
Abstract
BACKGROUND:
Chronic venous disease (CVD) is extremely common worldwide. The prevalence is increasing with age and is associated with a reduced quality of life, particularly in relation to pain, physical function and mobility. Symptomatic chronic venous insufficiency (CVI) with venous ulcer at its’ endpoint, indicates interventional surgery to cure venous reflux therewith promoting wound healing and preventing recurrence. To our knowledge up to now no coherent study has been undertaken in patients with CVI who underwent an open venous surgery concerning complications, venous hemodynamics and perioperative symptomology in one study population. This was undertaken in our retrospective, single-centre, consecutive case-control study in a single patient population of a university clinic in northern Germany. Part I covers postoperative complications in relation with co-morbidities, co-medication and clinical presentation. Part II will focus on pre- and postoperative hemodynamics and evolution of symptoms.
METHODS:
Records of n = 429 (467 extremities) patients from 2009–2013 treated with open surgery were analysed. Number and type of complication were evaluated with regards to demographic parameters, co-existing medical conditions and procedure related aspects. Complications were grouped as no events (NE), neglectable adverse events (NAE), non-neglectable adverse events (NNAE) and severe (life-threatening) adverse events (SAE).
RESULTS:
In 467 extremities of 429 patients with CVI 130 (27,84%) postoperative complications were observed after open surgery, thereof 64 (13,7%) NAE, 66 (14,14%) NNAE and 0 SAE. 29 (6,76%) patients developed a postoperative surgical site infection, thereof 4 (0,9%) with consecutive septicaemia. Except one case with nerval lesion and paraesthesia and hypoesthesia not resolving after 12 months all complications resolved within surveillance time span of 12 months. Patients developing NAE had a higher BMI (p = 0.003), were more likely to have diabetes mellitus (p < 0.001), and co-morbidities leading to the intake of anti-platelet or anticoagulation drugs (p < 0.001). Metabolic syndrome (p < 0.001) and anti-platelet or anticoagulation (p < 0.001) could be defined as independent risk factors for the development of complications. Patients receiving open surgery of small saphenous veins had 8 times higher risk of calf muscle venous thrombosis (p = 0.001).
CONCLUSION:
Patients with a metabolic syndrome or receiving anti-platelet therapy or anticoagulation medication should undergo open venous surgery under hospital conditions with routine postinterventional surveillance visits. Patients undergoing an open surgery of SSV are definite candidates for postoperative subcutaneous heparin thromboprophylaxis. In general stripping below knee increases the risk of postoperative sensory deficit. This resolves in almost all patients within one year.
Keywords
Background
Chronic venous disease (CVD) is along with arterial hypertension [1], cardiovascular disease [2] and obesity [3, 4] a wide spread disease entity in general population [5, 6]. Not only elder epidemiological studies like the Basel Vein Study [7] and Edinburgh Vein Study [8] but also the recent international observational study, the Vein Consult program, revealed a high prevalence of chronic venous disease in general [9]. Not surprisingly, this poses a high socioeconomic burden. It has been estimated that venous ulcers cause the loss of approximately 2 million working days with treatment costs of approximately 3 billion US-dollars per year in America [10]. Overall, CVD has been estimated to account for 1 to 3 percent of total health care budgets in countries with developed health care [11]. Although the classical fast ligation and stripping is already in practice for more than 100 [12] years and apart from eye-operations one of the oldest operations performed by mankind [13, 14], valid study references are rare. There is no study as holistic approach available, examining complications of open surgery in CVI patients including investigations of venous hemodynamics and evolution of symptoms in one patient population. Some studies access the clinical outcome [15–17], others the recurrence rate [18–20] or complication rates [21–25], separately. The situation is worsened by the fact that neither for the recently introduced minimally invasive techniques in Phlebology like laser ablation such data are referenced. This is in contrast with ongoing modern demands for strong quality assessment to ensure patients' safety and satisfaction. Although catheter-based venous interventions can theoretically be used in every patient with adequate venous anatomy there are always patients who benefit more from the classic-operative procedure. Hence, the aim of this study was to depict the complications with regards to the influence of risk factors, as well as to evaluate the postoperative haemodynamic and evolution of symptoms, finally, to deduce possible risk factors and corresponding prevention strategies in clinical practice in the future.
Material and methods
Material
429 patients (n = 467 lower extremities) who had undergone venous surgery from 01.01.2009 to 31.12.2013 at the dermatological University Department in Greifswald, northern Germany, aged 18 and above were included in our retrospective consecutive case-control study. All kind of surgical intervention types were analysed, most operations (n = 327) were stripping of the vena saphena magna and parva. Less frequently (n = 140) miniphlebectomy and ligation of perforating veins was performed. There were no exclusion criteria defined for this study. The study was performed in agreement with the ethical guidelines of Clinical Hemorheology and Microcirculation [26].
Methods
Before study initiation a positive ethics’ vote (No: BB 121/15) - in conformity with the Helsinki Declaration - was obtained by the Institutional Review Board of our university hospital in Greifswald, Germany.
The study population was selected from our clinical database, searching for all patients who had undergone a surgical procedure due to CVD (ICD: I83.0, I83.1, I87.2, I83.9). In total 666 patients with 686 venous surgical procedures were extracted. Patients only receiving surgical ulcer debridement were excluded. The routine follow-up period with regards to postoperative outcome was one year (follow-up visits: 1-day post-op, 10-days post-op, 6-weeks post-op, 1-year post-op) (Fig. 1).
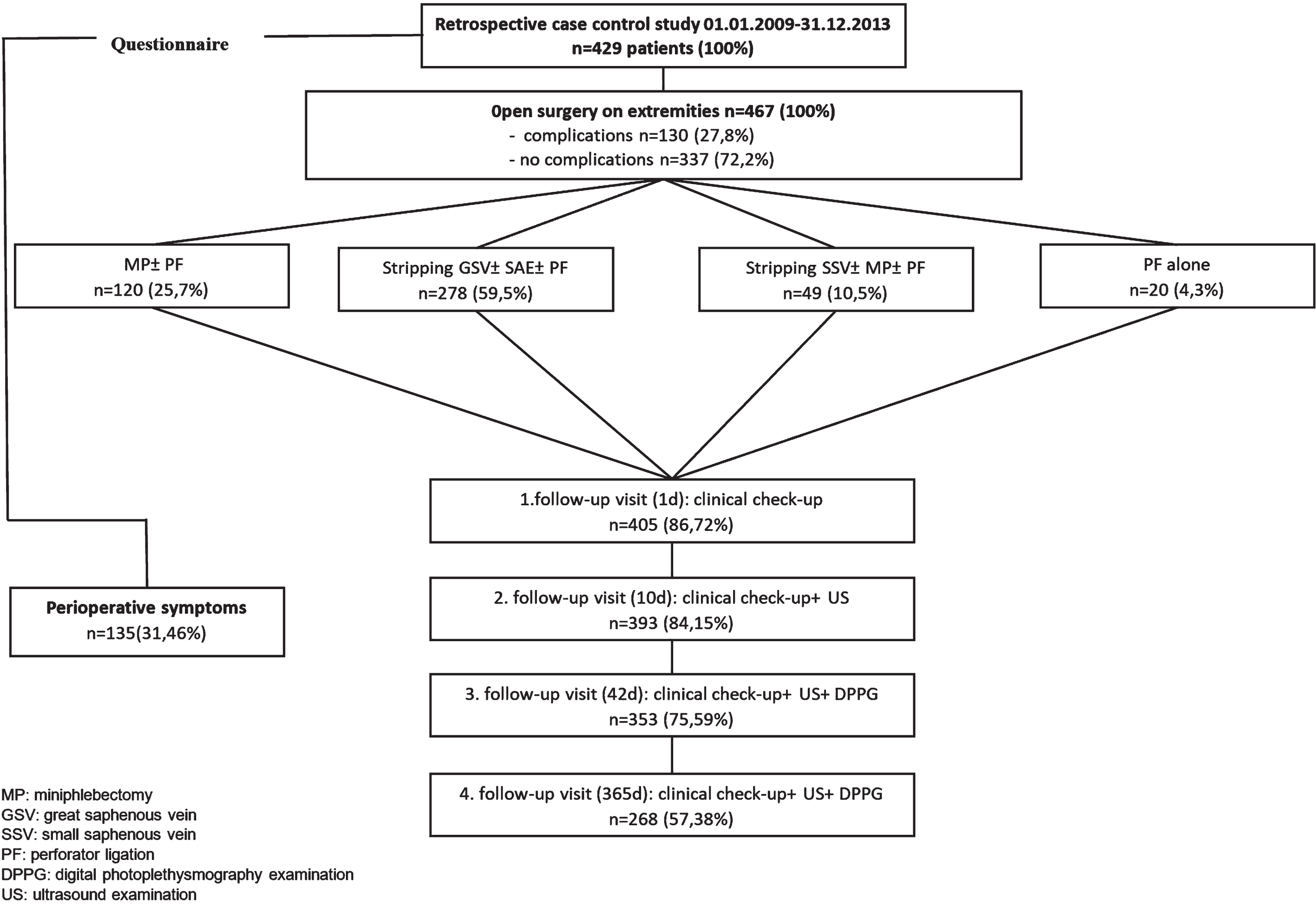
Study design. In total 429 patients (467 extremities) were included in this retrospective study. In 130 extremities postoperative complications could be detected. 20 extremities received a ligation of a perforating vein. 120 extremities were treated with a miniphlebectomy, 278 and 49 extremities received a fast ligation and stripping of the great saphenous vein or small saphenous vein respectively. Over a postoperative period of one year every patient received regular follow-ups (1d post-op 405 extremities, 10 days post-op 393 extremities, 6 weeks post-operative 353 extremities and one year post-operative 268 extremities were visited). Every patient received an additional questionnaire conering CVI related symptoms (preoperatively, postoperatively and later in time), results will be presented in Part II. Abbreviations: MP: miniphlebectomy; GSV: great saphenous vein; SSV: small saphenous vein; PF: perforator ligation; DPPG: digital photoplethysmography examination; US: ultrasound examination.
For assessment of CVI specific symptoms a questionnaire was send to the patients surveying pre- and postoperative symptoms and their evolution over the course of treatment. During routine follow-ups venous function was evaluated in intervals shown in section pre- and postoperative diagnostics. The above-mentioned symptomology and hemodynamics will be covered in a separate, future publication.
Clinical assessment preoperatively and to every follow-up visit included anamnestic and clinical evaluation of the operated limb, in accordance to the CEAP-Classification. Preoperatively, every patient received a duplex-ultrasound examination of the lower extremity veins. In the case of the GSV and SSV the insufficiency level was additionally graded according to the Hach-Classification. An additional venous function test with digital photoplethysmography (D-PPG), objectively evaluating the venous function with measures of passive venous refill time and active venous outflow, was performed. Postoperatively, a duplex ultrasound examination was performed at 10-days-, 6-week- and one year follow-up. Venous function changes were objectified with D-PPG at 6-week-, and one year follow-up.
Operative technique
Stripping of the great saphenous vein (GSV) and small saphenous vein (SSV)
Before surgery, the relevant venous complex to be operated was marked under guidance of duplex-sonography. The operation started with a 2–3 cm long, oblique incision in the groin or popliteal crease, exposing the femoral/popliteal vein and saphenofemoral/saphenopopliteal junction (SFJ/SPJ). The GSV/SSV was flush ligated with nonabsorbable sutures close to SFJ/SPJ. Additionally, all tributaries were ligated and dissected and the endothelium at the dissection-point coagulated to minimize recurrence. Hereupon, the stripping wire was led through the saphenous vein and with a counter-incision attached to the stripper head (olive) at the distal point of insufficiency. If needed, an additional miniphlebectomy of buldging side branches and ligation of perforating veins (as explained below) was performed. Finally, the great or small saphenous trunk was stripped from the distal insufficiency point to the proximal point of insufficiency with the purpose of abolishing reflux in the superficial venous system.
Miniphlebectomy and perforator ligation
Miniphlebectomy with additional ligation of perforating veins was performed as an individual procedure or in combination with the stripping operation. The insufficient side branches were treated with 3–4 mm stab incisions along the vein. The vein was then extracted by Varady hooks and ligated. The ligature of the previously ultrasound marked perforating vein was performed by a 2–3 cm long incision. Hereafter the perforating vein and all tributaries were dissected and ligated.
Intra- and postoperative management
Intraoperatively, compression bandages were applied to the extremity from foot to groin for a stripping operation of the great saphenous vein. In case of an operative procedure at the lower leg compression bandages were applied till knee. The compression therapy was maintained for at least six weeks (8 h/day) with compression stockings. Additionally, patients received a subcutaneous thromboprophylaxsis with low molecular heparin (2500 IU) for ten days.
Classification of adverse events
The patient population was subdivided into four groups no events (NE), neglectable adverse events (NAE), non-neglectable adverse events (NNAE) and serious adverse events (SAE). The different categories were defined as follows: no events: open venous surgery without postoperative complications neglectable adverse events: complications without any necessity to intervene, complete or partial symptom resolvement after time relapse non-neglectable adverse events: complications with necessity to intervene (outpatient treatment vs. inpatient treatment) serious adverse events: life-threatening intraoperative or postoperative complications.
Statistical analysis
Clinical data from medical records (age, gender, side diagnosis, clinical classification of CVD) were analysed with the software R 3.5.0 and R Studio (Open source Licence) and were deemed significant for p < 0.05. In general, three separate bivariate analysis were undertaken for the subpopulations (no events, neglectable adverse events, non-neglectable adverse events). Normality was checked with Shapiro-Wilks test. Comparisons were performed using the chi-square test or Fischer’s test, respectively. Wilcox-test and Kruskal-test as appropriate were used for categorical variables and t-test and ANOVA for continuous variables. Generalized regression modelling with error distribution binomial (known as logistic regression) or Poisson was performed to access history of DVT for recurrence of thrombotic events, procedure related aspects, patient demographics, co-morbidities and medication. A regression subset selection was undertaken before to find best models (BIC-criteria) with the r-package leaps since the mentioned number of variables was too large. As descriptive statistics we used mean, SD, Min.- Max., Median and as Graphics Boxplots and Line diagrams.
Results
General characteristics
In total 429 patients (n = 467 lower extremities) were included in this statistical analysis. The mean age in our patient population was 56,2, SD±11,9 (min. 21 years; max. 83 years) with a mean body mass index (BMI) of 28,7 kg/m2, SD±6,33 kg/m2 (min. 17,2; max. 65,5). The gender distribution was higher for female than male population (female n = 289 (67,3%) vs. male = 140 (32,7%)). In total 359 (76,87%) operations were performed in general anaesthesia, 20 (4,28%) in spinal anaesthesia and 88 (18,84%) extremities were treated in local (tumescent) anaesthesia (miniphlebectomy and perforator ligation). In total 278 (59,53%) extremities presented preoperatively without any signs of trophic skin changes of the treated limb (<C4-CEAP classification). In contrast 189 (40,47%) presented with clinical signs of venous insufficiency related skin changes, hence ≥C4-CEAP classification. Of this subgroup 43 (9,21%) extremities had an active venous ulceration preoperatively and 10 (2,14%) had a healed venous ulcer. Concerning relevant side diagnosis medical records revealed diabetes mellitus (n = 35, 8,15%), metabolic syndrome (n = 18, 4,19%), obesity (n = 97, 22,61%), coronary heart disease (n = 22, 5,13%), atrial fibrillation (n = 12, 2,8%) and history of thrombotic events (n = 39, 9,1%) in the patient cohort.
Complications
All operative procedures were performed under the care of one surgeon, who performed 96,2% of all the operations and was present in every single one of them.
Overall, in 130 of 467 (27,84%) open surgeries postoperative complications could be registered. Of these 64 showed neglectable and 66 non-neglectable adverse events. No patient suffered from serious adverse events.
Neglectable adverse events (NAE)
Five patients complained about postoperative hyperpigmentation along the treated vein, six had prolonged pain either at the level of incision or along the stripped vein. In 12 limbs painful hematoma of approx. 20× 10 cm could be detected. 6 patients had a superficial site infection treatable with local ointments and antiseptic therapy and three patients showed wound healing delays without signs of infection. In 22 limbs a postoperative paraesthesia was found which resolved completely after one year in every patient. 10 patients had a diverse set of complications (n = 3 type IV allergy to stockings/ skin marker/ plaster, n = 2 toxic dermatitis due to antiseptic, n = 2 postoperative nausea and vomiting, n = 1 heparin induced thrombocytopenia, n = 2 suture granuloma).
Non-neglectable adverse events (NNAE)
One patient suffered from an intraoperative nerve damage with lasting sensory deficit even after one year. Postoperative thrombotic events were diagnosed in 31 limbs. In total, 23 patients developed a surgical site infection with the necessity of antibiotic therapy. In total 7 patients had to be treated due to postoperative bleeding complications. 4 patients had a perfuse postoperative bleeding making a reintervention necessary and 2 patients developed an extensive postoperative hematoma making a surgical removal necessary. One patient received due to a hemodynamic relevant bleeding erythrocyte concentrates postoperatively. In total 4 patients developed a lymphatic complication (n = 2 lyphoedema of the lower extremity; n = 2 lymphatic fistula at the tigh) three of these patients underwent exploration at the groin due to recurrent varices and were treated with compression therapy or ligation of the fistula respectively.
Patients with non-neglectable adverse events had a higher BMI (p = 0.003) and a more severe clinical presentation of CVI in comparison to the other two groups (trophic skin changes = C≥4: no events 35,81%; neglectable adverse events 46,88%; non-neglectable adverse events 65,15% : p < 0.001; 95% CI:1.84–9.92; OR:4.122. Venous ulceration = C6: no events 7,71%; neglectable adverse events 3,31%; non-neglectable adverse events 22,72% : p < 0.001; 95% CI: 2,39–14,13; OR:5,95). Concerning the side diagnosis diabetes (p = 0.001), metabolic syndrome (p = 0.001), Coronary heart disease (p = 0.001), atrial fibrillation (p = 0.001) and in general a higher ASA category (p = 0.016) was also overrepresented in this subgroup.
Postoperative thrombotic events
In 31 (6,63%) limbs an iatrogenic venous thrombosis was registered. None of the patient developed a pulmonary embolism. In 11 (2,35%) lower extremities a thrombophlebitis of a side branch of the epifascial venous system occurred, one (0,21%) being at the saphenofemoral junction point. Duplex-sonography during the follow-up visits revealed a deep vein thrombosis of the lower leg in 20 (4,28%) patients, 16 (3,43%) presenting as calf muscle venous thrombosis. Patients undergoing a phlebectomy of the small saphenous revealed an increased risk of calf muscle venous thrombosis (OR 8,56, 95% CI 2,72–26,51; p = 0.0001) (Fig. 2). One patient developed a thrombophlebitis as well as a deep venous thrombosis of the lower extremity after a single operation at the affected extremity and was therefore counted to the subgroup of deep vein thrombosis as this represents the severer postoperative complication.
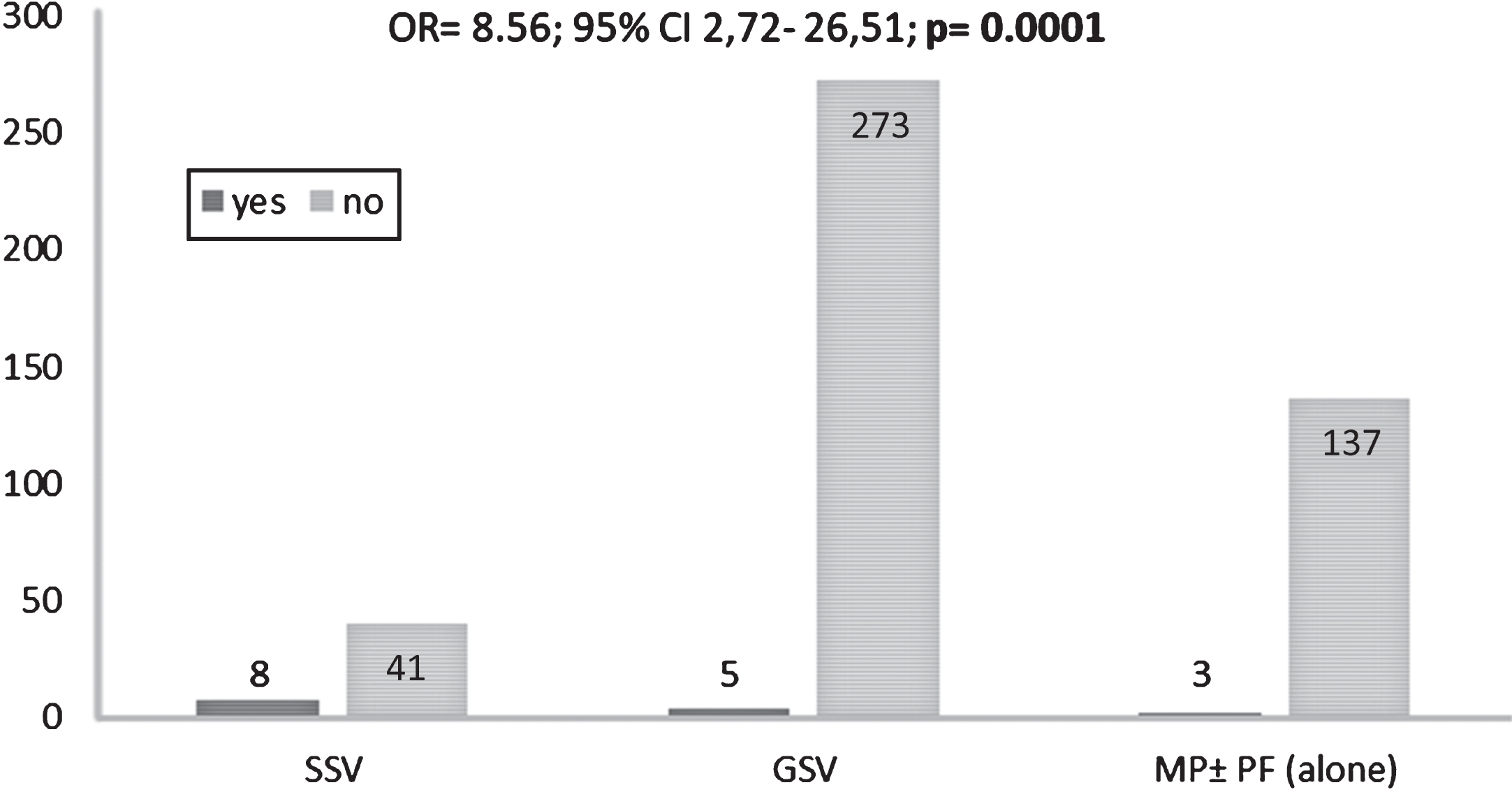
Incidence of calf muscle venous thrombosis after open surgery of vena saphena parva vs. vena saphena magna and miniphlebctomy. Patients receiving a fast ligation and stripping of the small saphenous vein have a higher risk of developing a claf muscle venous thrombosis (16,32%) in Comparison to patients receiving a stripping of the great saphenous vein (1,79%) or a Miniphlebectomy with or without perforator ligation (1,5%) (OR:8.56; 95% CI 2.72–26,51; p = 0.0001). Abbreviations: SSV: small saphenous vein; GSV: great saphenous vein; MF±PF: miniphlebectomy with or without Perforator ligation.
There was one case of intraoperative n. suralis damage. This patient suffered no motor deficit but had a sensory deficit presenting as paraesthesia and hypoesthesia of the toes which was still present at one-year follow-up. Another patient suffered from a sensory deficit at the upper thigh (miniphlebectomy of the anterior accessory great saphenous vein). Other nervous complications presented as sensory deficits at the distal leg or foot. In general, there was a significant association of developing postoperative paraesthesia with a higher ultrasonographic Hach grade (p = 0.002) (Fig. 3). According to the operation documentation in the case of the GSV and SSV the veins were stripped till the distal insufficiency points.
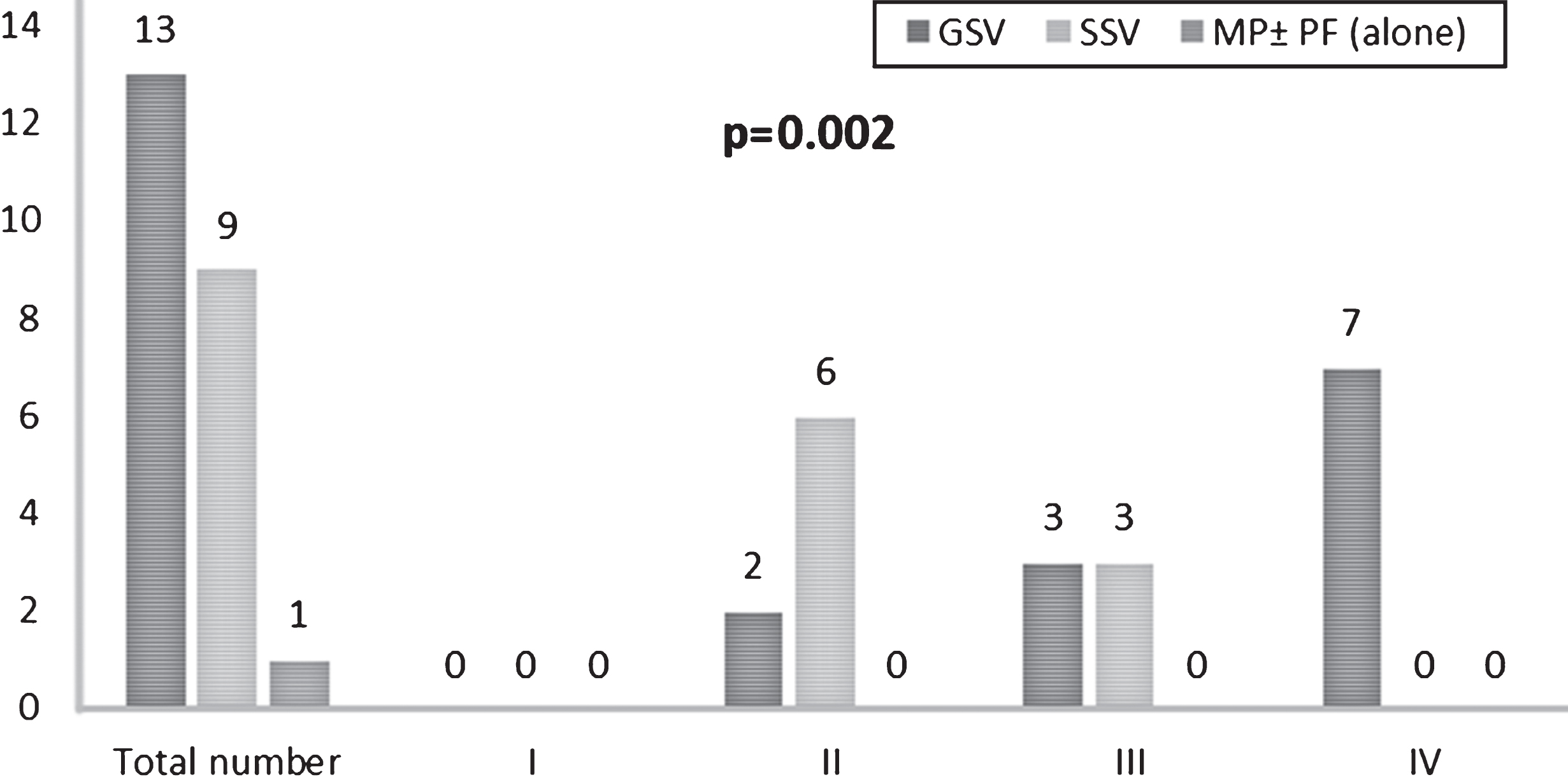
Incidence of Paraesthesia after open surgery in relation with Hach-Classification. Regardless of the stripped vein (GSV or SSV) the incidence of postoperative sensory deficit increases with a stripping below the knee (GSV from Hach III and SSV from Hach II) p = 0.002. Abbreviations: GSV: great saphenous vein; SSV: small saphenous vein; MP±PF: miniphlebectomy with or without Perforator ligation.
Eight (1,86%) patients developed superficial and 21 (4,89%) deep surgical site infections (according to CDC-definition of surgical site infections (SSI)). Thereof, 4 (0.93%) patients developed a consecutive septicaemia and 3 (0,69%) patients had a wound healing delay with dehiscence at the suture site without local signs of infection. The length of hospital stay was influenced by the severity of infection (median 2 days hospital stay in superficial surgical site infections vs. 10 days in deep surgical site infections and 17 days in septicaemia p < 0.001). In general, demographic factors (higher age p = 0.02) predisposing conditions (BMI; p < 0.001; D.m. type II, metabolic syndrome, coagulation/anti-platelet medication p < 0.001 and presence of venous ulceration, p < 0.001) as well as procedure related factors (longer operation time; p < 0.001) had a significant influence on the development of surgical site infections. Interestingly, these factors did not alter significantly the severity of surgical site infections (p > 0.05).
Extended hospital stay
In total 33 (7,06%) patients had an extended stay more than two days due to postoperative complications (haemostesiological complications, lymphatic complications and SSI) 5 patients (1,17%) were readmitted due to postoperative complications. Patients with three or more days of hospital stay were in general older (p = 0.007) and had a higher BMI (p < 0.001). The number of patients with diabetes (p < 0.001) and metabolic syndrome (p < 0.001) was also higher.
Discussion
The main objective of this study was to evaluate postoperative complications in CVI patients and the hemodynamic effects of therapy along with perioperative CVI specfic symptomology. We analysed 429 patients (467 extremities) with regards to complication development in junction with the influence of extrinsic and intrinsic predisposing factors. Venous disease therapy patterns appear to have shifted in the past decade in favour of minimally invasive procedures, leaving the classical open surgery in a defensive position [18]. Therefore, it is of utmost importance to evaluate the quality of this procedure with regards to complication development, hemodynamic effects and perioperative symptomology. The last two dimensions of post-operative outcome will be covered in a commencing publication. In contrast to other studies, we defined 3 complication groups, including every type and severity of complication, leading to an overall complication rate of 27,84%. At first this number seems oddly high, but one must bear in mind that up to now studies just evaluated certain aspects of complications [22, 27–31].
Thus, to be able to put the complications in the general context of complications reported so far by others, important ones will be discussed individually.
Concerning thrombotic events, a total of 20 patients developed a postoperative deep venous thrombosis and 11 a thrombophlebitis. One patient was admitted based on clinical suspicion of lung embolus, which could be ruled out by computer tomography. Our incidence of DVT with 4,28% is comparable with van Rij et al. stating the incidence of DVT with 5,3% with no resulting lung emboli. The incidence of calf vein thrombosis is also comparable [32]. Interestingly, 32,26% (n = 10) of our patients developing a postoperative thrombosis had a positive history of thrombotic event is the past. Though statistically not significant it is in accordance with the findings of Hofer et al. that thrombotic events are often caused by an underlying coagulation disorder predisposing to its development [33]. Unfortunately, in our patients developing a postoperative thrombotic event no testing for coagulation disorders was performed. Patients undergoing a flush ligation and stripping of the small saphenous vein are known to be prone to developing a calf muscle venous thrombosis [26], patients in our cohort undergoing an open surgery of the SSV had eight times higher risk for developing a calf vein thrombosis. This finding stands to logic as it is known in literature that 32% of gastrocnemius muscle veins share a common junction place with the small saphenous vein entering vena poplitea [26]. In these patient cases the operative procedure itself rather than the underlying haemostesiological factors are to be seen as a predisposing factor [26].
Comparison of patient subgroups (no events, neglectable adverse events, non-neglectable adverse events) with regards to distribution of demographic factors, comorbidities, clinical classification, postoperative complications and their statistical significance
Comparison of patient subgroups (no events, neglectable adverse events, non-neglectable adverse events) with regards to distribution of demographic factors, comorbidities, clinical classification, postoperative complications and their statistical significance
Abbreviations: BMI: body mass index; SD: Standard deviation; ASA: American Society of Anesthesiology; CEAP- C-Clinical, E- Ethiological, A- Anatomical, P- Pathological- Classification (Phlebology); sSSI: superficial surgical site infections; dSSI: deep surgical site infetions.
Our findings that stripping below the knee increases the incidence of paraesthesia is in concordance with other studies [31, 35]. This is due to the fact that the saphenous vein proximates the nerves progressing distally [31]. On one side, the incidence of nerve injury decreases from 23% –40% to 5%, when selective preservation of the saphenous vein is performed [36], on the other side, leaving a higher risk of recurrence [31]. According to Sorrentio et al. the shift to the technique of invaginated stripping reduces the incidence of nerve injury to 1,5% [37]. Cicek et al. suggest the stripping above knee with a big olive head and below knee with a small olive head, leading to a reduction of nerve injury [31]. Though it is an unpleasant complication our findings as well as other studies show that symptoms of sensory nerve damage disappear after one year without medical interference [38], if no major nerve was damaged intraoperatively.
Under physiological conditions skin poses a natural barrier to potential pathogens. With a surgical incision this protective barrier is interrupted, predisposing to surgical site infections. The risk of its development is influenced by the preoperative wound condition [39]. According to the surgical wound classification incisional wounds in phlebosurgery can be classified as clean wounds, with an overall risk of SSI of <5% without antibiotic prophylaxis [39]. Not only the wound condition itself but also several extrinsic and intrinsic factors influence the development and severity of surgical site infections.
The main influencing extrinsic factor is the total duration of operative procedure. According to Cruse and associates a doubling risk for SSI for every commencing hour of procedure can be expected [40].This is also seen in our cohort as patients developing a SSI had in average a 30 minutes longer operation time (SSI: Mean 128,39; SD±35,43 vs. no SSI: 96,81 SD±32,26; p < 0.001). The experience of the surgeon has also been shown to influence the incidence of SSI [41], this risk factor can be excluded in our patient population as 96,2% where performed by one experienced general surgeon, being present in every single one of the operations.
It is well known that certain intrinsic factors increase the risk of postoperative complications, especially SSIs. Studies undertaken in patients with skin surgeries state diabetes as an independent risk for SSIs [41–43]. This is in concordance with our findings that patients developing SSI are more likely to have an underlying diabetes. Several studies [43–46] depicted along with our results the negative effects of obesity on the development of postoperative complications, especially SSI (NE BMI 28 kg/m2 vs. NNAE BMI 32 kg/m2; p = 0.003). Carruthers and co-workers could show 2.16 times higher odds for superficial surgical site infections in patients with a higher BMI in their comparative study [44]. The increased odds of developing a SSI with underlying obesity has also been shown in the same manner by other studies in vascular surgical procedures [45–47].
As hematoma is a good breeding ground for bacteria we were not surprised that patients taking antiplatelet or anticoagulative medication showed higher risk of surgical site infections (p < 0.001), though being treated at a mean INR of 1,01. This is in accordance with Heal et al. [42].
Patients with advanced CVI related skin trophic changes (lipodermatosclerosis, white atrophy or venous ulcer) have shown to be more likely to develop NNAEs like SSIs (p < 0.001; 95% CI:1.84–9.92; OR:4.122). Under physiological conditions skin cells, including keratinocytes and mast cells, secrete peptides (e.g. Cathelicidin, β-defensin-2) [47–50] and sweat glands enzymes (lysoenzymes) with antimicrobial activities [49]. Additionally, the high salt content, partly caused by sweat evaporation has also antimicrobial properties [48]. Long standing venous and capillary hypertension leads to decreased skin barrier function and dryness caused by increased transdermal water-loss. Though not examined in CVI patients there are studies in atopic dermatitis patients with known skin barrier dysfunction and a dry skin which showed decreased Cathelicidin and β-definsin-2 levels [50]. The altered skin architecture and disrupted skin function probably leads to an overgrowth of opportunistic microbial agents which may spread over the whole extremity predisposing for postoperative wound infections. This is in line with Carruthers et al. depicting a higher incidence of postoperative surgical site infections in patients with venous ulcerations [44].
Keeping the above-mentioned risk factors in mind, our findings are only consistent that metabolic syndrome (p = 0.007), antiplatelet and/or anticoagulative medications (p = 0.0001) as well as severe clinical presentation of CVI (p = 0.0016) are independent risk factors for the development of complications.
Any retrospective study assessing outcomes after interventions is open to criticism in general as minor complications may be underrepresented. This may also be influenced by the fact that not all patients present to the department where the operation had been performed when a complication develops. The inter- observer variability in clinical assessment and documentation must be mentioned in this context as well. Further limitation is the small patient population which is prone to statistical errors in accessing complications especially regarding Type II errors. Other limitations of the study are the monocentric design as well as the fact that only 57% of the patient population completed follow-up.
Conclusion
In general, obese patient with concomitant diabetes, metabolic syndrome or diseases leading to the intake of antiplatelet and/or anticoagulation medication (CVD, AF) are more prone to developing non-neglectable severe events leading to a rehospitalisation or prolonged hospital stay. In consequence, these patients should receive an inpatient surgical treatment with regular follow up as this is not the mainstay postoperative management nowadays. We could prove that open surgery and stripping of the small saphenous vein increases the odds of developing a calf muscle venous thrombosis. Though recurrence of a thrombotic event with a positive medical history is statistically not significant, we saw a higher incidence of thrombotic events in these patients, which has also been proven in past studies. Therefore, patients undergoing a stripping of the small saphenous vein or patients having a positive history of a past thrombotic event should receive a subcutaneous heparin prophylaxis postoperatively. As open surgery poses a relative risk of complication development in every patient, surgery should more so be performed with some postoperative precautions in patients at risk.
Conflict of interest
None.
Funding
None.