
Abstract

Introduction
Rotationplasty is a limb-salvage surgery which has been used as an alternative to above-knee amputation in limb malignancies [1]. This operation was first described in 1930 by Borggreve [2]. Demel and Gold (1932 [3]) and van Nees (1950 [4]) reported about the use of this technique for the surgical treatment of congenital femoral dysplasia. More recently, by means of new diagnostic and therapeutic techniques, limb salvage procedures have also become possible in cases of malignant bone tumors [5, 6].
In 1976, Salzer was the first surgeon who published this method for operative treatment of osteosarcomas of the knee region [7]. In contrast to a thigh amputation, where an upper leg prosthesis becomes necessary, with a rotationplasty only a lower leg prosthesis will be needed while preserving an actively mobile knee joint. Further advantages include the preservation of the highly sensitive plantar surface and the possibility of further growth due to preservation of growth plates of the distal tibia in children, which can be used for length compensation.
A rotationplasty can be performed and preserve the extremity even in cases where other limb-salvage procedures are not possible anymore, such as skip metastases, inadequate soft-tissue conditions, or knee joint involvement [8, 9].
When performing a rotationplasty, preservation of the perfusion of the distal portions of the flap is paramount in order to prevent soft-tissue necrosis and subsequent complications.
In the past few years, intraoperative assessment of tissue perfusion using indocyanine green (ICG) fluorescence imaging has been introduced as a safe and simple method for various surgical indications to fill the gap between challenging preoperative imaging and subjective intraoperative evaluation [10, 11]. ICG is a fluorescent dye which is used in different medical diagnostics as an indicator substance and has a peak spectral absorption at about 800 nm. These frequencies penetrate retinal layers, allowing ICG angiography to image deeper patterns of circulation than fluorescein angiography. It is administered intravenously and the substance binds tightly to plasma proteins and becomes confined to the vascular system. Depending on liver function, it is eliminated from the body with a half-life of about 150–240 seconds [12]. The light needed for the excitation of the fluorescence is generated by a near infrared light source which is usually attached directly to a camera. A digital video camera allows the absorption of the ICG fluorescence to be recorded in real-time, allowing assess and document perfusion. Nowadays, ICG is routinely used intraoperatively in neurosurgical procedures, such as cerebrovascular and tumor surgeries [13], in breast cancer surgery [14], in lymphography [15, 16] and lymphatic surgery [17].
To our knowledge, this is the first report to demonstrate the applicability of intraoperative ICG monitoring during a rotationplasty to provide real-time angiographic images during pediatric tumor resection, providing an additional level of safety and precision.
Materials and methods

Post-contrast T1-weighted MR images of case 1. (a) Coronal image showing a large contrast-enhancing, well circumscribed mass adjacent to the femoral shaft with inhomogeneous enhancement. No bone edema was presented. (b) Note the regular course of the sciatic nerve (arrow) one axial plane without signs of perineural tumor infiltration.

Indocyanine green angiography (ICG) after revascularization (a) ICG angiogram shows earliest 100 % perfusion of ischiadic nerve (arrow); (b) ICG perfusion of Femoral artery (red arrow) and Femoral vein (blue arrow)

Indocyanin green angiography (ICG) show after revascularization lower leg
A total of three patients suffering from femoral sarcomas underwent tumor resection and rotationplasty in 2017. ICG fluorescence was used in all cases to control tissue perfusion.
For visualization, the SPY Near-Infrared Perfusion Assessment System manufactured by Novadaq Technologies Inc., Richmond, BC, Canada), which utilizes indocyanine green (ICG) 0,1 mg/kg body weight, is an imaging technology that allows real-time visual assessment of superficial blood flow. The ICG fluorescent molecule binds tightly to serum lipoproteins in the intravascular space, making its fluorescence an excellentmarker for blood flow. Additional SPY software (SPY-Q Analysis Toolkit, manufactured by Novadaq Technologies Inc.) allows for quantitative analysis of blood flow based on ICG fluorescence intensity.
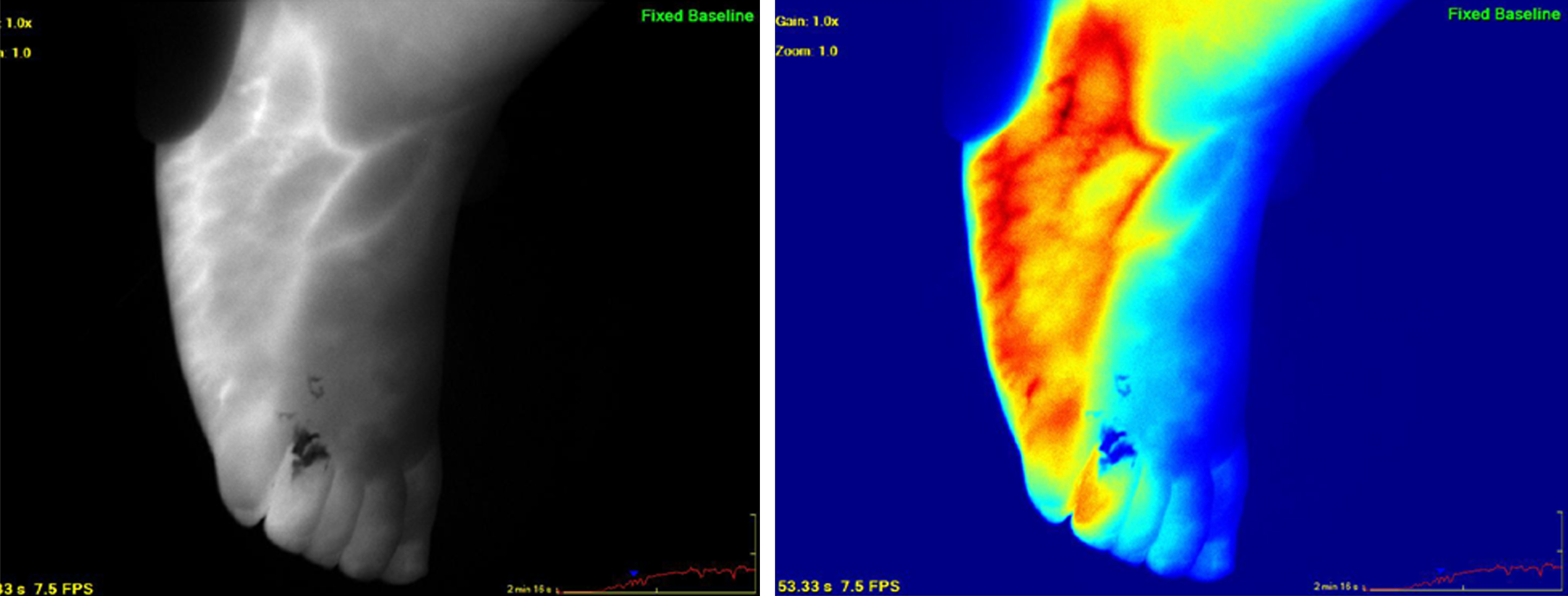
Indocyanin green angiography (ICG) show after revascularization foot and superficial venous
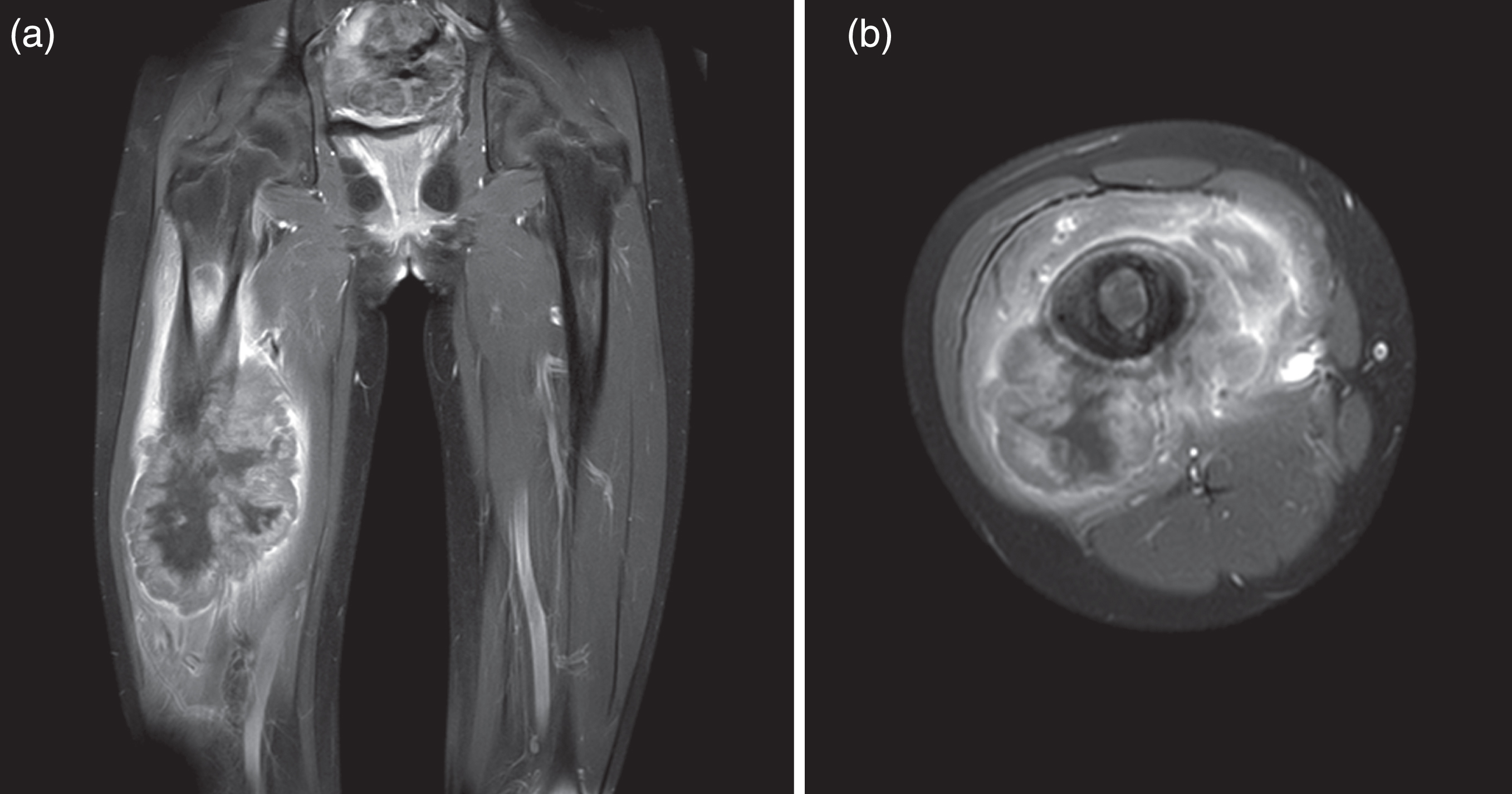
Post-contrast T1-weighted MR-imaging of case 2 (a) showing a large irregular shaped mass of the right femur with central necrotic parts and bone edema. (b) On axial plane the tumor mass is directly adjacent to the sciatic nerve but without signs of perineural infiltration.
One female and two male patients with a mean age of 26.3±53.5 months old (range 20–132 months) underwent rotationplasty. Mean follow up was three months. Early postoperative outcomes were all outstanding and no major postoperative complications occurred. Intravascular fluorescence occurred approximately 20 seconds after the intravenous bolus, and was directly observed through the ICG camera system.
In the mid-seventies, the Borggreve rotationplasty was introduced by Salzer as a possibility of surgical treatment for malignant bone tumors of the distal femur [7]. Overall, the number of patients who were operated using this technique is small. However, rotationplasty can be a valuable limb-salvage procedure for malignant conditions, and continues to remain an important tool in the armamentarium of orthopedic oncologists and plastic reconstructive surgeons. The technique is especially suited for young and still growing patients because differences in length can be compensated until skeletal maturity. A rotationplasty provides the advantage of a biologic and functional joint reconstruction with normal sensation and proprioception at the level of the contralateral knee [18]. Further rotationplasty shows good treatment modality with excellent clinical and good functional results [19–21].
Main requirements to enable the procedure are a tumor-free dissection and preservation of the sciatic-, tibial-, and peroneal nerves as well as a normal ankle function. While less ideal, in the case of tumor infiltration the affected structures can be resected and re-anastomosed. In all instances, careful patient selection and meticulous preoperative planning with a precise anatomical understanding are essential for a successful procedure.
During the last years, intraoperative ICG monitoring has become a versatile tool for several indications, and most authors use 0.2–0.5 of ICG per kg body weight [22]. In our experience, 0,1 mg/kg body weight provided a good concentration for adequate visualization. Extra boluses of ICG can be used to clarify the vascular anatomy while dissecting the neurovascular bundles. In the presented preliminary study, ICG fluorescence was used to better visualize the angioarchitecture during tumor resection and while performing the rotationplasty to provide essential information about tissue perfusion, which is a key element for sufficient soft tissue reconstruction. In this way, we were able to verify tissue perfusion during preparation in order to reduce the risk for postoperative complications such as wound healing disorders or flap necrosis.
There occurred no adverse event due to the systemic injection of fluorescein. Using ICG-enhanced fluorescence allowed the surgeon to identify anatomic variations, which are frequent in pediatric tumor growth. Interestingly, we observed that the first structure which showed fluorescence was the perivascular system of the sciatic nerve, even before the main arterial vessels.
The advantages of ICG application include that it remains strictly intravascular, therefore limiting artefacts due to extravascular leakage. It also has a short half-life, allowing repetitive injections. Disadvantages of ICG lie in the initially high cost of the device, the poor visualization of the surgical field and a limited magnification due to chromatic aberration effects [23–25].
Conclusion
ICG fluorescence is a safe and simple technique, which was found to be a valuable tool to guide rotationplasty surgery. Given the ease of use and low complication rates this technique should be considered when planning complex ablative and reconstructive procedures such as rotationplasties. Prospective studies are necessary to confirm its role and to assess the clinical benefits of ICG in the setting of oncologic tumor resections and reconstructions.