
Abstract
OBJECTIVE:
To clarify the clinical role of contrast enhanced ultrasound (CEUS) in predicting BI-RADS 4 breast disease.
METHODS:
A total of 92 sites of BI-RADS 4 breast diseases were reassessed by routine ultrasound and CEUS. The main indicators of routine ultrasound, CEUS and the combination of the two modalities were picked up by binary logistic regression analysis, scoring 0 for benign and 1 for malignant characteristics with pathology as referential standard to generate corresponding score systems of them. Finally, the receiver operating characteristic curves (ROC) were applied to compare the diagnostic efficacy of the three score systems.
RESULTS:
As pathological results showing, there were 43 malignant and 49 benign sites in total. Binary logistic regression analysis indicated that the margin, micro-calcification, and hyperechoic halo were main indicators for routine ultrasound score system. The scope expansion and pathological vessels in CEUS were main indicators for CEUS score system. The microcalcification, hyperechoic halo, the scope expansion and pathological vessels in CEUS were main indicators for the combination score system of the two modalities. The sensitivity, specificity and the area under ROC curve (AUC) of routine US, CEUS and the combination of the two modalities score systems were 74.4%, 91.8%, 0.885 and 88.4%, 87.8%, 0.901 and 86.0%, 95.9%, 0.937, respectively.
CONCLUSION:
In summary, CEUS is helpful for us to identify malignant disease and plays a supplementary role in predicting BI-RADS 4 breast disease in some extent. The scope expansion and pathological vessels in CEUS may be the most useful indicators.
Introduction
The most commonly used classification system for breast disease is breast imaging reporting and data system (BI-RADS)[1], which makes the diagnosis of breast disease more standardized and objective. However, the variability between the inter-observer and intra-observer are regularly seen in clinical work-up [2]. This is especially true for BI-RADS 4 breast disease, because of the atypical performance and a certain degree of overlap in their morphological characteristics. Therefore, how to predict BI-RADS 4 breast disease more accurately is still an active research field.
Elastography is now widely considered as a valuable complement to conventional US for its ability in describing the stiffness of breast tumors [3, 4]. But there are also considerable overlaps between the benign and malignant breast tumors as is the case of conventional US. In addition, elastography cannot provide the microvascular distribution information of the breast tumors.
Contrast enhanced ultrasound is a novel technique in detecting the microvascular which is essential for the development, invasive and metastasis of malignant breast tumors. Several previous studies have proved the usefulness of CEUS in diagnosis and prediction of breast diseases, even for the sub-centimeter breast lesions [5–11]. Notwithstanding, no specific pattern indicating malignancy has been identified and no single parameter of ultrasound can completely reflect the variable aspect of breast disease. The main indicators are also uncertain because of changeful feature of breast disease. The wide applications of CEUS in breast diseases still cannot be recommended in routine clinical work-up [12]. And how about the weight of CEUS in diagnosis of breast disease is still unknown. Therefore, in order to discuss the clinical significance and main indicators of CEUS in predicting BI-RADS 4 breast disease, we designed this research to make a fresh discussion.
Materials and methods
Patients selected
Between June 2016 and October 2017, a total of 89 patients (mean age 48 years, range 22-84 years) with 92 breast diseases which were screened primarily as BI-RADS 4 by routine ultrasound or X-ray were gathered for re-assessing by routine ultrasound and CEUS. All patients were scheduled for surgery or biopsy within one week, and all of them have not underwent other special examinations or interventional therapy. All patients were without severe cardiovascular, pulmonary disease and allergic history. Patients in the period of pregnancy and lactation were excluded. And lesions with macro-calcification were also excluded. The final pathological results can be obtained after the whole research.
In out department, CEUS is a routine procedure when the diagnosis is indeterminate or questionable by routine ultrasound. All patients involved were informed of the possible complications and signed a written and informed consent before the CEUS examinations. The research was approved by the ethics committee of our institution.
Equipment and contrast agent
Mylab90 and Twice (Esaote, Genoa, Italy) was used in this study. A linear transducer (LA532) with 8-13 MHz was selected in routine ultrasound. A linear transducer (LA522) with 4.5-7.5 MHz was selected in CEUS and the mechanical index was set less than 0.1, and the gain range was 100-120dB.
Sonovue (Bracco Imaging S.P.A., Milan, Italy) was used as the contrast agent in this study. A suspension was prepared by the addition of 5ml saline solution and 59mg lyophilized powder. A dosage of 2.4ml suspension was injected as a bolus through antecubital vein, following by a flush of 5ml saline solution, and the total dosage was less than 5ml for each patient on the same day.
Ultrasound examination
All the ultrasound examinations were performed by a same sonographer who had 6 years of experience in breast ultrasound and had a professional training in breast CEUS. Routine ultrasound was performed in multiplane with the equipment mentioned above. The largest plane of suspicious lesion was selected for the following CEUS procedure. The selected plane should include the lesion and the surrounding normal tissues as far as possible. The focus was set at the nearest rear of the lesion and should not be above the center of the lesion. Single image was used to remain enough surrounding tissue for comparing. But, when the lesion was too small to be located accurately during the procedure, dual images were applied. The probe was kept static during CEUS procedure. However, when the lesion was too big to be observed in one plane, the probe can be moved to the junction of the disease and normal tissue to observe the margin of the lesion during CEUS procedure. No parameters need to be changed during examination. A two minutes dynamic cine was acquired for analysis.
Images analysis
All images were read by two senior sonographers who had at least 10 years of experience in breast ultrasound and 2 years of experience in breast CEUS. All records were under an agreement of the two sonographers. The third sonographer with more experience was invited to make a final decision when disagreement occurred. During the whole research, all sonographers were blinded to patients’ clinical data and pathological results. After prospective read of the images, the final decisions of the ultrasound images and pathological results were inputted into a computer by an assistant who had nothing to do with the research, and the final data was analyzed by another researcher.
According to literatures and our clinical experience, the indicators of routine ultrasound and CEUS were defined as:
[1] Morphology (2 types): regular (round or oval), and irregular (non-round or non-oval); [2] Margin (2 types): clear structure, and unclear structure (burr-like, angulation or leaflet; [3] Micro-calcification (2 types): invisible and visible; (4) Hyperechoic halo (2 types): invisible and visible; (5) Vascular distribution in color doppler (2 types): absent or less than three strips, and rich or net-like blood flow; (6) Enhancement direction (2 types): diffuse or centrifugal (the diffusion of the microbubbles begin at the center of the lesions or no specific directions), and centripetal (the diffusion of the microbubbles begin at the periphery of the lesion); (7) Enhancement order (2 types): slow rise and rapid rise (compared with the surrounding normal breast tissues); (8) Enhancement degree (2 types): hypoechoic or isoechoic and hyperechoic (compared with the surrounding normal tissues); (9) Enhancement range (2 types): equal or shrink or undistinguished, and expansion (compared with the diameter in any dimension measured by routine ultrasound, Figure 2); (10) Enhancement boundary (2 types): clear and unclear; (11) Enhancement homogeneity (2 types): homogeneous, and heterogeneous (including perfusion defect); (12) Pathological vessels (2 types): absent, and present (including crab claw-like surrounding vessels or coarse twisted blood vessel or penetrating vessels, Figure 3, 4 and 5).
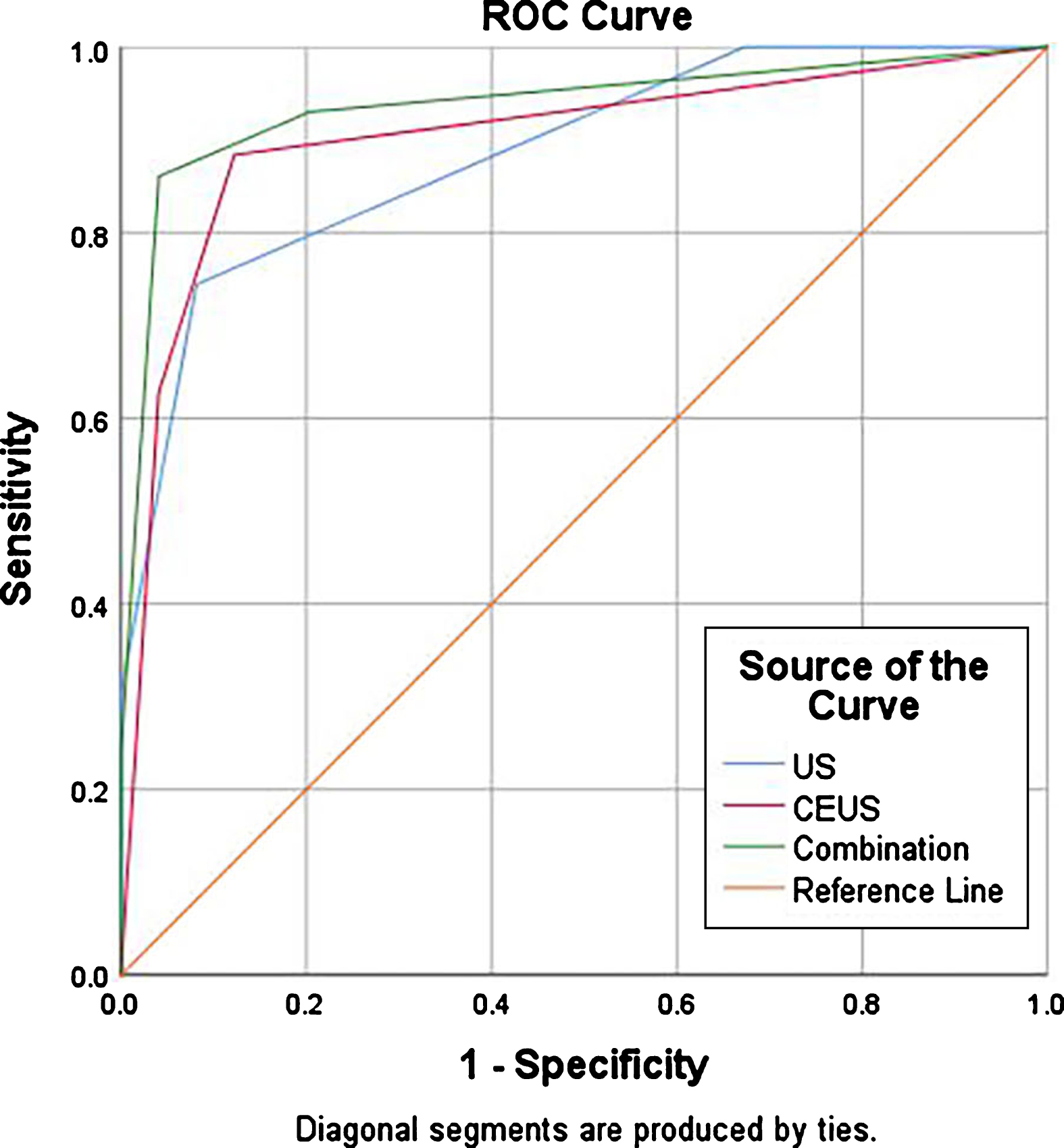
Graph of receiver operating characteristic curve analysis of routine ultrasound, CEUS and the combined score systems for differential diagnosis of breast disease.
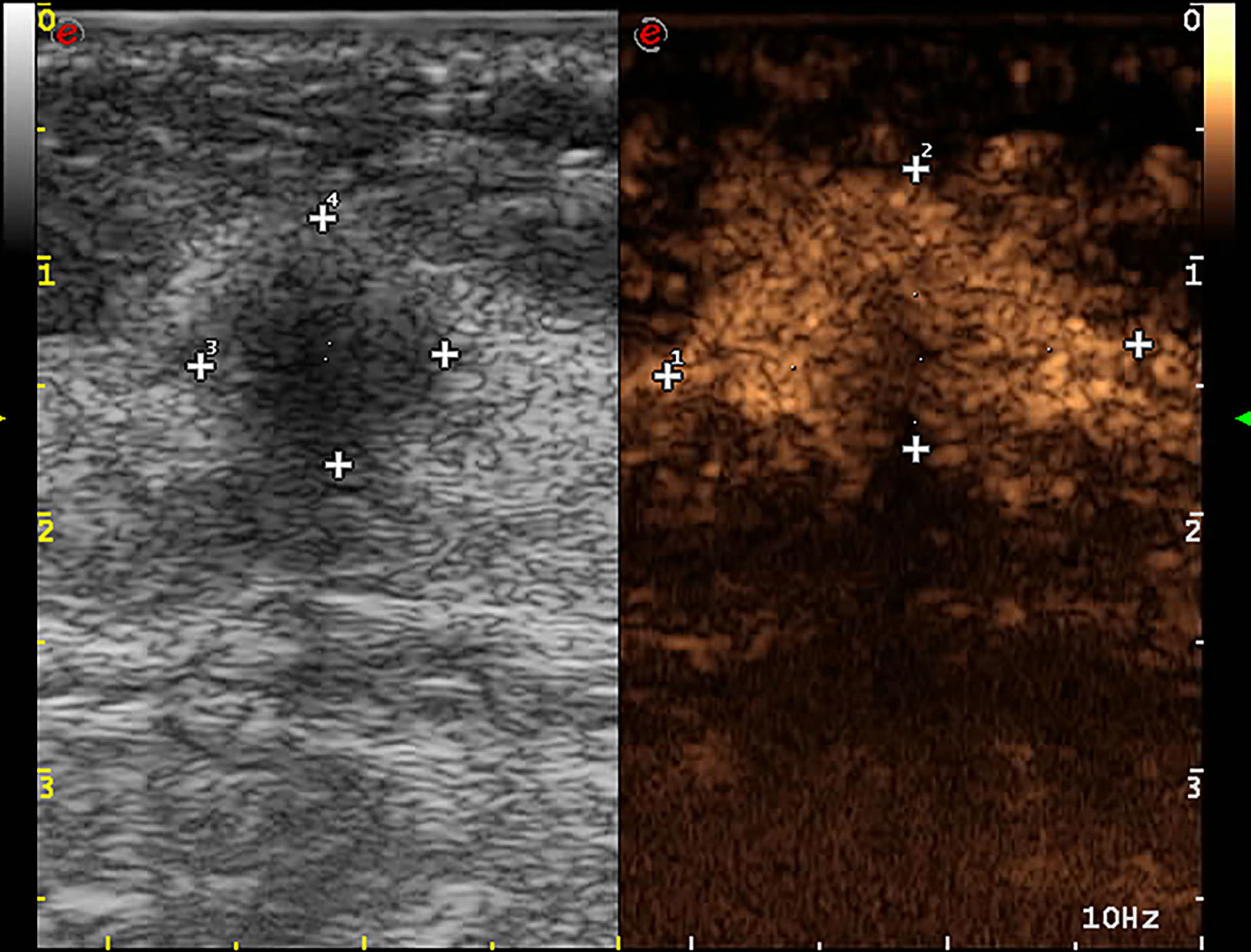
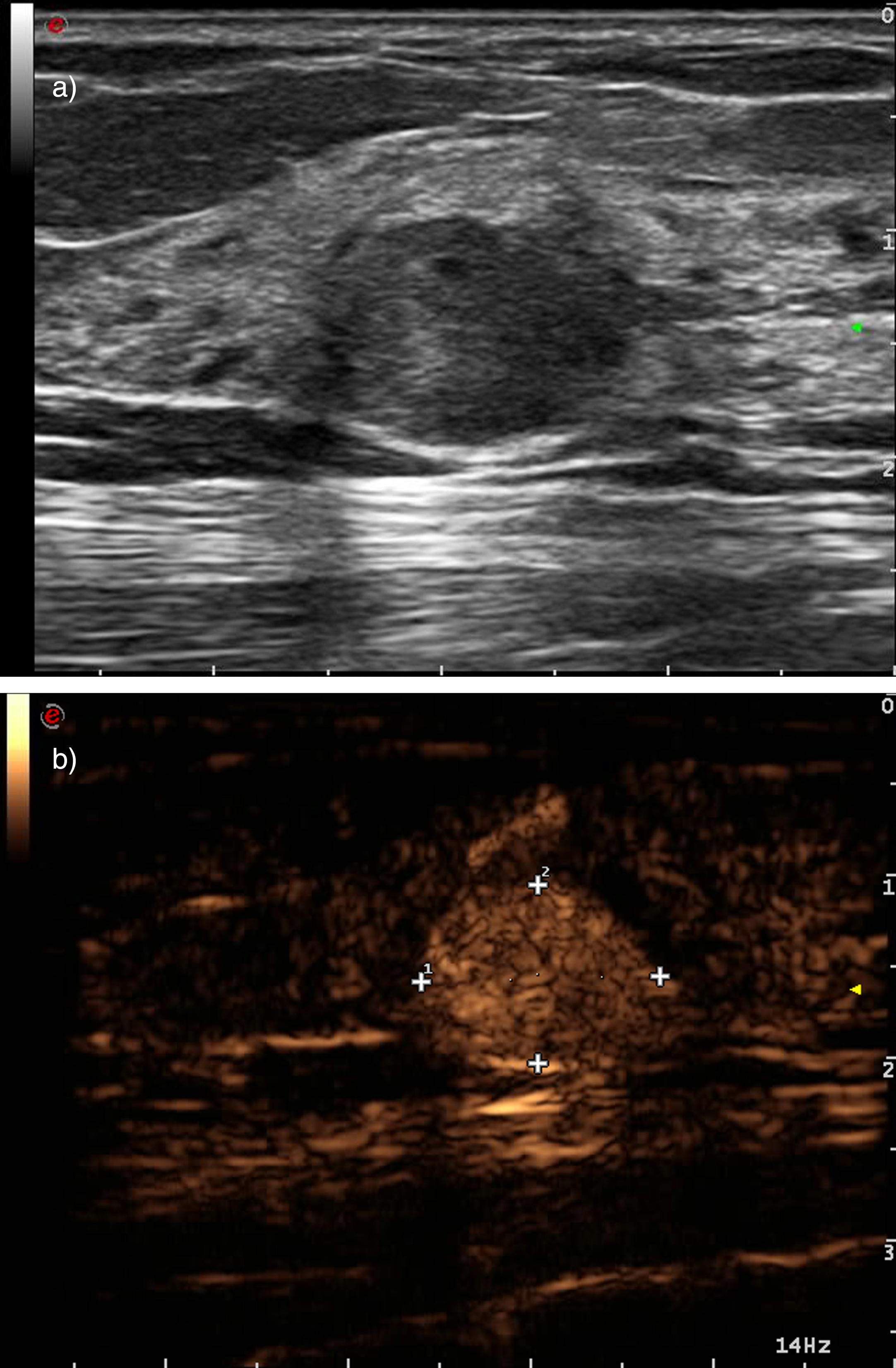
An invasive ductal carcinoma, the scope of the lesion became larger in contrast enhanced ultrasound than routine ultrasound.
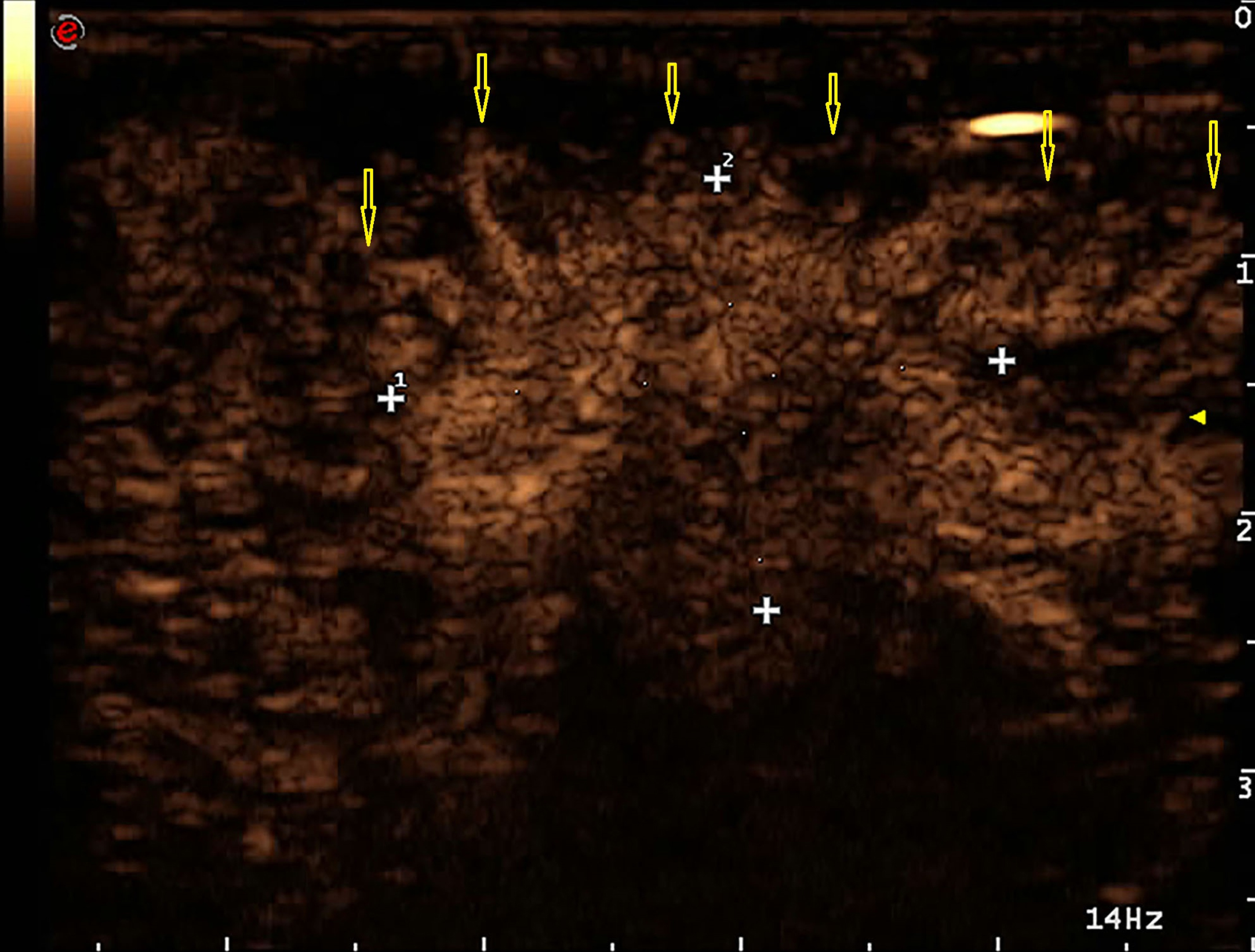
An invasive ductal carcinoma, yellow arrows indicated crab claw-like vessels at the periphery of the lesion in contrast enhcanced ultrasound, just like “tree roots”.

An invasive ductal carcinoma, yellow arrows indicated penetrating vessels of the lesion in contrast enhcanced ultrasound.
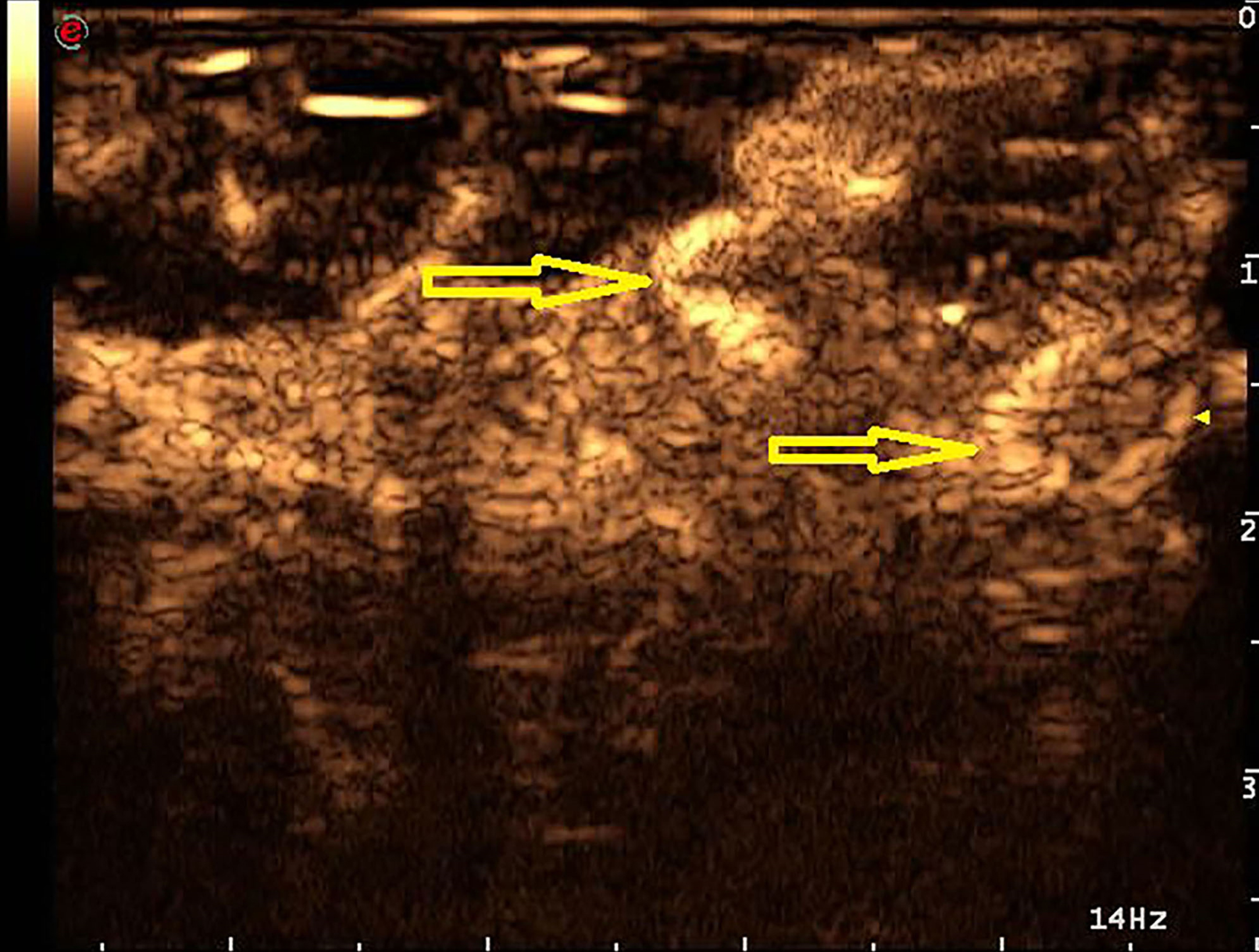
A ductal carcinoma in situ with microinvasion, yellow arrows indicated coarse twisted vessels in contrast enhanced ultrasound.
SPSS 25.0 software was used to analyze the data. Categorical data was analyzed by Pearson χ2 test. The binary logistic regression analysis with forward condition was used to choose the main indicators which were included in the three score system (p value for entry and removal were 0.05 and 0.01, respectively).
Main results
Histopathological findings
A total of 92 breast diseases were obtained pathological results, 49 of them were benign and 43 were malignant. The benign diseases consisted of 21 fibroadenoma, 12 intraductal papilloma, 9 adenosis, 4 inflammation, 2 hyperplasia and 1 residue of breast augmentation. The malignant diseases consisted of 33 invasive ductal carcinoma, 7 intraductal carcinoma in situ, 1 mucinous carcinoma, 1 recurrence of invasive lobular carcinoma, 1 primary squamous cell carcinoma.
Routine ultrasound analysis
The characteristics of 92 breast disease in conventional US and CEUS.
The characteristics of 92 breast disease in conventional US and CEUS.
Diagnostic efficacy of indicators of conventional US and CEUS by single factor analysis.
The characteristics of 92 breast disease in CEUS were shown in Table 1, and the diagnostic efficacy of indicators were shown in Table 2. There was statistical difference in all 7 indicators which were used in this study between benign and malignant lesions (p<0.05) by single factor analysis. Among all CEUS indicators, 2 of them (including enhanced range and pathological vessels) finally entered into binary logistic regression equator and were selected by the CEUS score system.
Combination of routine ultrasound and CEUS analysis
A total of 12 indicators showed significance statistics difference between benign and malignant by single factor analysis. Among all indicators, 4 of them (including micro-calcification, hyperechoic halo, enhanced range and pathological vessels) were selected by the combination score system.
Score system analysis
According to the results above, 3 indicators were selected into routine ultrasound score system and score range was 0-3. Two indicators were selected into CEUS score system and score range was 0-2. Four indicators were selected into the combination score system and score range was 0-4. The ROC curves indicated the cut-off valued and area under curve of the three score systems were 1.5, 0.885 and 0.5, 0.901 and 1.5, 0.937 respectively. The sensitivity, specificity and accuracy were 74.4%, 91.8%, 83.7% and 88.4%, 87.8%, 88.0% and 86.0%, 95.9%, 91.3% respectively. (Table 3, Figure 1)
Comparison of diagnostic efficacy of the three score system.
Comparison of diagnostic efficacy of the three score system.
Pathological study has proved that microvascular structure has changed earlier than the morphology of cancer and the detection of microvascular is helpful for differentiating benign tumors from malignant [13]. In particular, the application of second-generation contrast agents, such as SonoVue (known as Lumason in the United States), have facilitated the continuous and dynamic observation of tumor microvascular perfusion and expanded the usage range of ultrasound in clinical work-up [9].
Contrast enhanced ultrasound has been shown to provide excellent diagnostic efficacy in differential diagnosis of focal liver lesions [14], but the application in breast disease is still controversial and lacks consensus criteria. We analyzed some indicators of CEUS and routine ultrasound in order to illustrate the clinical significance of CEUS and which indicators have played the main role in diagnosis of BI-RADS 4 breast disease.
Many studies have proved some indicators of CEUS to be useful in differential diagnosis of breast diseases [5, 15], as the same case with our study. However, there also was a little difference. Jun Luo [8] found that 9 out of 10 indicators were selected in the logistic regression analysis. Jian Liu [16] reported that the enhanced homogeneity, expanded diameter and intensity grade were main indicators. Another study [15] demonstrated that approximately half of the homogeneously enhancing lesions on CEUS are malignant and a large enhancing area than pre-contrast was a strong indicator for differential diagnosis. But our results indicated that only enhanced range and pathological vessels played a main role for prediction. The difference may be explained by different samples, machines, contrast agent and subjective experience of sonographers. However, nearly all corresponding studies have identified the scope expansion in CEUS as a strong indicator [7, 15–17]. That is to say, enhancement range may be a general indicator for differentiating breast disease.
In addition, some studies also mentioned that the abnormal vessels observed by CEUS, such as crab claw-like or penetrating vessels were also a typical evident of malignance [7, 17], but no study has collected the homologous phenomenon as one indicator. In our opinion, such as crab claw-like, penetrating and coarse twisted vessels should be considered as a malignant indicator named as “pathological vessels”. As the result showing, this indicator has a relatively favorable diagnostic efficacy and play a main role in the prediction. It reminded us that we should not only pay more attention to enhanced range, but also pathological vessels in CEUS.
How about the weight of CEUS in ultrasonic diagnosis? It is a practical problem. As we all known, all new ultrasonic technologies are based on routine ultrasound images, thus, it will lose clinical value to discuss CEUS without routine ultrasound. According to the analysis of score systems, the results indicated that the predictable ability of CEUS and combination score system were higher than routine ultrasound score system. It illustrated that CEUS can improve the diagnostic efficacy of routine ultrasound to a certain degree. Just as the results showing the sensitivity and specificity of routine ultrasound, CEUS and the combination score system were 74.4%, 91.8% and 88.4%, 87.8% and 86.0%, 95.9% respectively. It also illustrated that CEUS were more sensitive to perform the malignant characteristics of breast disease than routine ultrasound and could provide more stable specificity.
We also found some enhancement patterns were only present in benign tumors. For example, some benign tumors would present unclear margins or irregular morphology in routine ultrasound, but present clear margins or shrinking range in CEUS (Figure 6). Therefore, we concluded that tumors with clear margins or shrinking range in CEUS were indeed benign and this group could be securely downgraded into BI-RADS 3 to avoid biopsy.
(a) a fibroadenoma, a routine ultrsound indicated that the margin was blurr at part of the lesion and classified as BI-RADS 4a; (b) The enhanced range of the lesion was shrink and the margin was clear than routine ultrasound.
In our study, 4 cases (9.3%) out of malignant tumors did not have obviously different characteristics in CEUS from surrounding normal tissues, but they were not missed, because of routine ultrasound characteristic. It reminded us that tumors with isoechoic enhancement in CEUS cannot be downgraded out of BI-RADS 4 group. This point may be different from previous study. Xiao X. etc. [5] have raised 5 score system to analyze CEUS images, they considered the lesions which displayed iso-and synchronous enhancement with surrounding tissue without a clear outline in CEUS images as benign ones and can be downgraded. This different conclusion may be caused by the cases included were sub-centimeter in their study.
What’s more, in our study, 6 cases of benign diseases were over diagnosed in CEUS because of scope expansion, including 3 cases of adenosis and 3 cases of inflammation. This indicated that CEUS has a trend to misdiagnose adenosis or inflammation as carcinomas. This point is consistent with previous study [8]. Notwithstanding, we found that the surrounding vessels in cases of inflammation were straighter than malignant ones, and the perfusion defects were always irregular, multicenter, and non-direction. Because of the smaller sample, we cannot conclude whether there were statistical differences between them and a further research should be conducted.
In summary, CEUS is helpful for us to identify malignant disease and plays a supplementary role in predicting BI-RADS 4 breast disease in some extent. The scope expansion and pathological vessels in CEUS may be the most useful indicators.
Limitations
This study also has some limitations. Firstly, the caseload is relatively small and all cases were from a single hospital, and the pathological subtypes were simple, therefore, the results may be influenced by selection bias. Secondly, we are still lack of experience in reading CEUS images and still has to face the problem of inter-observer agreement. Thirdly, the classification of the CEUS indicators are simple and crude, more reasonable classification is needed to be study. Besides, CEUS has a trend to misdiagnose inflammation or adenosis as carcinomas and may show no evident signs when the tumor was special kind, such as mucinous carcinoma. In summary, whether CEUS can be used as an independent observational modality in breast disease still need to be investigated and more reasonable analysis methods still need to be discussed.