformation. In this condition, arteries and veins are directly connected without passing through the capillary network. The clinical symptoms of uterine AVM are primarily abnormal vaginal bleeding, including hypermenorrhea and massive vaginal bleeding [6].
The various features of uterine AVM on ultrasound images have been delineated in case reports, but the contrast-enhanced ultrasound (CEUS) appearance of uterine AVM has not been clearly described. In this manuscript, we report a case of uterine AVM described as congenital uterine AVM followed by iatrogenic uterine AVM on CEUS and CECT. Manifestations on multifarious imaging examinations were carefully assessed, and the relevant literature was also reviewed.
The case report
A 47-year-old female patient was referred to the present hospital for further investigation by another hospital due to persistent lower abdominal pain and irregular vaginal bleeding for five months. During that period, the patient was diagnosed with cervical polyps at a local county hospital. After cervical polypectomy, the patient experienced constant vaginal bleeding. To stop the vaginal bleeding and clarify the cause, the patient was treated with curettage. However, 10 days after curettage, the patient experienced a high volume of menstrual flow.
Laboratory examination showed low hemoglobin (Hb, 88 g/L; normal range, 115–150 g/L), slightly elevated platelets (PLT, 402×10∧9; normal range, 125–350×10∧9), moderately elevated thyrotrophic hormone (7.95 μIU/ml; normal value: 0.3–5.5 μIU/ml) and significantly elevated estradiol (716, 20–40 Pg/ml). Other laboratory data including β-HCG, HBsAg, erythrocyte sedimentation rate, blood coagulation tests, blood biochemical tests, and urinalysis were all within normal ranges.
The patient subsequently underwent conventional US, CEUS, CECT examinations and digital subtraction angiography (DSA) in our hospital. The imaging findings, including previous imaging studies, were obtained as follows.
Imaging findings
Conventional US
Conventional US and CEUS were performed with a LOGIQ E8 scanner (GE Healthcare, Milwaukee, WI, USA) and a 3–10 MHz transducer. The conventional US results showed that hypoechoic area of the uterus anterior wall myometrium close to the endometrium was 3.6×3.2×2.9 cm with ill-defined edges, and color Doppler flow imaging (CDFI) showed a distorted and expanded blood flow signal. Dilated, tortuous vessels were visible on the left side of the uterus. Pulsed wave (PW) ultrasound showed a turbulent spectrum and venous blood flow at the peak of systole. Uterine and pelvic blood flow exhibited a high velocity and low resistance with a peak systolic velocity (PSV) of 63 cm/s and a resistance index (RI) of 0.28. The initial diagnosis was suspicion of uterine AVM with conventional US (Fig. 1).
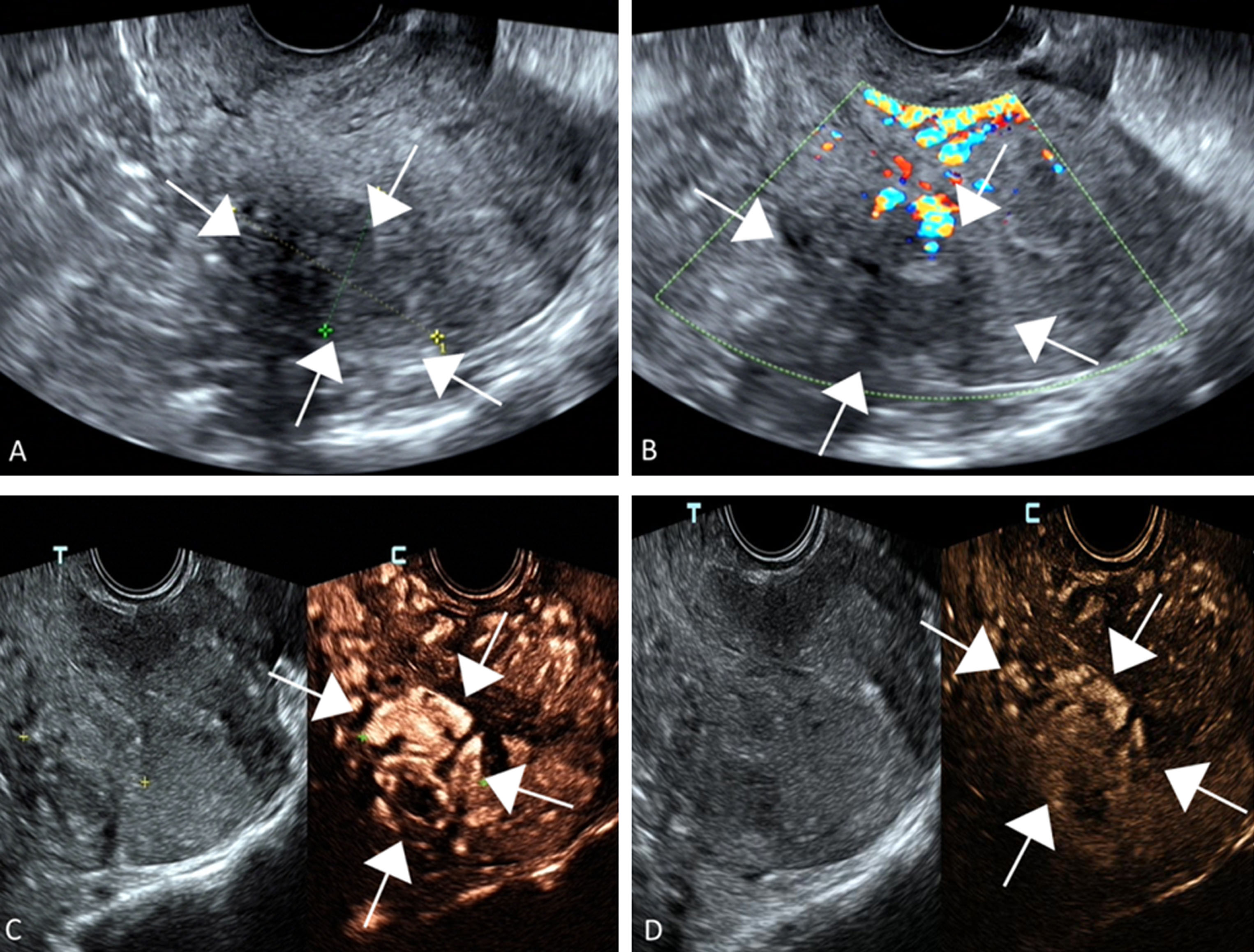
(A) Grayscale US image shows an inhomogeneous hypoechoic and ill-defined lesion (white arrow) measuring 3.6 cm×3.2 cm×2.9 cm in the anterior wall of the myometrium of the uterus. (B) Color Doppler flow imaging (CDFI) shows the distorted and expanded blood flow signal on the left side of the uterus. (C) Arterial phase (15 sec) on CEUS: The lesion (white arrow) appears defined, with obvious enhancement compared with the surrounding normal uterine tissue. (D) Late venous phase (62 sec) on CEUS: Microbubbles washed out from the lesion, and hypo-enhancement of the lesion is observed.
CEUS was performed with injection of 2 ml of SonoVue (Bracco, Milan, Italy) followed by 5 ml of sterile saline [7, 8]. Contrast-enhanced uterine ultrasound showed that enhancement of the hypoechoic area of the uterus anterior wall began at 9 s and peaked at 15 s after SonoVue injection, significantly earlier than in the surrounding normal uterine tissue, with a fast-forward and low-out mode (Fig. 1).
CECT
Plain computed tomography (CT) scanning showed a slightly low-density mass-like shadow on the left side of the attachment area and at the boundary between several layers, and the uterus was unclear. Enhanced CT scanning identified multiple shadows of tortuous dilated blood vessels in the arterial phase. The mass-like, low-density lesion was diagnosed as a uterine AVM [9] (Fig. 2).
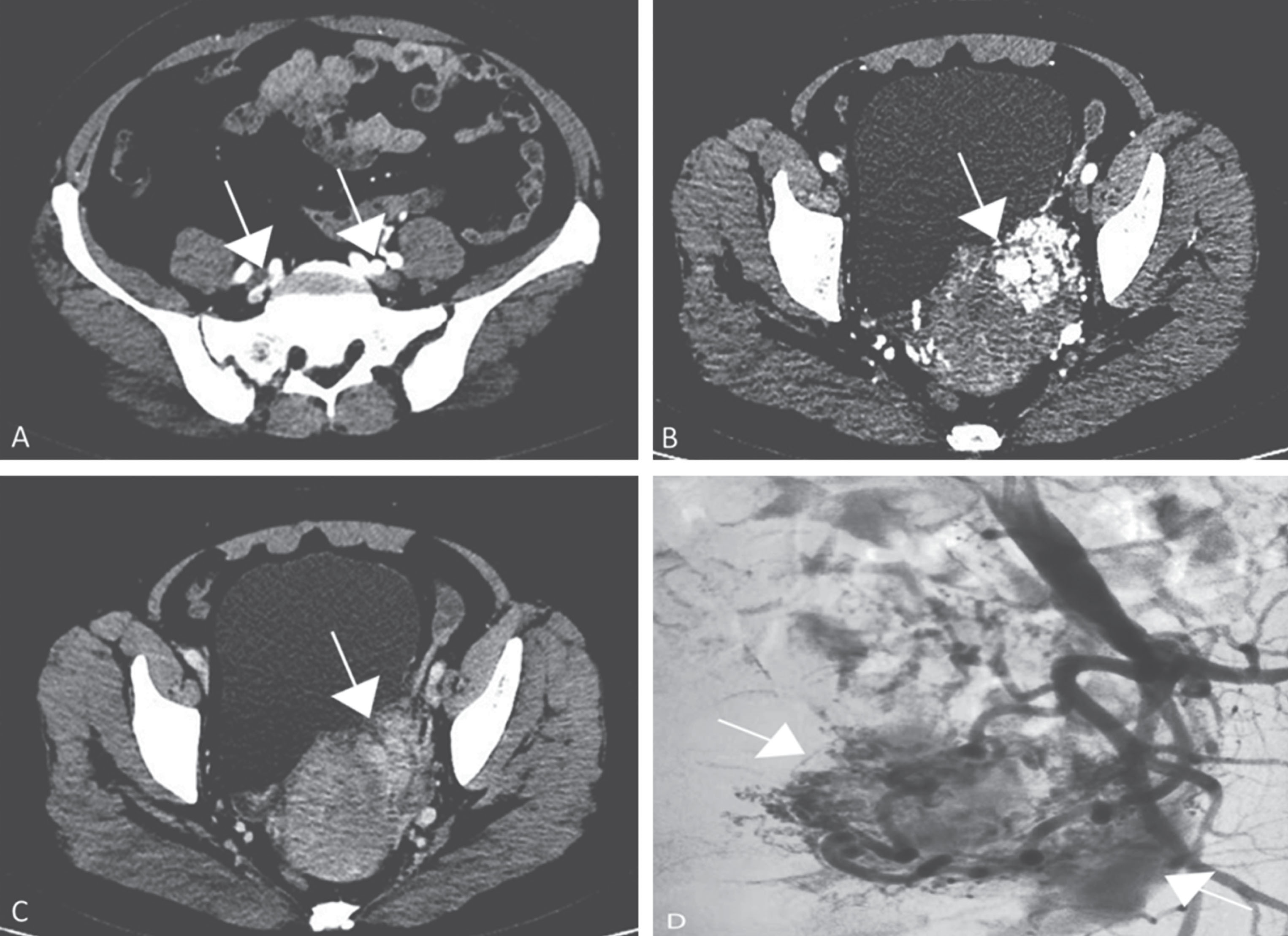
(A), (B) Arterial phase on CECT: Multiple shadows of tortuous dilated blood vessels are visible in the lesion (white arrow) in the arterial phase. Arterial phase on CECT: (C) Plain computed tomography (CT) scanning shows a slightly low-density mass-like shadow on the left side of the attachment area and at the boundary between several layers. The uterus is unclear. (D) DSA showed a non-functional and abnormal communicating branch between the uterine vein and artery.
DSA showed a non-functional and abnormal communicating branch between the uterine vein and artery. Then, the patient underwent left internal iliac arterial embolization, during which a “gelatin sponge granule” was placed into the lesioned artery for embolization, and the left uterine artery was selectively embolized [10]. After the surgery, the patient experienced slight pain in the lower abdomen, and a small amount of irregular vaginal bleeding occurred; no chest tightness or shortness of breath were reported. The patient had a normal menstruation cycle after discharge. After 3 months, ultrasonography showed remaining irregular echoes in the uterine muscle wall with slightly enriched blood flow. The blood flow in the pelvic cavity of the left uterus was slightly increased, and the flow rate was significantly lower than that before surgery. The patient had no symptoms of vaginal bleeding and achieved clinical cure (Fig. 2).
Discussion
Uterine AVM is a rare disease and can be classified as congenital or acquired. Congenital uterine AVM is the result of abnormal connections between veins and arteries. Acquired uterine AVM is caused by routine gynecological procedures (such as curettage), trophoblastic disease, etc. [11–14]. This kind of acquired uterine AVM is also known as iatrogenic AVM. The patient described in this article suffered massive vaginal bleeding after cervical polypectomy.
Due to the unspecific clinical symptoms and rare nature of uterine AVM, the experience of clinicians with this entity is limited, leading to a dismal prognosis. In this report, the lesion in the uterus showed an inhomogeneous hypoechoic region close to the endometrium and ill-defined edges, with an abundant blood flow signal in the lesion, similar to trophoblastic disease or neoplasia.
Uterine AVM shows a variety of findings on conventional US and CECT images [15–20]. Conventional US, a nonspecific imaging modality, of typical uterine AVM lesions often shows intensive rapid blood flow disorder or low-resistance flow and pulsatile venous and high-velocity arterial flow in the myometrium. However, CECT is more expensive than US and requires radiation.
There are few studies of the CEUS characteristics of uterine AVM. CEUS can be used to differentiate most malignant and benign uterine lesions by analyzing the spectrum form of the artery and the features of lesions enhancement. In the present case, the CEUS images were atypical compared with common uterus masses. The lesion exhibited a rapid increase in enhancement that washed out entirely in the venous phase. The lesion appeared significantly earlier and lighter than the surrounding normal uterine tissue and slight lighter than the surrounding normal uterine tissue in the late phase. All uterine AVM lesions are characterized by a remarkable fast-forward and low-out enhancement mode, similar to the enhancement pattern on CECT. This feature may be associated with the abnormal connection between the artery and vein. Digital subtraction angiography (DSA) is the “gold standard” for the diagnosis of uterine AVM [21]. DSA may provide accurate data about the size of the lesion and the relationship and feeding arteries with the pelvic vasculature.
As a convenient examination method, CEUS could adequately depict uterine AVM with some familiar characteristics, thereby providing reliable clues for the diagnosis of this rare disease [22]. CEUS should be routinely used to determine the presence of a uterine AVM, particularly when a patient presents with a large amount of vaginal bleeding and a history of uterine trauma and β-HCG and serum tumor markers are negative.