
Abstract
While fractional flow reserve (FFR) is a good diagnostic index to assess the myocardial ischemia, coronary flow reserve (CFR) and the index of microcirculatory resistance (IMR) can be used to address microvascular status without any significant epicardial disease. The independent predictors for FFR and IMR are totally different and acts differently on the macro- and micro-vascular dysfunction. In high FFR patients, low CFR and high IMR which indicates the presence of overt microvascular disease demonstrated poor prognosis. Thus, comprehensive physiological assessments using FFR, CFR and IMR could improve the ability to discriminate patients at high risk of future events.
Keywords
Introduction
Myocardial ischemia is the most important prognostic factor and ischemia-based revascularization has been a standard of care in patients with coronary artery disease. Since the coronary artery system has 3 components with different functions (epicardial coronary arteries, arterioles, and capillaries), myocardial ischemia can occur when any one of these systems fails. Although fractional flow reserve (FFR) has been used to detect the myocardial ischemia and it can guaranty to safely defer functionally insignificant lesion [1], in the FAME II study, 14.6% of the registry arm (FFR > 0.80 and deferral of PCI) experienced persistent angina [2]. Coronary flow reserve (CFR) and index of microcirculatory resistance (IMR) represent the microvascular status when there is no significant epicardial disease. In our recent study, patients with low CFR and high IMR (overt microvascular disease) had a significantly higher risk of clinical events [3]. In addition, the presence of low CFR in conjunction with high IMR was the most powerful independent predictor for clinical events among patients with high FFR. Although the microvascular system cannot be visualized by invasive coronary angiography, its function and presence of microvascular disease can be evaluated by invasive physiologic indices. IMR is a specific index for microvascular status, and can be measured by a thermodilution technique. In this review, we will focus on the role of microvascular disease and its clinical prognosis using the index of IMR.
Measurement of microvascular disease
Only 5% of the total coronary tree can be detected by the coronary angiogram and the substantial amount of coronary circulation depends on the microvascular function [4]. Since major controller of coronary resistance and flow is microcirculatory beds, the presence of epicardial coronary stenosis is not always a prerequisite for the ischemic heart disease (IHD). The maximal perfusion ability for the evaluation of coronary flow is fundamentally based on maximum reduction of microvascular resistance. In order to evaluate epicardial coronary artery and microcirculatory function, three functional indices can be utilized which are FFR, CFR, and IMR [5]. These indices can be easily measured with one interrogation of pressure-temperature sensor wire using thermodilution technique (Fig. 1). The patient had a typical chest pain on exertion and a positive exercise stress test. Coronary angiography showed no obstructive epicardial coronary artery disease and FFR was insignificant. However, IMR was high suggesting the presence of microvascular disease.
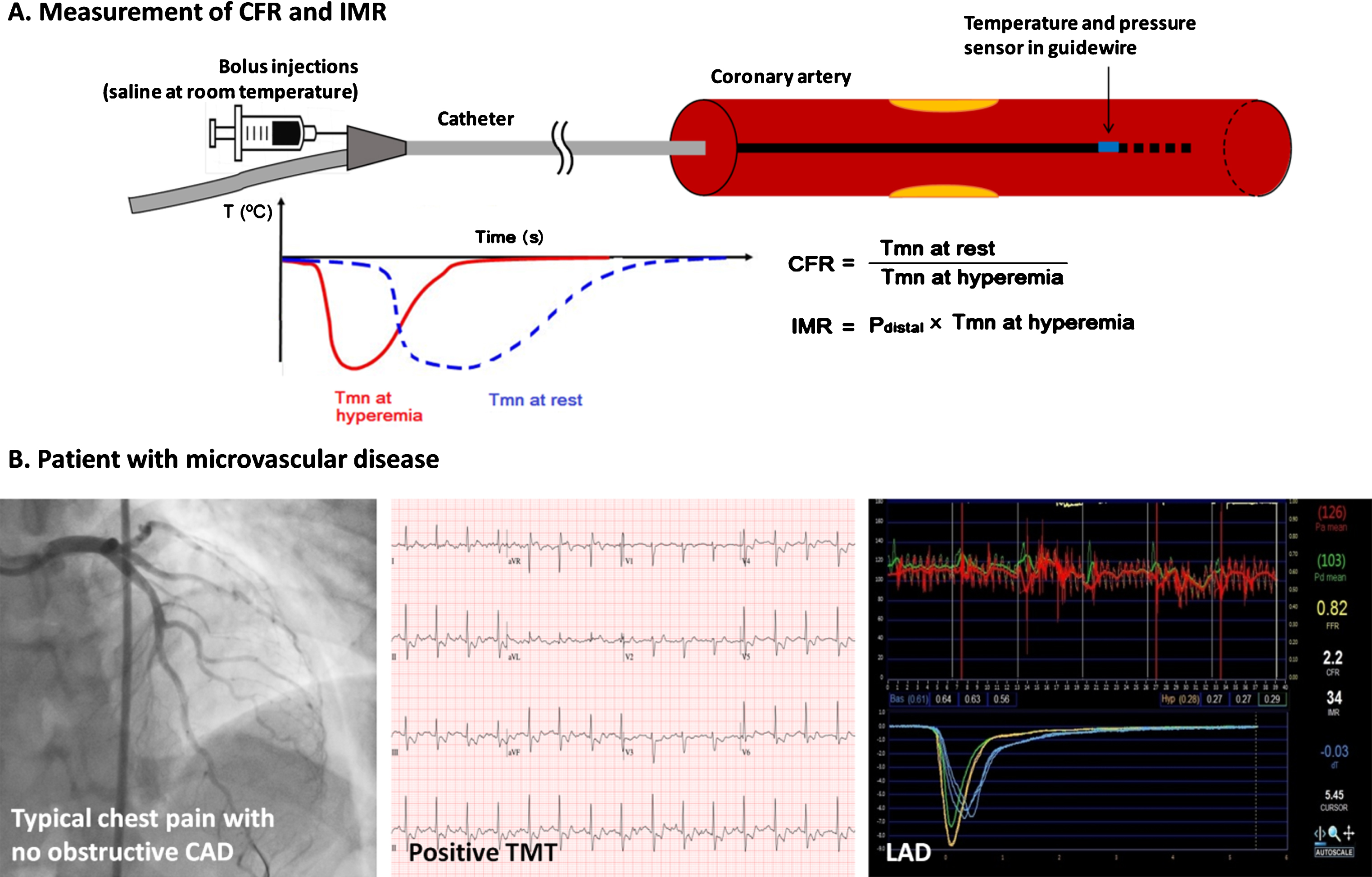
Measurement of CFR and IMR. CAD = coronary artery disease; CFR = coronary flow reserve; FFR = fractional flow reserve; IMR = index of microcirculatory resistance; LAD = left anterior descending artery; LCX = left circumflex artery; Tmn = mean transit time; TMT = treadmill test.
Our previous study investigated the distribution and determinants of IMR in patients with IHD [6]. The international IMR registry data of 1096 patients with 1452 coronary arteries from 8 centers in 5 countries were analyzed. In order to exclude the possibility of secondary microvascular damage from acute MI, these patients were excluded from the study. When evaluating the association with epicardial coronary stenosis severity, FFR showed significant correlation with diameter stenosis (DS) of epicardial disease (r = 0.561, p < 0.001). However, IMR did not show any correlation with DS (r = 0.033, p = 0.252). Furthermore, the independent predictors for low FFR (≤0.80) and high IMR (>75th percentile) were totally different. Previous MI, right coronary artery, female sex and obesity were predictors of high IMR, whereas left anterior descending artery, % DS ≥50, male, age were those of low FFR. In another study to evaluate the association between the markers of atherosclerotic burden in epicardial coronary artery, the correlation between SYNTAX score and IMR value was assessed [7]. In this study, IMR ≤25 was considered normal in non MI population. The vessel-specific and overall SYNTAX score had no significant correlation with IMR. Another representative scoring system, Gensini score, had no significant correlation with IMR at the patient level, whereas it had a weak negative correlation at the vessel level. The results from these studies suggest that macro- and micro-vascular diseases seem to possess independent disease process with different predictors for its development, although complex interaction could be presented.
Clinical prognosis of microvascular disease
To evaluate the prognostic implications of abnormal CFR and IMR in high FFR patients, a total of 313 patients with 663 vessels were assessed in our previous study [3]. The study showed that comprehensive physiological assessment using both CFR and IMR to stratify high FFR patients could differentiate patterns of microvascular status among the patients with functionally insignificant macrovascular disease. The demographic and risk factor profiles were well reflecting real world population of ischemic heart disease. Mean SYNTAX score was 7.0, Gensini score was 17.0, and 45% of patient showed multivessel disease. The included lesions were mainly intermediate degree of stenosis and mean FFR was 0.85 while mean CFR was 2.81. In this study 75th percentile value of calculated IMR was 21.6. Since this study focused on patients with functionally insignificant epicardial coronary stenosis, the patients with high FFR had % DS of 37, FFR of 0.91, CFR of 2.9 and IMR of 20. These high FFR patents were divided into 4 groups according to CFR and IMR. High CFR and low IMR group (61.3%) represents normal microvascular function, and low CFR and high IMR group (7.0%) represents overt microvascular disease. These 4 groups cannot be discriminated using conventional risk factors and they can be only discriminated by utilizing multiple physiologic criteria. During 2 years of follow-up, only low CFR and high IMR group showed significantly higher rates of patient-oriented composite outcome of any death, MI, and revascularization (hazard ratio: 5.623; 95% confidence interval: 1.234 to 25.620; p = 0.026). As seen in this study, the presence of overt microvascular disease was associated with poor prognosis in high FFR populations, and the comprehensive physiologic evaluation is essential to stratify those patients with overt microvascular disease.
Conclusions
Although FFR-based decision making for intermediate or ambiguous coronary lesions has been a standard practice, even among patients with high FFR and deferred revascularization, there may be myocardial ischemia due to combined microvascular disease or the influence of diffuse atherosclerotic narrowing. Measuring thermodilution CFR and IMR can provide additional insight about potential causes of IHD. Thus, comprehensive physiological assessments using FFR, CFR and IMR could improve the ability to discriminate patients at high risk of future events.