
Abstract
BACKGROUND:
Hepatic echinococcosis (HE) is a zoonosis and depicts a rare but potentially lethal disease caused by larval infestation of E. multilocularis (alveolar echinococcosis, AE) and E. granulosus (cystic echinocococcosis, CE). In many countries, HE is a critical public health problem. Clinically, HE patients initially are often asymptomatic for years. Depending on the echinococcal manifestations patients can later develop unspecific symptoms as fatigue, abdominal pain and may present with elevated transaminases, jaundice and hepatomegaly. The combination of grey scale ultrasound and serological tests has been the gold standard for the screening and diagnosis of HE. Besides MRI, CT and FDG-PET scans, safe and directly accessible contrast-enhanced ultrasound (CEUS) may easily help to indirectly describe perilesional inflammation. Upon diagnosis of HE, an appropriate therapeutical strategy should be evaluated in a multidisciplinary way.
OBJECTIVE:
The aim of the present retrospective monocenter study is to assess the diagnostic performance of CEUS examination in the evaluation of hepatic echinococcal manifestation by comparison with CT, MRI, FDG-PET scans and histopathology.
METHODS:
Out of 36 patients with echinococcal disease (16 patients with E. multilocularis infection, 12 patients with E. granulosus infection and 8 patient with unspecified Echinococcus infection) 8 HE patients (4 patients with E. multilocularis, 2 patients with E. granulosus and 2 patients with unspecified echinococcal liver disease) were included in this study on whom CEUS was performed between 2008–2016. The applied contrast agent was a second-generation blood pool agent (SonoVue ®, Bracco, Milan, Italy). CEUS examinations were performed and interpreted by a single experienced radiologist with more than 15 years of experience.
RESULTS:
All patients were examined without occurrence of any side effects. In all 4 AE patients, contrast enhancement could be detected by means of CEUS and was confirmed by MRI or PET-CT scan. In the remaining 4 patients (CE and unspecified echinococcosis), doppler ultrasonography, CEUS and corresponding CT or MRI scans could not detect any hypervascularization of the lesions of interest. The histopathological analysis did not reveal any viable parasite material. CEUS showed a sensitivity of 100% and a specificity of 100% compared to MRI, CT or FDG-PET-CT.
CONCLUSIONS:
CEUS depicts a safe method for the evaluation of echinococcal liver disease. In addition to serological tests and grey scale ultrasound, CEUS imaging could be integrated as an easily accessible tool helping to describe hypervascularization as a sonomorphological correlate for active perilesional inflammation of echinococcal manifestations. CEUS may further help to differentiate between CE and AE and also to evaluate treatment outcome.
Keywords
Introduction
Hepatic echinococcosis (HE) is a zoonosis and depicts a rare but potentially lethal disease caused by larval infestation of E. granulosus and E. multilocularis. In many countries echinococcosis is a major public health problem.
Cystic echinococcosis (CE), caused by E. granulosus, occurs worldwide [1, 2]. There are endemic areas especially in South America, East Africa and central Asia and Mediterranean countries.
The WHO Informal Working Group (WHO-IWGE) established an international standardized classification for CE in 2003 by which CE is subdivided in active (CE1/2), transitional (CE3) and inactive (CE4/5) stages [3]. The incubation period is variable. Characteristically, CE initially manifests as a single cyst which usually grows during the course of the disease. Clinically, CE is asymptomatic until complications emerge among which are mass effect, haemorrhage, cyst rupture and consecutive anaphylaxis, development of fistula or bacterial superinfections [4]. Besides ultrasound as the gold standard for CE screening and diagnosis, additional immunological tests are performed. Therapeutical options for CE patients are surgical resection, percutaneous interventions like PAIR (puncture, aspiration, injection and re-aspiration), chemotherapy and watch and wait concepts. Alveolar echinococcosis (AE) which is caused by E. multilocularis is mainly distributed in the Northern hemisphere [4] and shows an invasive tumor-like appearance, thus it often leads to complications as infiltration of vessels and bile ducts causing bleedings and jaundice, respectively. Hence, prognosis often is poor. Likewise the TNM classification for malignant tumors, the WHO Informal Working Group introduced the PNM classification for the staging of alveolar echinococcosis [5]. Clinically, AE patients initially are often asymptomatic for years. Depending on the echinococcal manifestations patients later develop unspecific symptoms as fatigue, abdominal pain and may present with elevated transaminases, jaundice and hepatomegaly. Not rarely, AE affects multiple organs. Treatment options comprise surgery, benzimidazole chemotherapy, percutaneous or endoscopic interventions [6].
The combination of clinical examination, epidemiological information, abdominal ultrasonography and serology helps with the diagnosis of HE. In addition, MRI, CT and FDG-PET scans are performed for validation and specific analysis of the lesions of interest and for assessing vascular or biliary infiltration. Safe and directly accessible contrast-enhanced ultrasound (CEUS) may easily help to describe the active inflamed surrounding tissue [7]. The advantage of CEUS is that it is a non-ionizing imaging modality and and it can be safely applied in patients with hyperthyroidism, kidney failure or underlying allergic reactions against iodinated contrast media. The aim of the retrospective monocenter study was to evaluate the diagnostic performance of CEUS in HE patients in comparison with CT, MRI, FDG-PET scans and histopathology [8].
Materials and methods
This retrospective study was approved by the local institutional ethical committee of the institutional review board and all contributing authors followed the ethical guidelines for publication in Clinical Hemorheology and Microcirculation [9]. All study data were gathered according to the principles expressed in the Declaration of Helsinki/Edinburgh 2002. Oral and written informed consent of all patients were given upon CEUS, CT, MRI and FDG-PET scans and their associated risks and potential complications have been carefully described. All CEUS examinations were performed and analyzed by a single skilled radiologist with more than 15 years of clinical experience. All included patients underwent native B-mode, Color Doppler and CEUS scans. Up-to-date high-end ultrasound systems with adequate CEUS protocols were utilized (GE Healthcare: LOGIQ E9; Samsung RS80A Prestige, sSiemens Ultrasound Sequoia S20000, S3000, Philips Ultrasound iU22, EPIQ 7). A low mechanical index was used to avoid early destruction of microbubbles (<2,0) [10]. For all CEUS examinations, the second-generation blood pool contrast agent SonoVue ® (Bracco, Milan, Italy) was used [11]. 1,0–2,4 ml of SonoVue ® were applied. After contrast agent was applied, a bolus of 5–10 ml sterile 0,9% sodium chloride solution was given. No adverse side effects upon administration of SonoVue ® were registered. All CEUS examinations were successfully performed and image quality was sufficient in every single case. The patient files and imaging records were collected from the archiving system of our institution.
A total of 8 patients with diagnosed HE on whom CEUS was performed between 2008–2016 were included in this retrospective monocenter study. The mean age of the patients at the time of CEUS performance was 41 years (min. 27; max. 62;±11.5).
The CE-CT, MRI and FDG-PET scans comprised imaging series using standard scanning protocols performed on scanners used at the time of the examinations. CE-CT scans were performed using standard scanning protocols on different CT scanners: Siemens SOMATOM Force, Siemens SOMATOM Definition Flash, Siemens SOMATOM Definition AS.
The histopathological analysis was performed in collaboration with the local Department of Pathology.
Results
Contrast-enhanced ultrasound could successfully be performed in all 8 patients without occurrence of any adverse reaction. One of the 8 included patients (patient #3) showed an 8,4×6,1 cm inhomogeneous lesion within the left lobe of the liver (Fig. 1A). Whereas Doppler ultrasonography could not detect hypervascularization of the lesion, by means of CEUS a contrast enhancement in the marginal zone and within the septa could be obtained upon application of SonoVue ® (Fig. 1B).
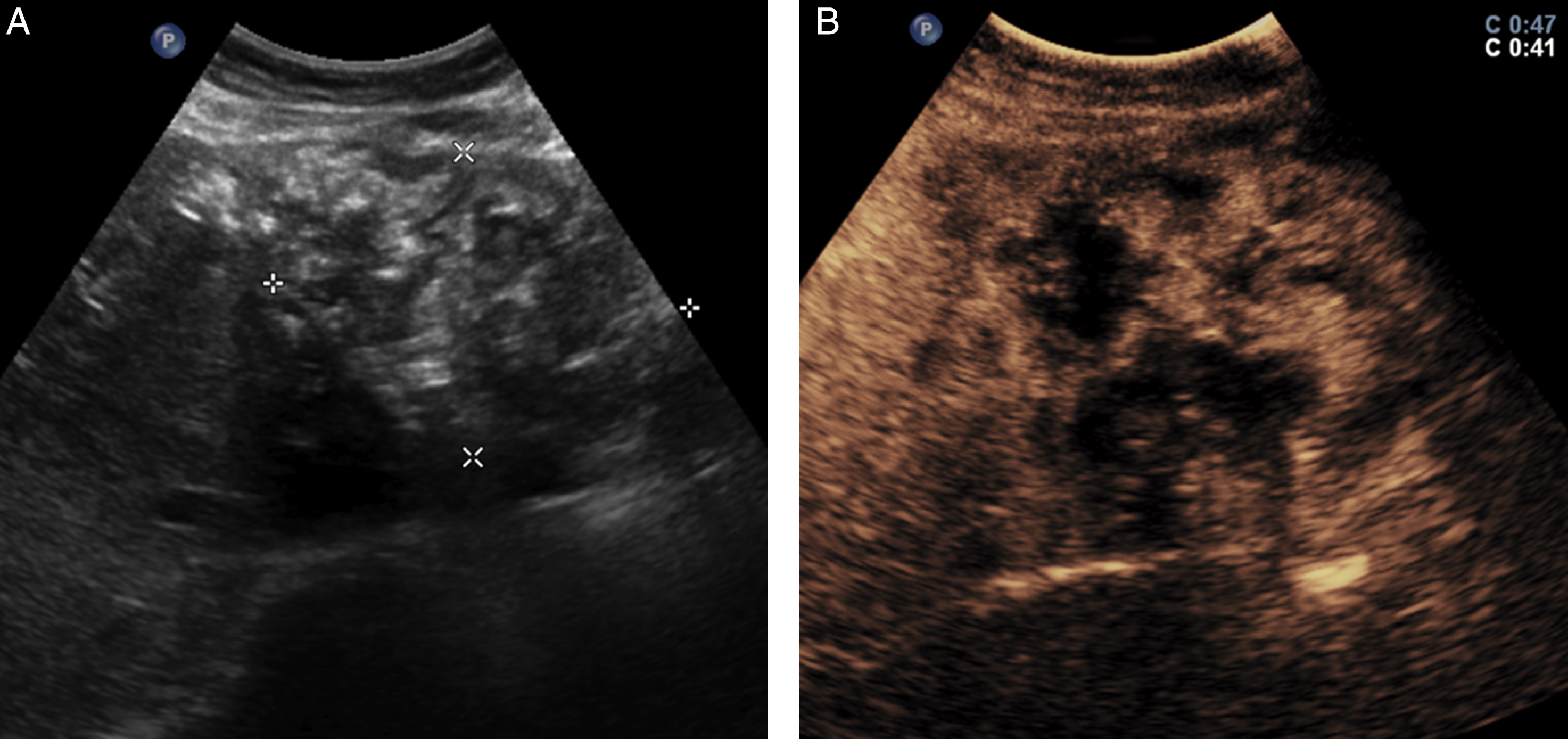
A. Native B-mode ultrasound shows a 8,4×6,1 cm inhomogeneous lesion within the left lobe of the liver with hyper- and hypoechoic areas. B. CEUS examination shows a marginal and septal contrast enhancement.
The corresponding MRI scan verified the pattern of enhancement seen during CEUS examination. Upon administration of contrast, septal and marginal contrast enhancement could be detected (Fig. 2C/D). By ELISA, the antigen Em10 which was described to be expressed by mature protoescolex and the germinal layer of larvae could also be detected [12, 13]. The Antigen B (AgB) ELISA - AgB is a specific secretory protein of E. granulosus - was negative [14]. The histopathology confirmed hepatic alveolar echinococcosis without detection of viable parasite material. The combination of the results above strengthen the underlying infestation of E. multilocularis with signs of surrounding hepatic inflammation. Another AE patient (patient #4) showed a heterogenous lesion in the right liver lobe in B-mode ultrasound with partial echo extinction because of calcifications (Fig. 3A). No hypervascularization could be seen in Doppler ultrasonography (images not provided). The following CEUS examination revealed marginal contrast enhancement (Fig. 3B). No central contrast uptake of the lesion could be observed. The CE-CT scan confirmed a central hypodense lesion within the right liver lobe with diffuse calcifications and partially marginal enhancement. The corresponding FDG-PET scan revealed a multifocally enhanced FDG uptake in the periphery of the lesion. In contrast, the central region showed no FDG uptake (Fig. 3D). The histopathology confirmed underlying hepatic alveolar echinoccosis, no vital parasite material could be observed.

A. Native T1-weighted image shows the heterogeneous lesion in liver segments II-IV with dominating areas of low signal, axial reformation. B. Native T2-weighted shows dominating areas of high and low signal, axial reformation. C. Contrast enhanced T1-weighted image shows septal and marginal contrast enhancement, axial reformation. D. The corresponding coronal reformation of contrast enhanced T1-weighted images.

A. B-mode ultrasound shows a 8×8 cm heterogeneous lesion within the right liver lobe with partial echo extinction due to calcifications. B. The corresponding CEUS reveals marginal contrast enhancement. No central contrast enhancement could be detected. C. The CE-CT scan (here axial reformation, venous phase) confirms the lesion of interest with areas of contrast enhancement and diffuse calcifications. D. The FDG-PET scan shows multifocally FDG-uptake in the periphery of the echinococcal lesion.
In AE patient #1, CEUS examination revealed septal and marginal contrast enhancement of the hepatic alveolar echinococcal manifestation in the right lobe which was confirmed by MRI. In AE patient #3, CEUS examination could show septal contrast enhancement, which was also validated by MRI.
In the remaining 4 patients (2 CE patients and 2 unspecified HE patients), neither Doppler ultrasound, CEUS nor corresponding CT, MRI or FDG-CT scans could detect any sites of hypervascularization or glucose hypermetabolism. Moreover, no signs of viability could be observed in the histopathological analysis of the 4 AE patients and the 2 CE patients (Fig. 4). There was no histopathological correlation of the unspecified echinococcosis patients. CEUS showed a sensitivity of 100% and a specificity of 100% compared to MRI, CT or FDG-PET scans.

Performed diagnostic tools on included echinococcosis patients. AE = alveolar echinococcosis. CE = cystic echinococcosis.
Hepatic echinococcosis is a potentially life-threatening disease. The diagnosis of HE is mainly achieved by means of ultrasound and immunoserological tests. Up to now, no reliable serological markers for assessing viability of echinococcosis have been described [15–17]. So far, FDG-PET is used for visualizing enhanced glucose metabolism as a correlate for hypermetabolic and inflamed (peri-) lesional tissue and serological screening for antigens and antibodies, e.g. Em10 which is a viability-associated antigen of AE, are performed. The development of lesional calcifications and shrinkage of HE lesions did not prove to be reliable morphological correlates for inactivity of echinoccosis, as it was shown that despite increasingly calcified and reduced size, some HE lesions still showed increased FDG uptake [17]. Furthermore long-term treatment with benzamidazoles did not correlate with inviable HE [18]. In a previous prospective study following 36 AE patients during treatment, it could be shown, that CEUS is able to detect viable HE lesions (specificity 100%, sensitivity 69%) [19].
As a sonomorphological correlate for perilesional inflammation and hence indirectly echinococcal viability by utilizing CEUS, hypervascularization of echinococcal lesions could be detected in all AE patients, whereas in the remaining CE and unspecified echinococcosis patients no hypervascularization could be observed. The vascularization pattern was verified by FDG-PET or MRI scan. Our retrospective study is in line with recent results of Kaltenbach et al. [19]. In a prospective study they could show that by using CEUS, in 22 out of 32 FDG-PET-positive AE patients hypervascularization could be observed.
Because of its cystic configuration and the granulomatous and later surrounding fibrous tissue (pericyst) [4] in sharp contrast to the infiltrative nature of AE lesions, CE lesions characteristically do not show surrounding inflammation and hypervascularization at the time of the diagnosis [20]. In both included CE patients as in the two included unspecified HE patients, no hypervascularization could be detected neither by CEUS nor by MRI nor CT. The histopathological analysis did not reveal any viable parasite material in all included patients.
CEUS is a non-invasive, easy accessible and cost-effective imaging modality which allows for further characterization of different pathological conditions, like gallbladder diseases, vascular complications after kidney transplantation or endoleaks after endovascular aortic repair [21–23]. In our study, CEUS helps visualizing enhanced microcirculation and thus active perilesional inflammation of hepatic echinococcal manifestations [24]. It remains to be further elucidated if the viability status of HE lesions can be concluded from observed (peri-) lesional contrast enhancement via CEUS as a sonomorphological correlate for surrounding active inflammatory response. Moreover, the visualization of (peri-) lesional hypervascularization may help to differentiate between HE and CE. The promising use of this non-ionizing imaging modality in combination with eligible serological viability markers might help for the diagnosis and follow-up during therapy of HE patients. By using CEUS in the future clinical setting, the usage of ionizing FDG-PET-CT scans for treatment monitoring could be reduced [25, 26].
The retrospective nature, limited patient numbers, the heterogenous cohort and differing ultrasound systems are limiting factors of our retrospective monocenter study. Future prospective and multicenter trials are necessary to further assess the role of CEUS in the diagnostic workup of HE and treatment monitoring.