
Abstract
INTRODUCTION:
We aimed to evaluate whether PIRADS 3 lesions in multiparametric MRI (mpMRI) represent a significant risk of prostate cancer (PCa) in a real-world setting of different referring radiologic institutes.
MATERIALS AND METHODS:
Between May 2015 and October 2017, a total of 408 patients were referred to our clinic for MRI-ultrasound fusion targeted biopsy of the prostate (FusPbx) due to suspected prostate cancer. In all patients, preoperatively an mpMRI of the prostate was performed by altogether 62 different radiologic institutes. Prostate lesions were classified according to the PIRADS system. A PIRADS 3 lesion was diagnosed in 41 patients. FusPbx was performed transrectally using a Philips EPIQ 7 (Philips Medical Systems, Bothell, WA) scanner with plane wise fusion of ultrasound and MRI image data. In addition to FusPbx in each patient a randomized 12-core transrectal ultrasound guided biopsy (USPbx) was performed.
RESULTS:
Mean PSA Level was 9.5 ng/ml (range: 1– 26 ng/ml), mean patients age was 66.1 years (48.6– 80.4). In 11/41 patients (26.8%) prostate cancer was diagnosed by FusPbx of the PIRADS 3 lesion. In the target lesion PCa was classified as Gleason Score 3+3 in 5 patients, as 3+4 in 3, 4+3 in 1, 4+4 in 1 and 4+5 in 1 patient. In patients with negative FusPbx USPbx revealed PCa in another 7 patients (17.1%). In 5 of these GS 3+3 PCa was found, in another 2 patients GS 3+4 PCa.
CONCLUSIONS:
PIRADS 3 lesion indicates an equivocal likelihood of significant prostate cancer. In our series the overall PCa detection rate was 26.8% and 14.6% for clinically significant cancer in PIRADS 3 lesions. This evokes the question, if PIRADS 3 lesions could be surveilled only. The findings should be confirmed in a larger series.
Introduction
An ongoing discussion about overdiagnosis and overtreatment of prostate cancer (PCa) started a couple of years ago [1–3] leading to new therapeutic options for clinically non-significant cancer [4]. Since then, imaging modalities gained importance in the primary diagnosis of PCa [5] as well as in the follow-up after organ-preserving therapy [6, 7].
Multiparametric MRI (mpMRI) might help to differentiate between clinically significant and non-significant PCa and therefore gained importance in the diagnosis of PCa [8–11]. According to current guidelines, a mpMRI should be considered in biopsy negative patients with elevated prostate specific antigen (PSA) level [12]. A mpMRI consists of a T2-sequence assessing the prostate anatomy as well as a functional diffusion-weighted (DWE) and a dynamic contrast-enhanced (DCE) sequence.
The widespread acceptance and use of mpMRI however, showed a great variation in performing, interpretation and reporting mpMRI of the prostate. Therefore, the European Society of Urogenital Radiology (ESUR) developed the Prostate imaging-reporting and data system (PI-RADS), a scoring system for prostate MRI to standardize interpretation [13]. In 2015 the American College of Radiology presented the updated second version, called PI-RADS v2 [14]. The classification is based on a five-point scale (Table 1) comprising the findings of mpMRI in T2W, DWI and DCE. By this, the likelihood of PCa for any lesion within the prostate can be expressed [14]. According to the ‘Epstein criteria’ clinically significant cancer is defined as Gleason score 7a or greater, more than three positive biopsy cores or a tumor infiltration of one core of more than 50% [15]. The likelihood of clinically significant cancer is equivocal (Table 1) when PIRADS 3 is reported in the mpMRI [14]. A biopsy may be appropriate depending on the clinical suspicion of the presence of PCa, e. g. an elevated PSA level or an abnormal digital rectal examination (DRE). There are no specific recommendations, if a PIRADS 3 lesion should be biopsied or surveilled. Recent studies including the PRECISION trial showed that the detection rate of PCa in a PIRADS 3 lesion is up to 34% [10]. However, only a small number of studies exist evaluating the detection rate of PCa in a PIRADS 3 lesion. In this study, we aimed to evaluate whether PIRADS 3 lesion in mpMRI represent a significant risk of PCa.
PI-RADS version 2 assessment categories [14]
PI-RADS version 2 assessment categories [14]
Patients characteristics
In this retrospective single center study, a total of 408 patients with a PIRADS 3, 4 or 5 lesion in the mpMRI were referred to our institute for MRI-ultrasound fusion targeted biopsy of the prostate between May 2015 and October 2017. A mpMRI was performed due to an elevated PSA level or abnormal DRE or a previous negative randomized transrectal ultrasound-guided biopsy and persisting suspicion of PCa. In all patients a standard 12-core transrectal ultrasound-guided biopsy of the prostate was performed additionally according to current guidelines [12]. We reviewed clinical and pathological data including patient age, PSA level and Gleason score of the target lesion and random biopsy [16]. The study was performed according to the ethical guidelines of our clinic and as well of the Clinical Hemorheology and Microcirculation journal [17].
mpMRI and MRI-Ultrasound targeted biopsy of the prostate
A mpMRI was performed in each patient prior to the biopsy due to clinical suspicion for PCa by altogether 62 different radiologic institutes. Only patients with a PIRADS 3, 4 or 5 lesion were included in the study. The categorization of each lesion in the mpMRI was assessed according to the PI-RADS classification version 2 [14]. In 41 patients a PIRADS 3 lesion was reported. Image fusion was done software-assisted using the Philips Percunav® device (Philips Medical Systems, Bothell, WA). The registration was realized with plane wise fusion of the ultrasound and MRI image data using the T2-weighted axial MRI sequence. The fusion of the MRI and ultrasound image is outlined in Fig. 1. The fusion biopsy as well as the 12-core randomized biopsy were performed transrectally using an end-fire probe with the Philips Epiq 7 (Philips Medical Systems, Bothell, WA) scanner. The standard biopsy consisted of 12-cores collected from the lateral and medial aspects of the base, mid, and apical part of the prostate on the left and right side. The number of cores gathered from the target lesion ranged between minimum two and maximum four cores depending on the size of the target.
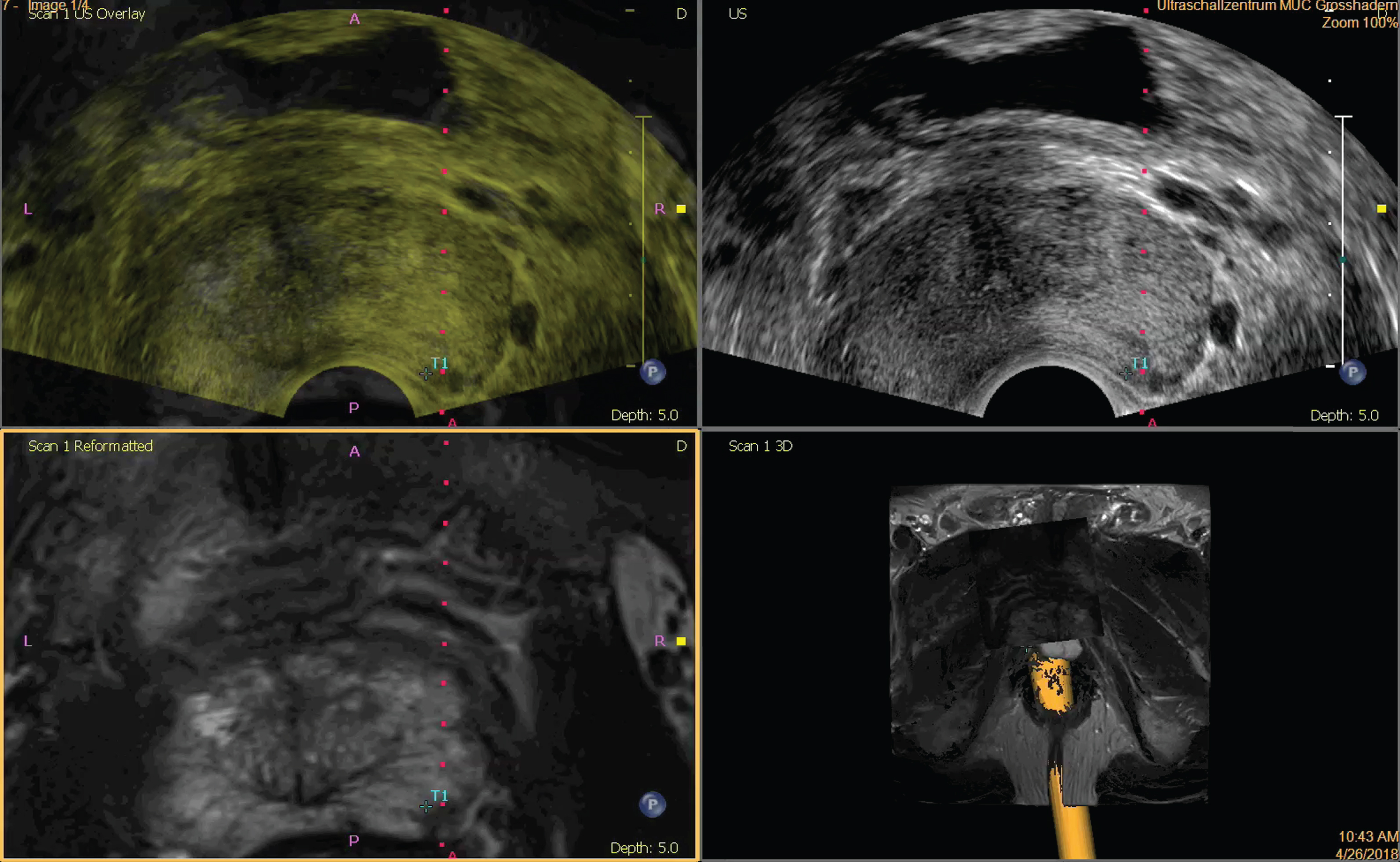
Image fusion of the axial T2-weighted MRI sequence with the axial real-time ultrasound image by plane wise fusion of the two image modalities. The target is marked as ‘T1’.
The overall cancer detection rate was defined as proportion of positive biopsies among the biopsied PIRADS 3 lesion or the random biopsy. The number of positive biopsies of the PIRADS 3 lesion as well as of the random biopsy were also displayed according to the Gleason score and categorized in clinically insignificant or clinically significant cancer. Continuous data are shown using medians and ranges and categorical data were summarized using frequencies and percentages.
Results
The patient demographic and clinicopathologic characters are shown in Tables 2 and 3. Mean patients age was 66.1 (48.6– 80.4) years and mean PSA level was 9.5 (range 1– 26) ng/ml. In 41 patients a PIRADS 3 lesion was reported in the mpMRI. A PIRADS 4 lesion was diagnosed in 190 patients and a PIRADS 5 lesion in 147 patients.
Patients and baseline characteristics
Patients and baseline characteristics
Histopathology of detected PCa in PIRADS 3 lesions
PCa was found in 11/41 patients (26.8%) with a PIRADS 3 lesion. Gleason score 6 was found in 5/11 patients (45.4%), Gleason score 7a in 3/11 patients (27.3%), Gleason score 7b in 1/11 patients (9.1%), Gleason score 8 in 1/11 patients (9.1%) and Gleason score 9 in 1/11 patients (9.1%) with a positive target lesion.
In patients with a negative targeted biopsy, PCa was diagnosed in 7/41 patients (17.1%) by the 12-core random biopsy. Only Gleason 6 or Gleason 7a PCa was found in the standard TRUS guided biopsy. Gleason score 6 PCa was diagnosed in 5/7 patients (71%) and Gleason 7a in 2/7 patients (29%) in the random 12-core biopsy.
In patients with a positive fusion biopsy the random biopsy was positive in 10/11 patients (90.9%) as well. 9/10 (90%) of those patients had the same Gleason score in the fusion as well as in the random biopsy. Only one patient (10%) showed a higher Gleason score in the random biopsy compared to the fusion biopsy.
More clinically significant cancer (Gleason 7a or greater) was diagnosed in the target (6/41 patients; 14.6%) compared to the random biopsy (2/41 patients; 4.9%).
MRI-ultrasound fusion based targeted biopsy of the prostate is well recognized and established for PCa detection [8– 10, 18]. Several studies could prove superiority of the MRI-Ultrasound fusion based targeted biopsy over the standard biopsy, especially in the detection of clinically significant cancer [8– 10, 18– 20]. According to the PIRADS classification in PIRADS 1 or 2 lesions clinically significant cancer is described as highly unlikely or unlikely to be present [14]. On the contrary to PIRADS 4 or 5 lesions which are characterized that clinically significant cancer is likely or highly likely present [14]. In the clinical practice PIRADS 4 or 5 lesions are generally biopsied to gain histological provement. However, studies are missing proving this approach and general recommendations for the treatment of lesions in the prostate classified according to the PIRADS system [14] from national or international guidelines do not exist at present. PIRADS 3 lesion, however, indicate by definition an equivocal likelihood of significant PCa and therefore are challenging for the clinical management. In the literature the detection rate of PCa in PIRADS 3 lesions is described as between 6.5% and 34% in the recently published PRECISION trial [10, 21– 24]. Those findings are comparable to our study with an overall detection rate of PCa of 26.8% in PIRADS 3 lesions. In our study, clinically significant cancer was diagnosed in 14.6% (6/41 patients) which is similar to the PRECISION trial with a detection rate of 12% [10]. Other studies describe a lower rate of clinical significant cancer with only 4.4% [21].
In the published literature there is a large variability of reported PCa detection rates in PIRADS 3 lesions arising questions for the further treatment strategies [10, 24]. In the presented study, we therefore aimed to assess the likelihood of PCa detection in PIRADS 3 lesions in a real-world setting with numerous referring radiologic institutes. The presence of clinically significant PCa in 14.6% of the patients with a PIRADS 3 lesion represents a relatively low risk. However, we suggest that a PIRADS 3 lesion should be biopsied additionally when performing a systematic biopsy due to suspicion of PCa.
In our series with a large number of referring radiologic institutes, the overall detection rate of PCa was 26.8% in PIRADS 3 lesions. Other studies with only one referring radiologic institute showed a slightly higher PCa detection rate in PIRADS 3 lesions of 39% [25]. The recently published PRECISION trial with several different referring radiologic institutes reported a PCa detection rate of 34%, in PIRADS 3 lesions which is comparable to our data [10]. Those findings evoke the impression that the assessment of the PIRADS classification is reproducible in a real-world clinical setting. Training, however can improve quality and reproducibility of mpMRI prostate imaging [26, 27], and potentially lead to a higher PCa detection rate.
Conclusion
In this large series of >60 referring radiologic institutes the overall PCa detection rate in PIRADS 3 lesions was 26.8% and for clinically significant cancer 14.6%. We therefore recommend taking an additional biopsy of any PIRADS 3 lesion whenever a randomized biopsy due to the suspicion of PCa is indicated.