
Abstract
The analysis of platelet aggregation and thrombosis kinetics has significantly advanced with progress in microfluidic technology. However, the results of platelet aggregation tests do not fully reflect the observed clinical outcomes. To address the present unmet clinical needs, the basic but essential biology of platelets should be reconsidered in relation to the characteristics of microfluidic systems employed for platelet tests. To this end, the present article provides an overview of commercially available point of care devices and focuses on recent microfluidic studies, describing their measurement principles. We critically discuss the characteristics of the microfluidics systems used to evaluate the complex processes underlying platelet aggregation, and that are specifically designed to mimic the pathophysiological environment of blood vessels, including hemodynamic factors as well as blood vessel injury. To this end, we summarize unsolved issues related to the application of platelet function tests based on microfluidics. Overall, we confirm that platelet function tests based on microfluidics provide a versatile platform that encompasses a variety of basic research, as well as clinical diagnostic applications.
Introduction
Platelets play an essential role in hemostasis, which minimizes blood loss in the event of vascular injury. During hemostasis, platelets are rapidly recruited to the site of injury on the vessel wall and then undergo a sequence of changes, including integrin activation, adhesion, spreading, reshaping, aggregation, secretory events, procoagulant surface exposure, and clot retraction, as shown in Fig. 1. Similar processes may occur in arteries and veins and can lead to thrombosis in blood vessels and, eventually, myocardial infarction or stroke [1].While hemostasis and thrombosis both result in clot formation, the clots are different and occur through distinct processes. In other words, the boundary between favorable hemostasis and adverse thrombosis is thin and platelets contribute to arterial and venous thrombosis. Therefore, platelet function should be balanced between hemostasis and thrombosis.
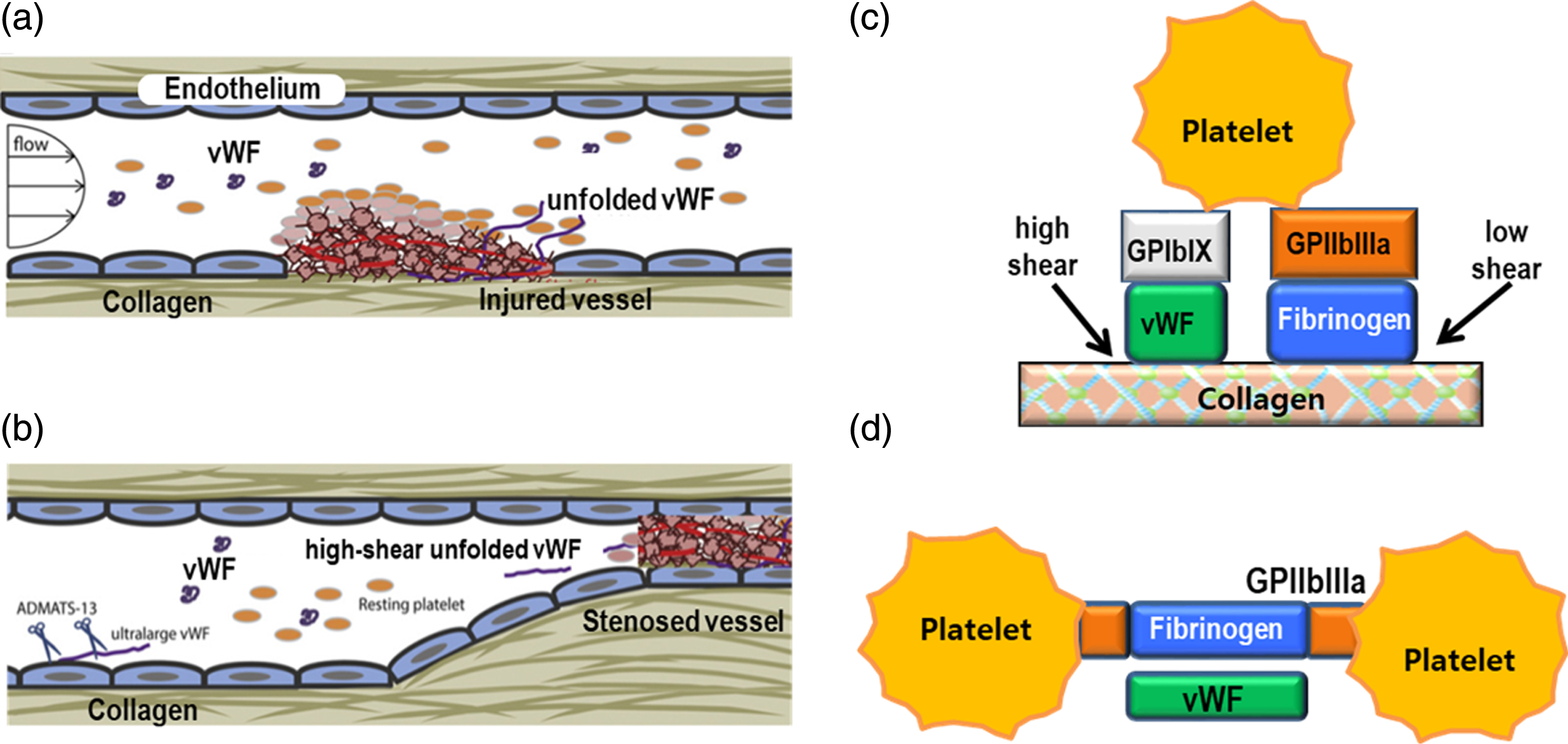
(a) Hemostasis at an injured vessel wall, (b) Thrombosis at a stenosed artery (adapted with permission, reference 80), (c) schematic of platelet adhesion and (d) schematic of platelet-platelet aggregation.
Owing to significant advances in biosensors and microfluidic technology, various devices and instruments are available to test platelet functions in clinical settings. Because of the rising incidence of atherothrombotic disease, reliable platelet function testing has become increasingly important. However, clinicians are not entirely satisfied with state-of-the-art technology devices, since clinical outcomes are not in full accordance with the results of the platelet function tests [2–4]. Furthermore, different devices produce highly variable, even opposite, results for the same test, thereby complicating clinical decisions [5–7]. Thus, As a consequence, the demand for new technical solutions and reliable tests is definitely urgent. In order to address the present unmet clinical needs, an in-depth understanding of the technical principles underlying detection systems including microfluidics is strongly required.
A number of excellent review papers and books dealing with platelet assay have been published, each with its own strengths [8–11]. Based on these reviews, the present article intends to provide engineers with basic and essential information necessary in the development of new devices suitable for in-depth evaluation of platelet function. This review summarizes the current commercially available technologies for point-of-care testing and recapitulates the recent microfluidic approaches for platelet function tests.
Coagulation is the process by which blood changes from a liquid to a gel state, forming a blood clot. The process consists of an enzymatic chain reaction involving both cellular (platelets) and protein (coagulation factors) components. Typical coagulation factors include calcium, thrombin, and fibrinogen. Any defect in these factors impairs coagulation. For instance, typical anticoagulants, such as EDTA and citrate, absorb calcium and halt the coagulation cascade. Platelets play a critical role in coagulation through the arrest of bleeding and the development of thromboses.
The overall process of thrombus formation can be briefly described as follows. When blood vessel injury occurs and the subendothelial collagen is exposed to blood, the von Willebrand factor (vWF) binds to the exposed collagen and adopts an unfolded conformation due to wall shear stress [12] as shown in Fig. 1. Platelets flowing near the vessel injury are arrested (adhesion) at the injured site owing to their interaction with both collagen and vWF, which initiates platelet activation and recruitment of additional platelets (aggregation). Activated platelets secrete various prothrombotic substances that accelerate platelet aggregation, ultimately leading to the formation of a platelet plug. The platelet plug provides a central area where different coagulation factors can induce the stable formation of fibrin-reinforced platelet plugs [13]. Platelets interact with fibrin fibers, which display a wide range of mechanical properties, to form a clot and stop bleeding.
Furthermore, platelets secrete numerous substances [14] upon activation by various agonists in the blood [15]. Hyperreactive platelets tend to form platelet plugs under normal blood flow conditions, resulting in coagulation-associated vascular occlusion. During these processes, platelet surface mediators such as glycoprotein (GP) complexes, collagen receptors, and α2β1 integrins bind to vascular ligands, e.g., von Willebrand factor (vWF) and fibrillar collagen. The interactions between platelets and the vascular subendothelium are significantly influenced by hemodynamic factors, and trigger signaling events that reinforce adhesion and promote platelet activation. Agonists in the bloodstream, such as adenosine diphosphate (ADP) and thrombin, are rapidly released from either the vascular wall or adherent platelets.
Platelets can bind directly to injured blood vessel walls, which contain a large number of adhesive macromolecules, such as laminin, fibronectin, collagen, and vWF, as shown in Fig. 1(c). The mechanisms of platelet adhesion at sites of injury are determined by the hemodynamic environments and the mechanical stiffness of the underlying substrate [16, 12]. Vessel wall injury exposes endothelial collagen to which the adhesive macromolecule vWF can bind. Under high shear flow, platelet adhesion relies on shear-dependent changes in vWF morphology [18]. Under low shear flow, vWF is irregularly coiled because of self-association, but is extended under high shear flow [19]. When a critical hydrodynamic force is exerted on vWF, the protein straightens like a threaded rope, until the coiled domains are exposed for binding to ligands, which, in turn, promote anchoring to the surface of the subendothelium and platelets even under high shear flow [19, 20].
The initial tethering of platelets to the collagen surface is mediated by interactions between the platelet receptor GPIb and vWF bound to collagen [21]. The binding of GPIb to vWF has a fast off-rate and is, therefore, insufficient to mediate stable adhesion, thus allowing rolling of platelets [22]. Stable platelet adhesion to collagen occurs via the two major direct collagen receptors: GPVI and integrin α2β1. Even though collagen is the primary platelet adhesion molecule, other substrates in the subendothelial matrix also help to stabilize platelet adhesion, including GPVI and the platelet integrin α6β1.
Platelet activation, adhesion, and secretion do not necessarily occur in a sequential manner. However, all of these processes eventually take place prior to platelet aggregation, leading to the formation of a platelet plug. Binding between platelets requires the activation of platelet receptor GPIIb/IIIa (also known as integrin αIIbβ3) and bridging of adjacent platelets by either fibrinogen or vWF [23]. Pharmacologic modulation of platelet hyperaggregation can be achieved by targeting the GPIIb/IIIa integrin complex, which results in the inhibition of fibrinogen binding. In fact, several GPIIb/IIIa blockers, such as abciximab, eptifibatide, and tirofiban, have been developed [24].
In addition to biochemical agonists, platelets can also be activated by physical stimuli, such as abnormally high shear stress. Many studies have reported that high shear forces cause binding of vWF to the platelet receptor GPIb, resulting in platelet activation and subsequent shear-induced platelet aggregation (SIPA) and thrombus growth [16]. Specifically, a pathological shear stress of 8 Pa or higher is required to activate platelets [25, 26], corresponding to shear rates of 5,000 s–1 or higher. In vivo, typical shear rates ranges near the wall are 20–200 s–1 for veins, 300–800 s–1 for large arteries, 500–1,600 s–1 for arterioles, and 800–10,000 s–1 for atherosclerotic stenosed arteries [21]. A recent study reported that a wall shear rate of 2,500 s–1 is the threshold for platelets activation and formation of dense platelet thrombi on collagen-coated surfaces [27]. Nevertheless, most SIPA studies have been conducted at physiological (500–1,500 s–1), rather than pathologically high, shear rates (>5,000 s–1), despite the latter rates being more clinically relevant for arteriothrombosis [28]. Notably, the SIPA process is non-enzymatic and aspirin-insensitive [26]. A recent study reported that protocatechuic acid inhibits SIPA and attenuates simultaneous platelet activation, including associated intracellular calcium mobilization, granule secretion, and adhesion receptor expression [29].
Point-of-care platelet function assay
Since the significance of platelet function in hemostasis has been demonstrated, there has been a high demand for platelet function testing methods and devices. Platelet function testing has become routine for predicting hemorrhage and monitoring the efficacy of antiplatelet treatments [6, 30]. Thus, owing to these clinical needs, numerous platelet assaying devices have been developed using leading-edge technologies [5, 30–32]. Although the present review describes several POC devices, as listed in Table 1, other available laboratory devices, such as those based on LTA (light transmission aggregometry), TEG®, ROTEM®, and flow cytometry are not reviewed in this article.
Point-of-care assays for the evaluation of platelet function
Point-of-care assays for the evaluation of platelet function
Electric impedance can detect platelet aggregation in optically opaque whole blood. Two platinum electrodes set at a fixed distance measure the time-dependent variation in electrical impedance as they are gradually covered with accumulating activated platelets. Platelet aggregation is automatically calculated as the area under the curve of impedance versus time [33]. A multichannel (5 channels) impedance-based analyzer (Multiplate® system, Roche Diagnostics, Switzerland) has become available with disposable cuvettes and standardized reagents [34].
Comparative studies indicate that this method yields results similar to those obtained via the classical turbidimetric aggregometry (LTA) but outperforms turbidimetric methods in the assessment of anti-platelet therapies [35]. The Multiplate® system is a flexible system that allows reagents to be changed and tested according to the researchers’ objectives, thus enabling the study of various pathways of platelet activation and aggregation. Also, multiple sensing systems allow one to perform several tests at once. However, the performance of the Multiplate® system is dependent on both the hematocrit (HCT) and the number of platelets. A recent clinical study reported that the Multiplate® system was not reliable in predicting adverse outcomes in patients with acute coronary syndromes (ACS) [3].
Verify now assay
The VerifyNow® System (Accriva Diagnostics, USA), formerly known as the Ultegra Rapid Platelet Function Assay, is based on optically turbidimetric measurements of whole blood using fibrinogen-coated polystyrene microparticles (5μm) and near-infrared nanoparticles [36, 37]. The detection chamber contains fibrinogen-coated beads and a specific platelet agonist, such as arachidonic acid (AA) or ADP+ prostaglandin E1(PGE1). Activated GPIIb/IIIa receptors on platelets bind to the fibrinogen on the beads, which leads to agglutination of the platelets and beads. As the agglutinated platelets and beads precipitate, infrared-light transmittance through the chamber increases as the platelets fall out of the solution. Due to the characteristics of infrared light, blood cells do not influence the detection of platelet/bead agglutination. Currently, there are two versions of this assay: the VerifyNow aspirin assay, which uses AA as the agonist, and the VerifyNow P2Y12 assay, which uses ADP as the agonist and is antagonized by PGE1. Owing to a well-designed disposable cartridge and an automated device, no pipetting is required and the test can be rapidly completed within 5–7 min. However, owing to its convenience-first design, the system is not very flexible and agonist changes are not allowed. Also, the VerifyNow® measurements are affected by both the HCT value and the number of platelets. However, correcting platelet reactivity for HCT did not improve the prediction of thrombotic events after percutaneous coronary intervention (PCI) [37]. In general, the VerifyNow Aspirin® assay yields more predictive results of adverse outcomes compared to LTA [38].
Platelet function analyzer
A platelet function analyzer (PFA; PFA-100 or -200, Siemens, Germany), is designed to expose platelets to shear stress and agonists and induce the formation of a platelet plug through a membrane aperture (150μm), while the flow rate is monitored over time [39]. During the test period, a constant suction pressure is applied (40 mbar) and the flow rate is monitored. When the flow rate falls to below 10% of the initial rate, the test records a parameter called “closure time”. The flow system is carefully designed to mimic physiological arterial flow conditions, including capillary size (200μm) and shear rate (4,000 to 5,000 s–1). A collagen-coated membrane reproduces the subendothelial layer. In addition, either ADP or epinephrine is added to the collagen membrane. Initial adhesion to this membrane is induced by a high shear rate (>5,000 s–1) of capillary-tube flow and is mediated by GPIb-VWF interactions. The subsequent release of platelet granule contents in the presence of agonists, such as epinephrine or ADP, on the membrane result in platelet aggregation. A platelet plug is eventually formed occluding the aperture of the membrane and stopping the blood flow. The test is a simple and rapid point-of-care assay and a potential screening tool for assessing hemostatic abnormalities.
In fact, although the original in-vitro bleeding test suffered from poor reproducibility and was inconvenient for clinical use, these difficulties were resolved by the introduction of the PFA-100/200® system, displaying a perceivable clinical efficacy for the screening of von Willebrand Disease (VWD) and platelet function disorders, and possibly for anti-platelet therapies as well [39]. The advantages of this system include user-friendliness and a high sensitivity to conditions affecting primary hemostasis, which is defined as the formation of the primary platelet plug. However, its major limitation is that the results of the closure time (CT) test are neither predictive of, nor specific for, any individual disorder [40].
Impact, the cone and plate(let) analyzer
The cone and plate(let) analyzer (Impact, Matis Medical, Brussels Belgium) measures platelet adhesion to the subendothelium, or a similar surface, under rotating shear flow conditions [41]. The cone and plate apparatus, which is commonly adopted for rheological measurements, induces uniform shear flow in the entire space between a stationary plate and a rotating cone. Application of a uniform shear flow (1,800 s–1) to the blood sample results in platelet activation, adhesion, and aggregation on the plate surface. By staining the platelets and using an image analyzer, the percentage of surface covered by the stained objects and the average size of the objects (per μm2), reflecting platelet adhesion and platelet aggregation, respectively, are determined.
Global thrombosis test
The global thrombosis test (GTT; Montrose Diagnostics Ltd, London, UK) assesses platelet function using whole blood in the absence of an anticoagulant [42]. Blood flow driven by gravity goes through two-step slits formed between two ceramic balls and a conical plastic tube. Flow through the first slit generates relatively high shear rates, activating the platelets. In the space after the first slit, a low shear flow facilitates platelet aggregation. Subsequently, aggregated platelets adhere to the entrance of the second slit. As the second slit is gradually occluded, the time interval between two consecutive drops increases. A time interval between drops longer than 15 s is considered as the occlusion time. In the second phase, coagulated blood is lysed and blood flow resumed. This is recorded as the lysis time (seconds). As the test uses non-coagulated blood, thrombotic status can be determined without adding calcium. The correlation between the GTT results and clinical outcomes is still under evaluation [43, 44].
Total thrombus-formation analysis system
The total thrombus-formation analysis system (T-TAS; Fujimori Kogyo Co., Tokyo, Japan) is an automated microchip flow chamber system that quantitatively analyses thrombus formation under blood flow. Using a precision injection molding technique, two types of single-use plastic microchips have been developed for evaluating platelet-specific and comprehensive thrombus formation under variable blood flow conditions [45]. A blood sample driven by a micropump flows at high shear rates through collagen-coated multichannels. Owing to the high shear rates, the platelets become activated and adhere to the surface. Platelet thrombus formation in the flow chamber is continuously monitored by a video microscope and a pressure sensor that tracks pressure changes in the flow path. The platelet aggregates gradually increase in size and eventually occlude the capillary, resulting in enhanced flow pressure. Therefore, the flow pressure patterns reflect platelet thrombus formation.
Comparative evaluation of POC assays
As described above, many point-of-care testing (POCT) devices have been recently introduced and some of them (i.e., PFA-100, VerifyNow System, Multiplate Electrode Aggregometry [MEA]) are now widely used in clinical settings. These devices are based on leading-edge technologies which may be used both in critical clinical settings and in standard laboratories because they are rapid and easy to use, employ whole blood, and do not implicate sample processing. For instance, VerifyNow does not require any pipetting for blood sample loading but insert a test kit into a system. By eliminating pipetting in the sample loading process, the systems allow the operator to handle blood very easily. Also, most POCT can be conducted in only 5–15 min allowing for the examination of dozens of blood samples a day.
However, despite the significant improvements in both usability and reproducibility, clinicians are not satisfied with the current devices, owing to a number of serious intrinsic problems, as mentioned below). First, a poor correlation is observed between the results obtained with different POC devices [3–5, 32–32]. In a recent study [5, 9], we reported a poor pairwise agreement, as assessed by Cohen’s kappa coefficient and kappa values, between three platelet function assays, PFA®, Multiplate®, and Plateletworks, employing the same agonist. Of course, these devices were compared with a gold standard device such as LTA at the time they were introduced. The specific measurement of platelet function for a given device should be interpreted with caution based on a detailed understanding of the device characteristics. In fact, the observed discrepancies are mainly due to differences in methodological details [30, 30]. For instance, the characteristic length scale in a sensor would give different results even at the same device [28], as is discussed in section 4.5. Thus, the poor correlation between POC devices should be carefully addressed in the development of future systems.
Another major problem related to POC devices is the gap between test results and clinical outcomes. In a prospective, observational, single-center cohort study of 1069 consecutive patients taking clopidogrel and undergoing elective coronary stent implantation, three devices failed to discriminate between patients with and without primary endpoint at 1-year follow-up [2]. The VerifyNow assay showed a strong potential to predict adverse outcomes in patients with acute coronary syndromes (ACS) [46]. Of course, for some of the above-mentioned devices, the results showed a good association with platelet dysfunction, but none of them was able to provide accurate prognostic information to distinguish low-risk patients from patients at high risk of experiencing bleeding or ischemic events [2].
One potential cause of the problem is the inclusion of anticoagulants, lowering calcium level. In citrated blood at critically low [Ca2+], the physiological response of platelets to various agonists such as thrombin cannot be considered [44]. In fact, thrombin can induce significant platelet granule secretion (ADP release, TXA2 formation). Another issue is that conventional tests of platelet function do not consider thrombolysis. Thus, thromboelastography (TEG) and GTT devices are designed to examine both thrombosis and thrombolysis. A recent study reported that an impaired thrombolytic status is predictive of adverse cardiac events in patients undergoing primary percutaneous coronary intervention [47]. Therefore, the results obtained with current POCT devices need to be monitored along with clinical correlations.
Moving microfluidics into clinical application
As microfluidics can mimic the atherosclerotic confinement of vessels and physiological shear rates and gradients, numerous studies have examined human whole blood using these technologies in combination with extracellular matrix surface coatings. Several excellent reviews covering different aspects of these technologies are available [48–52]. Also, there are several good practical, ‘how-to’ and best practice articles that readers interested in testing platelet function in microfluidics should consult [53–57]. This section briefly describes the advantages of the microfluidics approach for platelet assays.
Figure 2 depicts typical configurations of platelet assays with microfluidics. Figure 2(a), shows a schematic of microfluidic channels for collagen coating onto a glass slide (top left) and a microfluidic device to measure platelet function (bottom left). A micro-channel coated by collagen is represented in green and a channel for blood perfusion is labeled in red, with arrows indicating flow direction. A device with 13 micro-channels for the analysis of blood flow experiments is shown on the right [58] Fig. 2(b) shows a microfluidic device with a specific channel geometry with collagen and TF(tissue factor) coating (dark area).
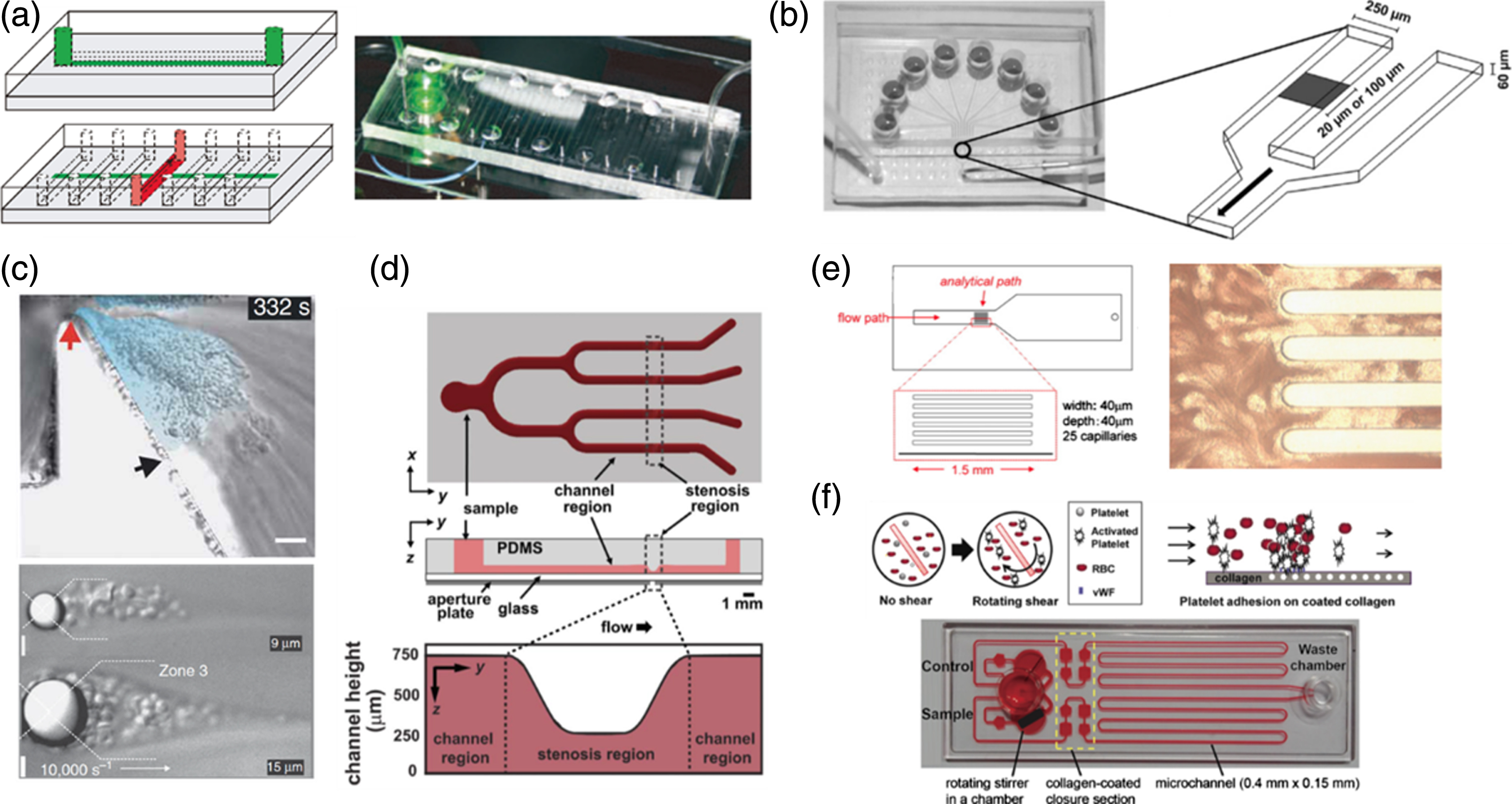
Microfluidic devices to measure platelet thrombus formation under physiologic and pathologic conditions. (a) microchannels for collagen coating onto a glass slide, reproduced with permission from J. Thrombosis and Haemostasis 6, 2193 (2008), (b) Various channel geometries with collagen and TF coating, reproduced with permission from Biophysical J. 114, 978 (2018, (c) Microfluidic geometries with severe stenosis facing high shear gradient, reproduced with permission from Nature medicine 15, 665 (2009), (d) A microfluidic chip including a stenosis region, reproduced with permission from PLoS One 9, e82493(2014), (e) a microfluidic chip with 25-capillaries and thrombus formation on a collagen-coated surface, reproduced with permission from Microvascular research 83, 154 (2012), and (f) a microfluidic chip for platelet function test with measuring migration distance of blood sample through a microchannel, reproduced from [H. Lee, G. Kim, C. Lim, B. Lee and S. Shin, Biomicrofluidics 10, 064118 (2016)], with permission of AIP Publishing.
The device is reversibly attached to a glass under vacuum pressure. The arrow indicates the direction of blood flow [59]. In Fig. 2(c), microfluidic geometries with severe stenosis facing a high shear gradient. When flow direction was left to right, platelets were preferentially aggregated in low-shear zones after stenosis (top) and after round pillar (bottom). The red and black arrows in the top figure indicate the initiation and end of the thrombus formation, respectively [60]. Figure 2(d) depicts a microfluidic chip including a stenosis region and detailed section views. Channels with various heights can be subjected to reproduce various shear conditions, including physiological as well as pathological conditions [61]. Figure 2(e) shows a microfluidic chip with 25-capillaries (left) and the formation of a thrombus on a collagen coated surface after a 7-min blood perfusion (right). Blood sample flowed from left to right at a shear rate of 1,500 s–1 [62]. Finally, Fig. 2(f) demonstrates shear-induced platelet activation (top) and shows a microfluidic device for platelet function test using a rotating shear flow generated by a rotating stirrer (bottom). In this device, platelet function was determined by evaluating the migration distance through the microchannel, which was occluded so as to mimic thrombus formation onto a collagen-coated area [63].
Microfluidics-based platelet function tests have various advantages, including the ability to mimic the pathophysiological environment and the structure of injured blood vessels. Numerous microfluidics studies have examined platelet function and coagulation using extracellular matrix surface coatings [64–67]. Successful microfluidics assays require elaborate patterning of proteins, such as collagen [59, 68–70], TFs [70], and vWF [71], or even ECM [72]. A simple dipping and rinsing method can be used to pattern microchannels, but this approach has several limitations, including lack of homogeneity and reproducibility. Therefore, researchers have focused their efforts in developing more sophisticated patterning techniques.
Using a microarrayer, microcontact printing can be used to generate microspots (176μm diameter) of adsorbed protein on a glass substrate [64]. To mimic distinct thrombotic regions, collagen is patterned on a 250μm-wide stripe on the microchannel surface. Here, additional coatings with biotinylated anticollagen antibody, biotin, and streptavidin allow for the subsequent capture of TF liposomes. Fibrinogen has also been successfully patterned onto glass substrates using the polydimethylsiloxane (PDMS)-stamping technique [65, 66]. Endothelial cell coatings have also been described in the literature [67]. Using the above-mentioned local protein-patterning techniques, a microfluidic focal thrombosis model was developed and used to analyze platelet adhesion and stability on a micropatterned surface of collagen in a PDMS-glass microchannel [58]. Platelet adhesion and aggregation at this focal collagen region can be visualized by epifluorescence microscopy.
The selection of coat components including proteins is an important issue and depends on the purpose of the test. For instance, in bleeding tests, vessel injury must be reproduced and, therefore, collagen is the most appropriate choice. For this reason, PFA200 adopts collagen as the main protein coating the porous membrane for bleeding tests. For platelet aggregation tests in a bloodstream, fibrinogen is the most suitable protein, as is the case with VerifyNow. In Table 2, we summarized the different proteins that can be used in microfluidic platelet assays, depending on the purpose. Moreover, two or three different coat components may be combined for specific tests. For instance, the VerifyNow P2Y12 test adopts two coat components in a blood sample chamber: one is ADP as an agonist and the other is PGE1 as an antagonist.
Microfluidics assays for platelet function tests
Microfluidics assays for platelet function tests
As described, agonists (e.g., ADP, epinephrine, AA, and thrombin) are released from the injured vascular surface and platelets. In in vitro studies, the release of agonists is critical for mimicking pathophysiological environments. Microfluidics can provide agonist release patterns similar to those typical of the in-vivo environment. For instance, PFA-200 utilizes a porous membrane coated with agonists, such as ADP and epinephrine. When blood contacts the agonist-coated membrane, agonists can be easily dissolved. Most microfluidics devices utilize surface coating of agonists on different substrates, such as glass, PDMS, porous membranes, and various plastic plates. In our studies, an agonist was carefully selected for a specific test and used to coat the plastic surface of blood chambers. Most agonists exhibit good water solubility and are easily dissolved into the blood. However, a mixing mechanism may be required to ensure efficient solubilization of agonists in blood. Therefore, a stirrer may be adopted in blood chambers for proper mixing [73, 63].
Microfluidics can use liquid agonists in flowing environments reproducing in vivo blood flow. For instance, two parallel microchannels have been designed, connected via a porous membrane, with a controlled agonist flow from the bottom to the top channel [74]. The mixing of liquid agonists and blood, also based on diffusion and convection, allows for more rapid and precise platelet responses, as compared to the diffusive mixing of solidified agonists on a surface.
Surface coatings with solid agonists often result in delayed responses due to slow solubilization in blood, compared to liquid agonists. We also experienced a difference in the time of platelet activation between solid and liquid agonists, as liquid agonists are faster and more effective. Furthermore, since surface-coating agonists are greatly affected by oxygenation and storage temperature, robust and reproducible protocols should be designed for studies based on microfluidics prior to performing the main tests.
Vascular similarity: Control of flow dynamics
A major requisite of microfluidics used in platelet assays is the ability to replicate in vivo hemodynamic environments. For instance, extreme flow conditions in microfluidics can be easily reproduced by pathological vessel geometries or mechanical assist devices [21, 12]. Physiological shear flow conditions can be effectively simulated by varying either the microchannel dimensions [75, 61] or the driving pressure [40, 76]. There are two types of driving forces, i.e., constant flow rate and constant pressure.
Syringe pumps generate a constant flow rate in which a growing thrombus causes large pressure drops without affecting the flow rate [45]. Conversely, the use of a pressurized (or vacuum) chamber in a large volume can provide a constant driving pressure in which the growing thrombus reduces the flow rate [73, 61]. For instance, the PFA-200 utilizes a constant driving pressure and the decrease in flow rate is monitored [40], whereas the T-TAS adopts a constant flow rate, thus monitoring the increase in pressure [45].
In order to mimic in vivo peripheral artery environments, constant blood flow rate would be the most physiological condition for ensuring oxygen delivery to tissue, rather than constant pressure. When blood flow decreases due to platelet thrombus generation, peripheral blood vessels dilate to maintain a constant flow rate. However, in vitro constant flow rates cannot mimic the vascular tonic control and lead to excessive pressure due to the reduced cross-sectional area of microchannels. In this case, the results of platelet tests would be strongly affected by the vWF function. Although microfluidic studies did not pay much attention to flow conditions, most studies adopted a constant flow rate rather than a constant pressure because of the adoption of the syringe pump system. In recent studies we adopted a constant vacuum pressure, by which the flow rate gradually decreased over time, eventually stopping the fluid flow through the microchannels [63].
Vascular similarity: Hemodynamic shear rate/stress
An important hemodynamic parameter is the shear rate, which greatly affects platelets and other blood cells. Shear rate in a circular vessel is defined as the velocity gradient at an arbitrary radius. In general, the maximum shear rate occurs near the wall, and velocity significantly changes in the radial direction. The circular lumen is replaced with a rectangular microchannel because of fabrication constraints, but the shear rates in the microchannel are similar to those of a circular blood vessel. The shear rates in microfluidics can be controlled by varying either the dimensions of the channel or the driving pressure.
In the physiological circulation, platelets experience a wide range of shear rates. Typical ranges of (wall) shear rates are 20–200 s–1 for veins, 300–800 s–1 for large arteries, 500–1,600 s–1 for arterioles, and 800–10,000 s–1 for atherosclerotic stenosed arteries [21]. The corresponding shear stress ranges are 0.08–0.8 Pa in the venous circulation, 1–6 Pa in the arterial circulation, and 3–38 Pa for stenosed arteries [21]. Generally, high shear rates (>5,000 s–1) or high shear stress (>8 Pa) are employed to induce platelet activation (SIPA) and aggregation [16, 77]. Similar SIPA results were also confirmed in our previous studies [63, 73].
In microfluidic devices, typical hemodynamic shear rates at either venous or arterial walls (100 s–1 or 1000 s–1) can be produced in a straight channel [16]. Furthermore, pathological shear conditions were obtained by mimicking the stenotic vessels, using a specific microchannel dimension [78, 79] and rotational shear flow [63, 80]. Therefore, shear-dependence of platelet adhesion to blood vessel walls can be easily examined in microfluidic devices [61, 81]. Severe stenosis can be conveniently modeled using microfluidics to induce a high shear rate (>20,000 s–1). Also, platelet aggregation can be observed in post-stenosis areas [60]. A few studies also showed how shear gradients affect VWF function, and thus platelet adhesion [20, 82].
Geometric factors in microfluidics
Considering the size of platelets (2–3μm), the general dimensions of microfluidics (50 – 500μm) are sufficiently large to allow for both platelet adhesion and platelet-platelet aggregation [8–11]. Nevertheless, both section size and the geometry adopted in microfluidics may strongly affect the platelet function tests. In a previous study, the ratio of platelet-platelet to platelet-surface interactions, R, and the percentage of platelet-platelet interactions, P, were investigated in microfluidic test sections [28]. The results showed that the test section geometry strongly affects both R and P, with the test section height in low aspect-ratio channels or diameter greater than 90μm being dominated by platelet-platelet interactions (R > 10). With the increase in channel dimensions, R rises linearly while P asymptotically approaches 100 %. Thus, the size of a microfluidic test section should be carefully considered in relation to the purpose. For instance, a rectangular channel with a high aspect ratio (≥10) requires a 50μm section to assay platelet-platelet aggregation [28]. Notably, if the characteristic length of the test section is smaller than the above values, platelet adhesion, rather than aggregation, will be predominantly observed.
In general, thrombotic occlusion is the result of platelet adhesion followed by aggregation [78]. These two sequential events are frequently analyzed as a unique process, without distinction. However, depending on size and geometry, one mechanism will predominate over the other. For instance, PFA-200 assays implicate an initial platelet adhesion followed by platelet aggregation to simulate thrombotic occlusion. Considering the diameter of the PFA membrane hole (150μm) [39], which is greater than the critical value (90μm), platelet aggregation is dominant over platelet adhesion. On the other hand, when the typical height of a microchannel ranges from 40 to 80μm, as is the case with T-TAS [62], platelet adhesion is dominant over platelet aggregation.
Effect of temperature
Since platelet activation, adhesion, and aggregation require multiple enzymatic reactions and cellular activities, the susceptibility of these processes to the environmental temperature is not surprising. Interestingly, temperature exerts distinct effects on platelet aggregation and for activation pathways and agonists. In fact, SIPA is significantly more efficient at 24, 32, and 35°C compared to 37°C, both in whole blood and in platelet-rich plasma [83]. On the other hand, the aggregation induced by collagen, ristocetin, and arachidonic acid (AA) does not differ significantly at test temperatures of 34 and 37°C but is significantly impaired at 22°C. By contrast, ADP-induced aggregation is significantly increased at both 34 and 22°C compared to 37°C [84]. Therefore, to avoid conflicting results, all in vitro measurements in platelet assays should be performed at a standard temperature of 37°C [85].
Selection of anticoagulants
Although a careful selection of the appropriate anticoagulant is an absolute prerequisite [44], the ideal anticoagulant for accurate platelet function tests remains controversial [86]. Typical anticoagulants used include citrate, heparin, EDTA, and hirudin. The use of phosphate buffers should be avoided, as they result in the formation of calcium phosphate precipitates. For hemodynamic studies that are not focused on coagulation or platelet function, EDTA is an ideal inhibitor of thrombin production and platelet adhesion. Commonly known as a calcium chelator, EDTA substantially attenuates αIIbβ3 function [87]. For measuring platelet function, thrombin inhibitors such as PPACK or hirudin are preferable since they do not alter cation concentrations [88]. Once established that these are the ideal options, citrate remains the most commonly used anticoagulant for clinical platelet function tests. It is worthy to note that citrate significantly impairs αIIbβ3. Moreover, citrate chelates not only Ca+but also Mg2+and Zn2+ions [89].
Notably, when blood is withdrawn from veins, the first 5 mL are usually discarded to avoid tissue factor contamination during venipuncture. Also, the drawn blood should not be shaken on an automatic roll-mixer or similar device, but rather gently mixed by hand for one minute. When transport over long distances, and even within the same hospital, is required, samples should be carefully handled to avoid strong shaking. Furthermore, the test should be completed within 2 hours after the blood is drawn [86]. Should this not be possible, a maximum of 4 hours should be recommended as a workaround.
Detection methods
There are numerous detection methods available for analyzing platelet adhesion and aggregation. Both light transmission aggregometry and VerifyNow utilize optical turbidometry, whereas Multiplates uses electric impedance spectroscopy [46]. Both turbidometry- and impedance-based methods rely on the area under the curve. The Impact system uses optical fluorescent intensity and direct microscopy image analysis and is the most widely adopted microfluidics approach. In this case, the area of platelet adhesion to a surface and the fluorescence intensity are the main parameters analyzed. On the other hand, both PFA-200 and T-TAS are based on the relationship between flow rate and pressure and measure the time until flow passage is blocked due to platelet aggregation.
In Table 2, various microfluidic assays for platelet function tests are categorized based on the detection method, the flow-driven method, as well as other parameters. Most studies of microfluidics rely on the measurement of fluorescent area and intensity. Also, most of these studies employed a constant flow rate with a syringe pump. However, several other studies rely on non-fluorescent detection methods, including measurement of the closure time with the simultaneous monitoring of pressure or flow rate [45, 90].
Our recent studies have introduced the measurement of the migration distance through a microchannel until flow passage occlusion as an estimate of platelet aggregation [63, 73]. This is represented in Fig. 2(f), showing a blood sample mixed with agonists in a sample chamber entering the main section of the collagen-coated microchannel. As activated platelets adhere on the collagen surface, the flow passage narrows and is eventually blocked by platelet aggregation. Therefore, the distance from the entrance to the final stop position of the blood sample is defined as migration distance (MD). The MD through the microchannel was determined from images captured every 0.1 s by a CCD camera. A few hundreds of images were analyzed by a computer, and the MDs were determined within a second. Owing to the resolution of the image sensor (CCD), the migration distance was precisely measured by counting the number of pixels along the centerline of microchannels. Furthermore, the time-varying velocities and flow rates could be calculated based on the MD over time.
Conclusions
There have been significant advances in the analysis of platelet function and thrombosis kinetics using microfluidics-based technologies. This is mainly due to the advantages of the microfluidics platform, which can mimic vascular environments and serve as small-scale integrated sample-to-answer systems. In these systems, vascular environments are mimicked through the patterning of subendothelial proteins on specific surfaces, stenosed geometry, the use of shear flow in the in vivo range, and the accumulation of platelet thrombi on injured surfaces.
However, there are still unmet clinical needs for platelet function tests. The major question is whether the test results are correlated with clinical outcomes. For instance, platelet function tests yielded stable and safe results for patients with thrombotic risk, who eventually experienced thrombotic events [6]. A recent article criticized the fact that the conventional devices cannot discriminate between preoperative or referred patients with and without mild platelet function disorders [30]. Of course, thrombosis cannot be predicted only with platelet function tests. This is a good indication of the current status of platelet function tests. Thus, new solutions to predict thrombotic events are urgently required.
In the present review, we confirmed that platelets play an essential role in thrombogenesis but are only one component of a complex mechanism. Thus, a comprehensive test should be developed, allowing for the delineation of multiple contributing processes. Another unsolved issue is the assessment of thrombolytic activity after the occurrence of thrombosis. Although not addressed in this paper, it is of note that some of the rheometric devices such as TEG and ROTEM can analyze thrombolytic characteristics in the blood of patients. Thus, the development of an innovative microfluidic method to test thrombolytic activity is highly desirable.
The microfluidics approaches for assessment of platelet functions could be further enhanced by a comprehensive understanding of platelet biology as well as the mechanisms operating in microfluidics environments. Although this review is limited to the description of platelet aggregation and function tests, many extensive studies have already been conducted on platelet drug screening and thrombus formation using microfluidics [48–52]. Therefore, in future studies, a thorough comprehension of microfluidics will allow for an exhaustive assessment of platelet pathophysiology.
Footnotes
Acknowledgments
This research was supported by a National Research Foundation of Korea Grant funded by the Korean Government, MSIP (2016R1A5A1010148) and the Korean Health Technology R&D Project, Ministry of Health and Welfare (No. HI14C0670).