
Abstract
This review focuses on the contribution of abnormal blood rheology in the pathophysiology of sickle cell anemia (SCA). SCA is characterized by a reduction of red blood cell (RBC) deformability but this reduction is very heterogeneous among patients. Recent works have shown that patients with the lowest RBC deformability (measured by ektacytometry) have enhanced hemolysis and would be more prone to develop several complications such as priapism, leg ulcers and glomerulopathy. In contrast, patients with the highest deformability, and not under hydroxyurea therapy, seem to develop more frequently vaso-occlusive like events. Although less studied, RBC aggregation properties are very different between SCA and healthy individuals and it was demonstrated that increased RBC aggregates strength could be involved in some complications. Finally, several studies have established that the vascular system of SCA patients could not fully compensate any increase in blood viscosity because of the loss of vascular reactivity, which may result in vaso-occlusive crises.
Introduction
Sickle cell anemia (SCA) is the most frequent genetic disease in the world. It is characterized by a single nucleotide mutation (adenine ⟶ thymine) in the β-globin gene that leads to the presence of sickle hemoglobin (HbS) resulting from the substitution of valine for glutamic acid at the sixth position of the β-globin chain. When deoxygenated, HbS polymerizes causing a mechanical distortion of red blood cells (RBCs), i.e. sickling. Sickle RBCs are rigid and do not easily flow through the microcirculation, causing frequent vaso-occlusive episodes in affected patients. Recurrent HbS polymerization leads to numerous RBC and systemic physiological abnormalities with variable phenotypic severity [21]. In addition, sickle RBCs are very fragile, which explains the chronic hemolytic anemia observed in SCA patients.
RBC deformability in SCA
Mean RBC deformability (measured by ektacytometry) is decreased in SCA patients at steady state compared to healthy individuals as shown in Fig. 1 [5, 55]. The presence of dehydrated irreversible sickle RBCs (ISCs) in the blood impacts directly on the mean deformability of the whole RBC suspension [6]. Both RBC membrane stiffening and increased internal viscosity are responsible for the lowering of RBC deformability [15, 39]. HbS deoxygenation, as it may occur in post-capillary venules, further causes a reduction in RBC deformability because the formation of polymerized HbS fibers disrupts cell morphology [15]. When re-oxygenated, most of the sickled RBCs unsickle and recover their deformability, although still reduced compared to healthy RBCs.
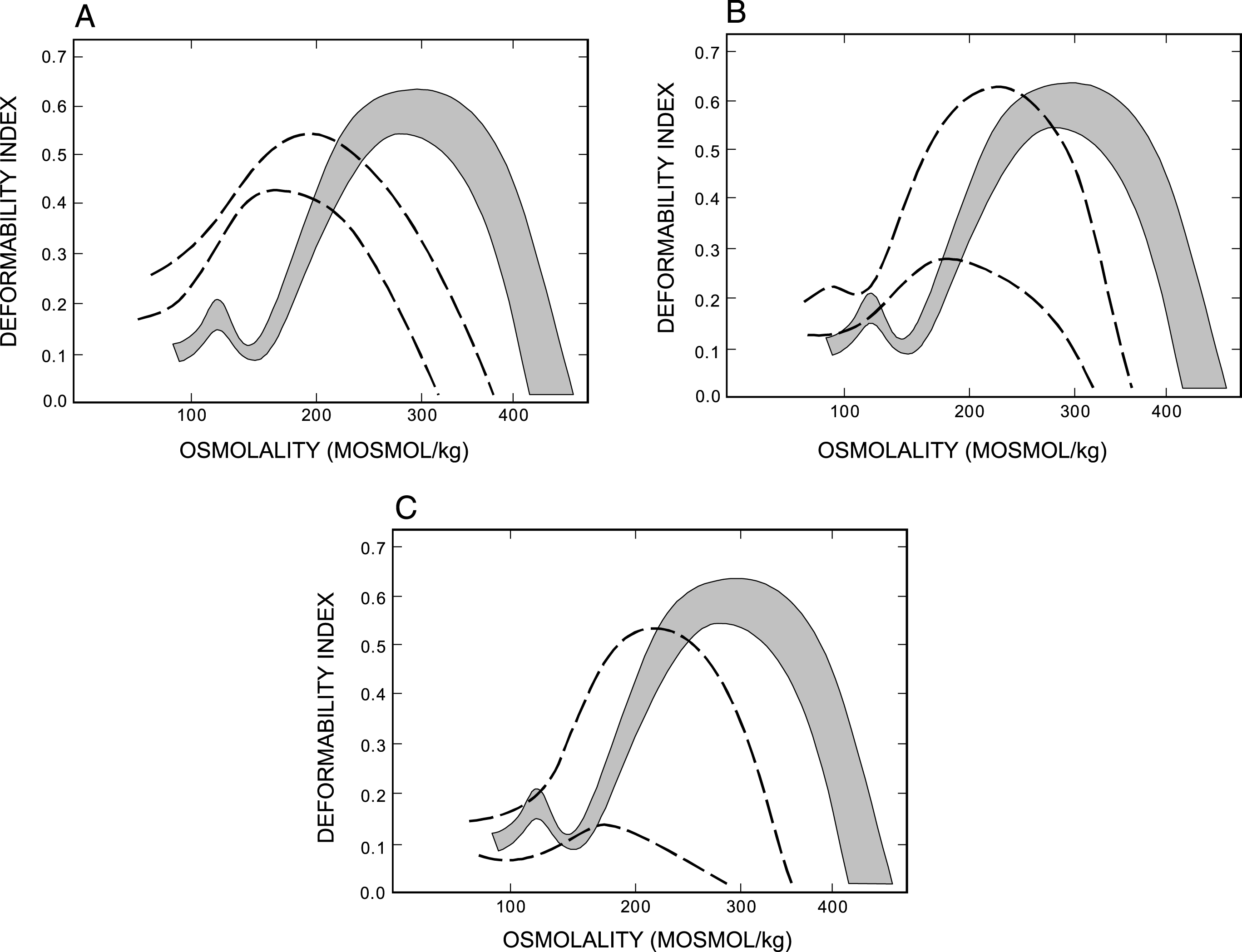
Osmotic deformability profiles for normal control and sickle red blood cells (RBCs). The shaded area represents the range for normal control subjects. (A) The range of 29 determinations from RBCs of six patients with two alpha genes; (B) the range of deformability profiles of 98 determinations from RBCs of 20 patients with three alpha genes; (C) the range of 224 determinations from RBCs of 39 patients with four alpha genes. From [5].
RBC deformability has been extensively studied in the context of SCA. It appears that patients with the so-called hemolytic-endothelial dysfunction phenotype [26] – i.e. leg ulcers [9, 18], frequent priapism [16] or glomerulopathy [30] – have lower RBC deformability than patients without these complications. These findings are in agreement with those of Bartollucci et al. [7] who reported higher number of dense RBCs in patients with these complications. Interestingly, we recently reported a negative association between RBC deformability and several markers of hemolysis [19]. In addition, when exposed to a constant high shear stress (70 Pa) for 30 min, we demonstrated that dense rigid RBCs exhibited a higher decrease in their deformability over time than the less dense RBCs, suggesting that decreased RBC deformability is accompanied by increased RBC fragility [19]. Mixing SCA RBCs (75% ) with healthy deformable RBCs (25% ) decreased the RBC fragility of the whole blood suspension [29]. Indeed, patients with a severe reduction in RBC deformability would be characterized by increased hemolytic rate and marked anemia [19]. Nevertheless, further works are needed to investigate the mechanisms that link reduced RBC deformability and increased RBC fragility in SCA. It is now admitted that hemolysis plays a key role in the pathophysiology of SCA [26] (for further details, see the review of Kim-Shapiro and Gladwin, as well as the review of Usmani and Machado, in this special issue on sickle cell disease published in Clinical Hemorhelogy and Microcirculation). Part of the free hemoglobin released into plasma quickly reacts with haptoglobin and the complex is cleared from plasma. However, this system is insufficient to eliminate the excess of free circulating hemoglobin in SCA and a large amount reacts with nitric oxide (NO) to produce methemoglobin and nitrate ultimately leading to reduced NO bioavailability [26]. In addition, the release of RBC arginase into the plasma catabolizes plasma arginine and thus reduces its bioavailability. Furthermore, heme and heme-iron dissociate from Hb and contribute to the production of reactive oxygen species (ROS) that serve as potent NO scavengers [26]. The decline in blood NO and the increase in blood heme content leads to endothelial dysfunction, over-expression of vascular adhesion molecules and impaired vasomotor tone [8, 40]. In support of these mechanisms, plasma from patients with SCA contains cell-free ferrous oxyhemoglobin, which stoichiometrically consumes micromolar quantities of NO and abrogates forearm blood flow response to NO donor infusion [50]. In summary, it seems that a link exists between reduced RBC deformability, increased hemolysis and the development of chronic vasculopathy in SCA [17].
RBC deformability and vaso-occlusive events
In contrast, it has been demonstrated that although an increase of RBC deformability is beneficial for blood flow (because of the reduction of blood viscosity for instance) and tissue perfusion (because deformable RBC can easily negotiate small capillaries) in the healthy population, SCA patients with the highest RBC deformability would be prone to osteonecrosis [37] and frequent acute painful vaso-occlusive crises (VOC) [31–32]. The increased risk of SCA patients with alpha-thalassemia to develop more frequently VOC, compared to those without, has been attributed to the effects of alpha-thalassemia on RBC deformability [51]. While RBC deformability is decreased during vaso-occlusive events, Ballas et al. [6] demonstrated that high level of RBC deformability during the recovery phase of a painful vaso-occlusive event (Fig. 2) was a predictor of a new painful crisis. Lande et al. [32] reported a significant and positive correlation between the incidence of painful crisis in SCA and RBC deformability, as initially reported by Ballas et al. [3, 5]. This surprising finding may be explained by the fact that sickle RBCs with the highest deformability are also the most adherent RBCs to the vascular wall, thus decreasing the lumen of microvessels, slowing blood flow and initiating vascular occlusion [5, 44]. The increased adhesiveness of sickle RBCs with the highest deformability would be explained by the fact that they could spread their adhesive patch to a greater extent than the more rigid sickle RBCs [44]. In contrast, although hydroxyurea therapy improves RBC deformability in SCA patients [34, 38], it decreases the frequency of VOC-like events [12]. These apparently contradictory data could be explained by the fact that hydroxyurea treatment also increases fetal hemoglobin level (thus decreasing the proportion of HbS and its propensity to polymerize [60]), decreases platelet and leucocyte counts [60], reduces the adhesiveness of sickle RBCs, as well as of white blood cells, to the endothelium [20, 60], decreases oxidative stress [54, 58] decreases the expression of phophatidylserine at the surface of circulating microparticles [22] and could increase the level of circulating nitric oxide [45].

Changes in the percentage of dense red blood cells (RBC) and in the osmotic gradient deformability profile of sickle cell anemia RBC at various times during the evolution of the vaso-occlusive crisis (VOC). The number of each curve represents the VOC day on which the profile was determined. Changes in the percentage of dense RBC are indicated in the left upper corner. The shaded area represents the range for normal control subjects. The deformability profile was determined sequentially in the steady state (S) and on days 5 and 13 of the VOC. From [4] with permission.
RBC aggregation properties have been poorly studied in SCA but several studies reported that RBC aggregation (which depends on the number of RBC aggregates and time for RBC aggregates formation) is rather decreased in SCA patients compared to healthy individuals. The lower RBC aggregation seems to be due to the low ability of the rigid ISCs to form aggregates [14, 19]. Deoxygenating sickle cell blood in vitro results in a further decrease of RBC deformability and RBC aggregation [10]. However, patients with increased RBC aggregation seems to be prone to frequent VOC-like events [35, 51]. While RBC aggregation is rather decreased in SCA, once formed, sickle RBC aggregates are 2 to 3 fold more robust than healthy RBC aggregates [52, 59]. Chronic enhanced oxidative stress has been reported to strongly modulate the strength of RBC aggregates [25]. The findings of Loiseau et al. [41] suggest that these sticky RBC aggregates would preferentially deposit at bifurcation level in vascular networks, which could increase the risks for VOC-like events. Indeed, Lamarre et al. [31] found an association between RBC aggregates strength and acute chest syndrome (ACS) in SCA. To date, no study measured the RBC aggregation changes during a VOC event in SCA and only limited data are available on erythrocyte sedimentation rate, a parameter that is affected by both hematocrit and RBC aggregation [2, 33]. The increase of fibrinogen during VOC could promote RBC aggregation [2] but further studies are needed to directly investigate this parameter during crisis.
Blood viscosity in SCA
Owing to the chronic severe anemia, SCA patients have lower blood viscosity at native hematocrit under oxygenated conditions than individuals with normal hemoglobin [55]. However, blood viscosity would increase with ageing in SCA patients [52], which could explain at least partly why osteonecrosis and retinopathy prevalence increase with age in this population [36]. When adjusted to a normal hematocrit level in-vitro (40–45% ), blood viscosity of SCA patients is above the controls under oxygenated conditions (partly due to the presence of ISCs). When deoxygenated, the sickling of RBCs causes a further rise in blood viscosity at all shear rates [15].
Classically, it is suspected that any increase in blood viscosity could be deleterious for the cardiovascular system. However, a rise in blood viscosity is pretty well tolerated in the general and healthy population [53]. The production of NO by the endothelial NO-synthase is strongly dependent on the shear stress applied on the vascular wall. Shear stress is the product of shear rate by blood viscosity. Indeed, when blood viscosity increases, endothelial cells produce more NO, which results in compensatory vasodilation that normalizes vascular resistance and blood flow [56, 57]. However, in case of endothelial/vascular dysfunction, like in SCA [1, 49], a rise in blood viscosity could not be fully compensated and is suspected to impair blood flow [13].
A large epidemiological study conducted in the United States (the Cooperative Study of Sickle Cell Disease) demonstrated that high hematocrit and Hb increased the risks for VOC [48] and ACS [11], respectively. This is in agreement with previous findings showing that Hb value is an independent predictor for the development of acute pain crisis in SCA [32]. Hematocrit is a key determinant of blood viscosity, particularly at low shear rate where the rise in viscosity is exponential. Indeed, it is not surprising to observe that SCA patients with more frequent hospital admissions for VOC have higher blood viscosity at steady state than patients with less frequent hospitalizations [31, 51]. Moreover, blood viscosity was shown to rise further during a VOC, which may worsen tissue perfusion and oxygenation [2].
Conclusion
Progress has been made in the last decades in the understanding of the pathophysiological mechanisms involved in SCA. Previous and recent studies identified several potential biomarkers and hemorheological predictors of various acute and chronic complications that paved the way for stimulating novel approaches to develop appropriate therapies. In addition, further studies are needed to better understand the relationships between RBC rheological properties, RBC fragility (i.e., hemolysis) and RBC adhesiveness in the context of SCA.