
Abstract
OBJECTIVE:
Objective of the study was to assess the performance of ultrasound strain elastography combined with conventional B-mode ultrasound to diagnose suspicious breast lesions (BI-RADS 4 and 5).
METHODS:
Between January 2015 and December 2017, a total of 86 patients (55±17.9 years) with solid or unclear, non-cystic breast lesions were enrolled in the study. The breast lesions were evaluated by B-mode ultrasound and subsequent ultrasound strain elastography. Ultrasound features including echo pattern, lesion shape, marginal characteristics, calcifications, orientation and posterior features are useful for differentiating benign breast lesions from malignant ones. Malignant ultrasound features are irregular shape, hypoechoic pattern, spiculated margin, nonparallel orientation and posterior shadowing. Lesions with benign features such a circumscribed margin were classified as low conspicuous. In patients with highly conspicuous malignant masses ultrasound-guided core needle biopsy or surgical excision was performed.
RESULTS:
Among the 86 patients, 60 masses were histologically proven and 36 of these were malignant. Of the malignant lesions 26 invasive carcinomas were of no special type (NST), 1 invasive lobular carcinoma, 3 ductal carcinomas in situ and 6 metastases. 20 of these patients had breast density classified as ACR 3 or 4. The mean size of the masses was 1.2 cm (range: 0.5–5 cm). Based on ultrasound B-mode imaging, the lesions were classified as BI-RADS category 4 (n = 20; three 4a, nine 4b and eight 4c) and BI-RADS category 5 (n = 16). One patient had to be reclassified after strain elastographxy to BI-RADS 3.
The sensitivity of ultrasound with strain elastography and additional B-Mode ultrasound for the characterization of solid breast lesions was 97%, for conventional B-mode alone 92%; the respective specificities were 82% and 73%, respectively.
CONCLUSION:
Ultrasound elastography can be a supplementary approach to conventional ultrasound to improve the diagnostic accuracy of malignant breast lesions.
Keywords
Introduction
Breast cancer is one of the most common malignant solid tumors in women. According to a survey of the Robert Koch Institute there were 72.000 new cases of breast cancer diagnosed in Germany in 2016 [1]. The incidence of breast cancer is still rising and patients tend to be affected at a younger age [2, 3]. Nearly 30 % of the women with breast cancer are younger than 55 years at diagnosis. At this age, most other cancer types play a marginal role [1]. Patients with breast cancer benefit from medical advances in recent years. This is reflected in the good prognosis of this cancer, the five-year survival rate of patients suffering from breast cancer is nearly 79–88% percent after diagnosis [1]. The World Health Organization (WHO) attributes this to the improved diagnostic methods with earlier detection through screening and awareness efforts, as well as breakthroughs in treatment [4]. Nowadays there are several imaging techniques for the diagnosis of breast cancer available. Ultrasound and ultrasound elastography play an important role in dense glandular tissue. For lesions in which the biopsy is indicated and if there is a discrepancy between the findings of BI-RADS 3 and 4a, ultrasound elastography may be helpful to increase diagnostic confidence [5, 6]. There are two main elastography methods described, i.e. strain and shear wave elastography. At present, strain elastography is the most widespread method for the characterization of soft tissue stiffness [7, 8].
Previous studies have demonstrated that malignant and benign breast lesions can be differentiated based on the information of tissue stiffness [8–10], as soft tissue deforms more than stiff ones [7, 12].
Ultrasound elastography is able to visualize breast masses that are not detectable in conventional ultrasound, especially in dense breast tissue. Until now, such masses were diagnosed as conspicuous only as palpation findings [13].
In prior studies, elastography has been used to characterize conspicuous breast lesions, with greater sensitivity and specificity (41.0–98.5%) than B-mode ultrasound (7.1–98.8%) [14, 15].
Ultrasound elastography combined with conventional B-mode ultrasound imaging increases the diagnostic performance [16–21].
Pu et al. [22] demonstrated that in breast screening after re-evaluation of the inconsistent by shear wave elastography results between mammography and conventional ultrasound, the diagnostic performance significantly increased, so that shear wave elastography was reported to be a powerful tool for further assessment of such inconsistent malignant findings of traditional imaging methods.
The purpose of our study was to assess the diagnostic performance of ultrasound strain elastography as complements to the conventional B-mode ultrasound in diagnosis of suspect breast lesions.
Materials and methods
Study design
From January 2015 to December 2017, a total of 86 patients (mean age 55±17,92 year; age range, 23–86 years) with solid and suspect / unclear breast lesions (BI-RADS 4 and 5), were enrolled in this retrospective study. Breast lesions (mean size: 12 mm±0,5; range: 5–50 mm), discovered with standard clinical examination or detected incidentally during prior imaging study, were evaluated by B-mode ultrasound and ultrasound elastography in the university hospital.
The inclusion criteria were as follow: 1. Palpable in physical examinations or visible on imaging breast lesions; 2. Solid or predominantly solid breast lesions; 3. No treatment such as breast surgery, chemotherapy or radiotherapy performed on the lesion. If multiple lesions were present (n = 2), only the most conspicuous lesion at ultrasound was selected.
Pathologic results of 60 masses determined by US-guided core needle biopsy or surgical excisions were used as a reference standard.
The local ethics committee approved the study, and written informed consent was collected from all patients who were enrolled in the study (Vote 17-694-104).
Conventional ultrasound and ultrasound elastography
Conventional ultrasound and ultrasound elastography were performed in all patients in their supine position by the same ultrasound scanner (LOGIQ E9, GE Healthcare, Milwaukee, USA). Linear multifrequency transducer (frequency range 6–15 MHz) was used for B-mode ultrasound and for ultrasound elastography. Bilateral whole breast ultrasound examination was performed by one radiologist with Ultrasound experience of more than 10 years’ experience with more than 3000 patients per year. Images were stored in DICOM standard and send to the PACS for independent reading by two radiologists in consensus. After B-Mode ultrasound examination the same radiologist performed also ultrasound elastography on the same screen. Elastography images were generated using freehand manual compression.
First, two-dimensional ultrasound imaging was performed on the breast lesions to observe the number, location and the size of the lesion. Shape, margin, orientation to the plane of skin, echo patterns, posterior acoustic shadowing, internal calcification of the masses were also evaluated. Second, all lesions were categorized according to the BI-RADS classification [23]. Third, for elastography the same depth, focus position and gain setting were used as during conventional imaging. Finally, the strain ratio was measured by five-point elastic score that visually ranked the stiffness [7]. Blue represented stiff tissue and red represented soft tissue. This scoring is a qualitative evaluation. Similarly to all ultrasound techniques, operator dependency is also a limitation of the elastographic evaluation.
Statistics
All samples are described with arithmetic mean and standard deviation. To calculate sensitivity, specificity, positive predictive value, and negative predictive value the following formulas were used based on the agreed table 2×2 (TP: true positive, FN: false negative, TN: true negative, FP: false positive): Sensitivity = TP / (TP + FN) Specificity = TN / (FP + TN) Positive predictive value = TP / (TP + FP) Negative predictive value = TN / (FN + TN) Accuracy = (TP + TN) / (TP + TN + FP + FN).
Results
From 86 patients 60 conspicuous breast lesions were histologically proven, 36 of those were malignant and 24 were benign. The malignant lesions included invasive carcinomas of no special type (NST) (n = 26, Fig. 1), invasive lobular carcinoma (n = 1), ductal carcinomas in situ (n = 3, Fig. 2), and metastasis in breast tissue (n = 6); the benign lesions were fibroadenoma (n = 10), fibrotic nodules (n = 10), scar with fibrosis (n = 2), hematoma with particular necrosis (n = 1). Concerning the metastasis two were classified as lymphoma, one as malignant melanoma, one as plasma cell myeloma (Fig. 3), one as chloroma (Fig. 4) and one as squamous cell carcinoma of unknown primary site. The pathological results are summarized in Table 1. The malignant lesions were more frequently found in elder (>50 years; 23/36, 64%) than in younger patients (<50 years; 13/36, 36%). Based on ultrasound imaging, the lesions were classified as BI-RADS category 4 (n = 20; three 4a, nine 4b and eight 4c) and BI-RADS category 5 (n = 16). Three lesions in the BI-RADS category 4a were diagnosed as malignant after histological assessment. Figure 5 shows one false positive lesion of conventional ultrasound with unclear margin (BI-RADS 4a). At ultrasound elastography the lesion appears to be relatively circumscribed in margin. Using both imagine methods the lesion was classified as BI-RADS 3. Histological results confirmed that this lesion is a fibroadenoma.
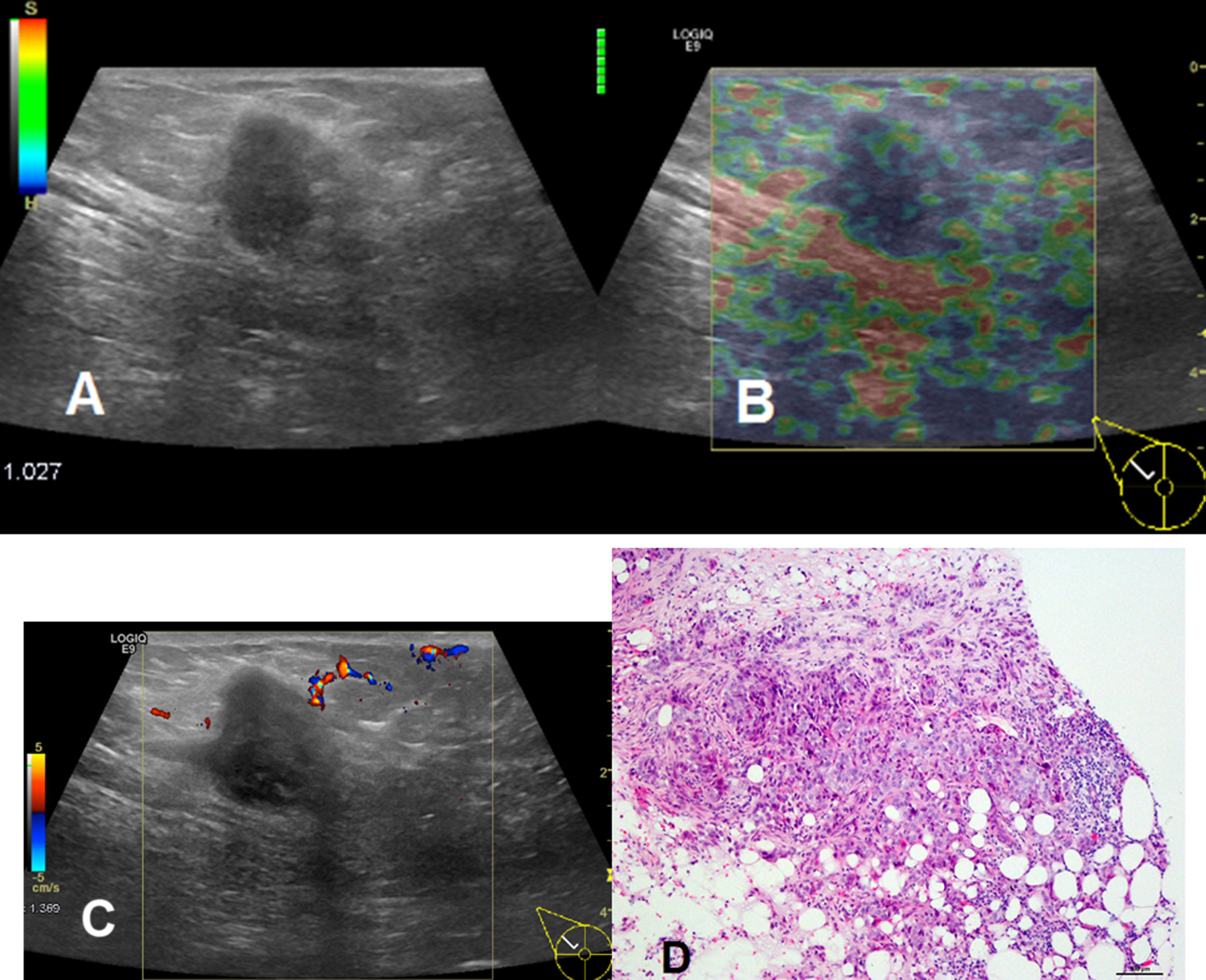
Grade 3 invasive carcinoma of no special type (NST) in a 64-year-old woman. (A) Conventional ultrasound shows a 15×22 mm hypoechogenicity breast lesion with irregular shape, nonparallel orientation, unclear margin which is classified as BI-RADS 5. (B) At the ultrasound elastography, the lesion appears to be relative stiff. (C) The color blood flow signal is visible outside the lesion. (D) Histological result (hematoxylin-eosin, original magnification×200) confirms the diagnosis of invasive carcinoma of no special type (NST).

Ductal carcinoma in situ in a 52-year-old woman. (A) Conventional ultrasound of dense breast tissue (ACR 3) shows three breast lesions. The lesion 2 in the middle 5×5 mm shows hypoechogenicity, irregular shape, nonparallel orientation and posterior shadowing which is classified as BI-RADS 4c. (B) Ultrasound elastography shows that the lesions are stiff and the boundaries are better defined. (C) Histological result (hematoxylin-eosin, original magnification×200) confirms the diagnosis of ductal carcinoma in situ.

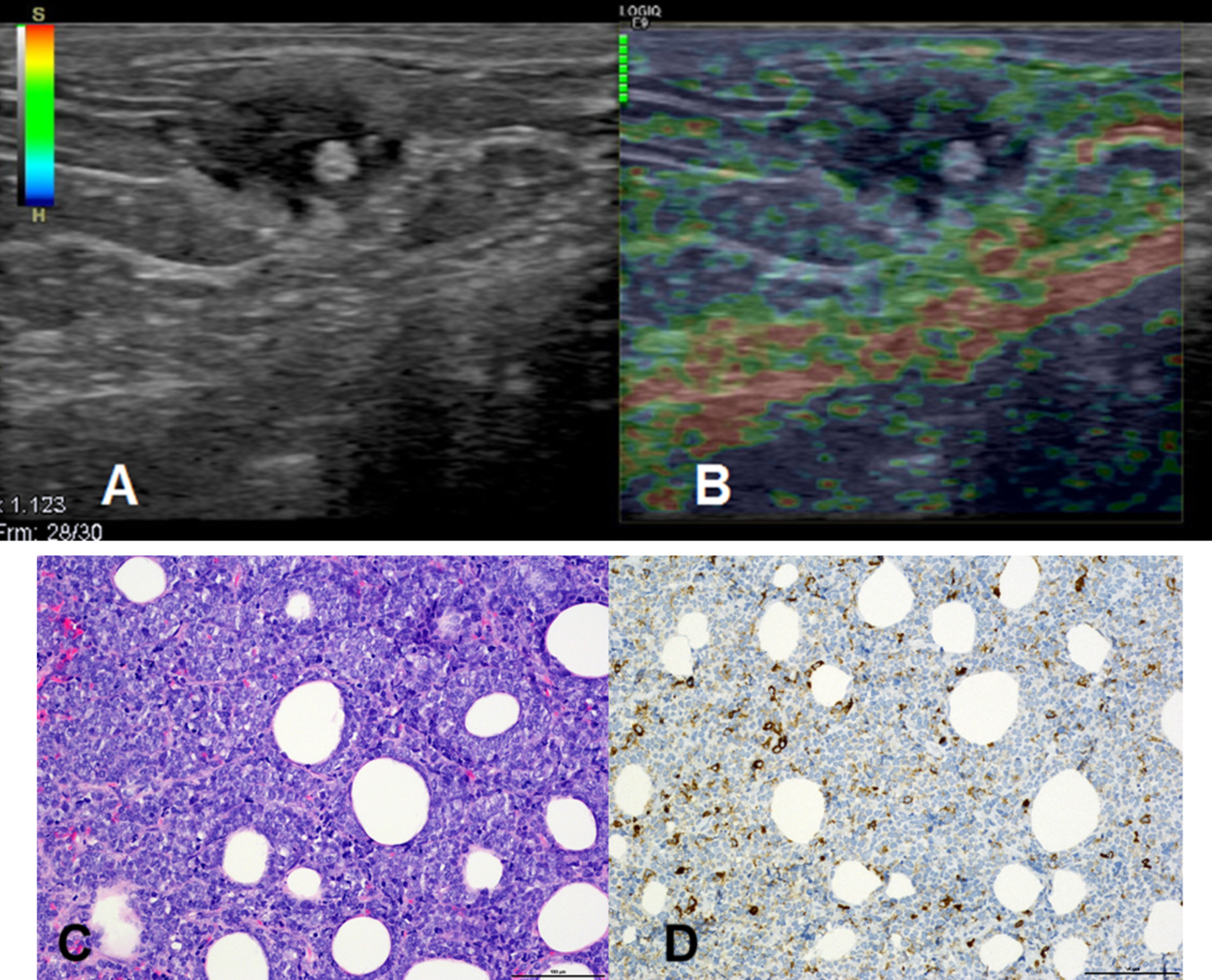
Breast metastasis from plasma cell myeloma in a 74-year-old woman. (A) Conventional ultrasound of dense breast tissue (ACR 3) shows a 36×25 mm hetero-echogenicity breast lesion with irregular shape, rough margin which is classified as BI-RADS 5. (B) At the ultrasound elastography, the lesion appears to be relative stiff. (C) Histological result (CD138, original magnification×200) confirms the diagnosis of breast metastasis from plasma cell myeloma.
Breast chloroma in a 45-year-old woman with acute myeloid leukemia. (A) Conventional ultrasound of dense breast tissue (ACR 3) shows a 15×20 mm heteroechogenicity ovoid (in transverse) mass with irregular shape, rough margin and a 5 mm hyperechogenicity round part at the lower edge area which is classified as BI-RADS 4b. (B) At the ultrasound elastography, the lesion appears to be relative stiff. (C), (D) Histological results (hematoxylin-eosin (C) and Myeloperoxidase (MPO) (D), original magnification×200) confirm the diagnosis of chloroma.
Pathological distribution of the 36 breast lesions
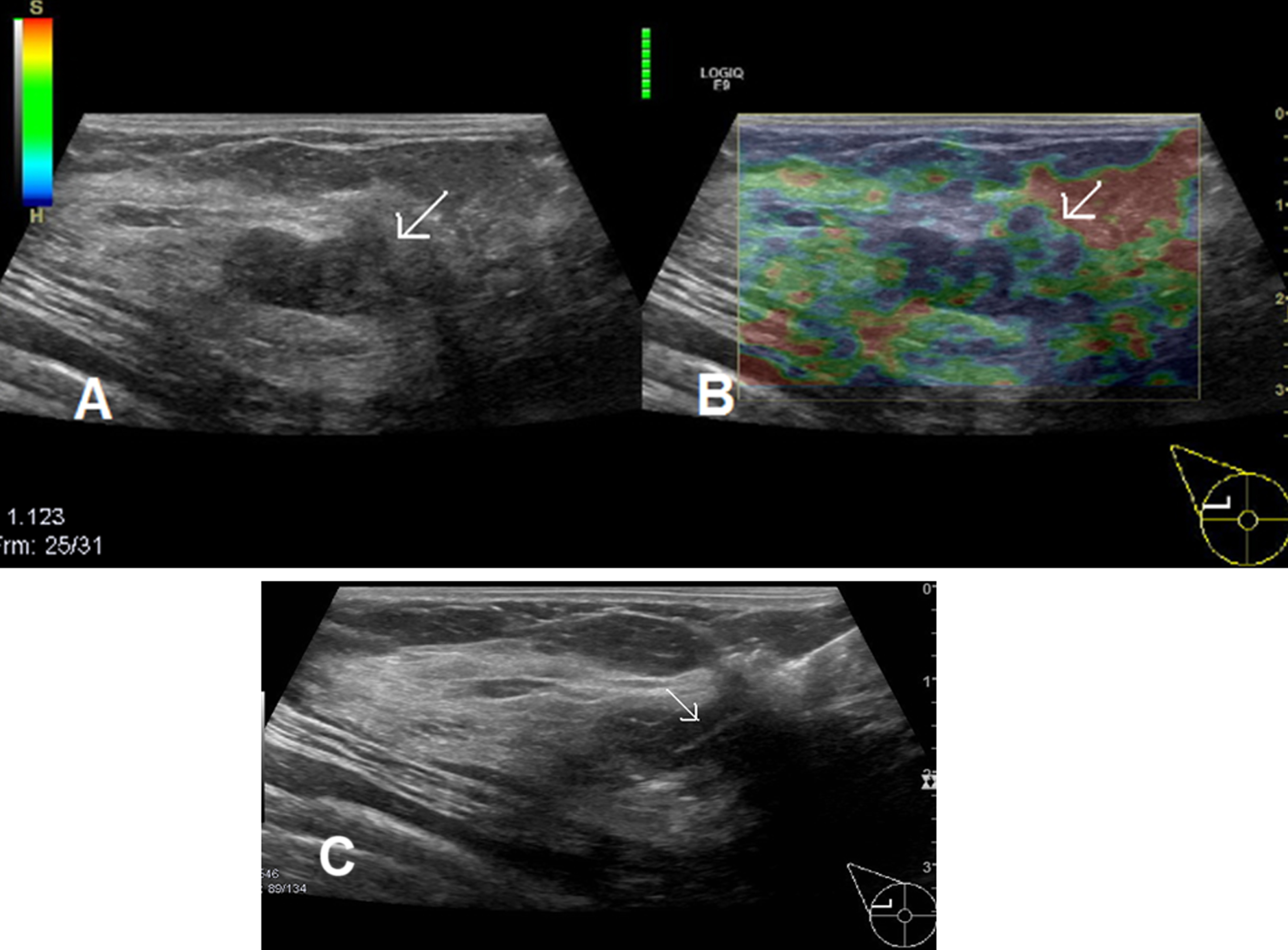
Breast fibroadenoma in a 26-years-old woman. (A) Conventional ultrasound of dense breast tissue (ACR 3) shows a 10×20 mm hypoechogenicity ovoid (in transverse) mass with not completely circumscribed margin (black arrow) which is classified as BI-RADS 4a. (B) Ultrasound elastography shows that the lesion is relatively homogeneous and appears to have relatively regular shape (black arrow). (C) Images from ultrasound guided core biopsy (white arrow).
Ultrasound features such as shape, margin or echo pattern are summarized in Table 2.
Breast density also based on ultrasound findings: 20 of these patients had breast density classified as ACR 3 or ACR 4. 31 lesions (86%) were located at the upper lateral quadrant of the breast: 15 on the right side and 16 on the left side.
The sensitivity of ultrasound with strain elastography and additional B-Mode ultrasound for the characterization of solid breast lesions was 97%, for conventional B-mode alone 92%; the respective specificities were 82% and 73%, respectively.
Basic characteristics of the ultrasound feature of the lesions
Diagnostic performance of ultrasound (a) and of ultrasound with real-time elastography (b)
The breast density influences the image quality in the diagnosis of breast cancer. Using Ultrasound as diagnostic tool, this influence is discussed to be less significant compared to other modalities [24, 25]. In the study presented here, ultrasound could be demonstrated as efficient approach in malignancy prediction of conspicuous solid breast lesions.
Palpation of the breast is a very effective method for the detection of abnormal masses, with hardness being an indicator of malignancy. Elastography has been developed based on this fundamental principle. Elastography is a sonographic imaging technique that provides qualitative and quantitative data by comparing the hardness of a target tissue with that of the adjacent breast tissue.
There is growing evidence pertaining to the importance of breast elastography in the BI-RADS classification [26]. Ultrasound elastography in conjunction with BI-RADS are proven to increase diagnostic specificity and sensitivity [27]. Wang reported that the combination of BI-RADS and 3D-shear wave elastography were a useful tool for predicting breast malignant lesions in comparison with BI-RADS alone and demonstrated the usefulness of shear wave elastography in differentiating benign from malignant lesions [28]. Very recently, Zhao et al. found using strain elastography and a cut-off point of 2.98 a sensitivity, specificity and accuracy of the strain ratio method of 86.9%, 86.6% and 82.6%, respectively, for patients with BI-RADS-US 3 and 4A lesions [29].
In the present study strain elastography was applied. With this method tissue displacement is estimated with freehand compression technique and presented by a color map and digital data [30]. Soft tissues often undergo substantial deformation in contrast to hard tissue, which is subject to small deformations. In malignant lesions, elasticity is lower due to the increased hardness and lead to smaller deformation. Wan et al. [31] reported that triple-negative breast cancer was associated with high elasticity score and mean shear wave values on acoustic radiation force impulse (ARFI) imaging which may indicate a high probability of malignant.
In our study we used ultrasound elastography complementary in addition to conventional ultrasound in patients with conspicuous or unclear breast lesions. The diagnostic performance using both imaging methods was superior (sensitivity: 97%, specificity: 82%) to that of using conventional images alone (sensitivity: 92%, specificity: 73%). These high diagnostic values may be due to our high experience: in our department ultrasound elastography is performed in all patients with dense breast tissue and unclear breast lesion. With conventional ultrasound and ultrasound elastography, only one malignant lesion (2,8 %) was misdiagnosed. This one false negative lesion was a grade 1 invasive carcinoma of no special type (NST) with a diameter of 6 mm in dense breast tissue (ACR 3). Small lesions might be softer and tumor size had significant effect on tissue stiffness measurement. Small breast cancers (≤10 mm) were more likely to show benign features on ultrasound elastography in the study by Vinnicombe et al. [32].
Elastography can help to better assess the degree of risk of malignancy of sonogrpahically detectable lesions. This also makes it possible to target the indications for biopsies more precisely [33]. Our study is limited in its retrospective approach. It was a mono-centric study with relative small number of patients. Another limitation of our study were differences in the density of the breast tissues adjacent to the breast lesions which affected the elasticity values [34]. Moreover ultrasound elastography is dependent on the experience of the radiologist. Finally, we did not perform the correlation among ultrasound and elastography with MRI and/or mammography. Rong et al. [35] reported that the combination of ultrasound elastography and MRI is effective in the diagnosis of breast cancer and can greatly improve the detection rate of malignant breast tumors. Further studies should be performed; whether ultrasound elastography brings added value to conventional ultrasound as an adjacent to mammography in breast cancer screening.
Conclusion
The information provided by ultrasound elastography alone is limited. However, ultrasound elastography can provide additional information to conventional ultrasound improving the reliable diagnosis of breast lesions. Thus, ultrasound elastography in combination with high-resolution B-Mode ultrasound may improve the diagnostic accuracy, increase the detection rate of malignant breast masses and reduce unnecessary biopsy (especially in BI-RADS 4 lesions).