
Abstract
BACKGROUND AND OBJECTIVES:
Early persistent facial paralysis is characterized by intact muscles of facial expression through maintained perfusion but lacking nerve supply. In facial reanimation procedures aiming at restoration of facial tone and dynamics, neurotization through a donor nerve is performed. Critical for reanimating target muscles is axonal capacity of both donor and recipient nerves. In cases of complete paralysis, the proximal stump of the extratemporal facial nerve trunk may be selected as a recipient site for coaptation. To further clarify the histological basis of this facial reanimation procedure we conducted a human cadaver study examining macro and micro anatomical features of the facial nerve trunk including its axonal capacity in human cadavers. Axonal loads, morphology and morbidity of different donor nerves are discussed reviewing literature in context of nerve transfers.
METHODS:
From 6/2015 to 9/2016 in a group of 53 fresh frozen cadavers a total of 106 facial halves were dissected. Biopsies of the extratemporal facial nerve trunk (FN) were obtained at 1 cm distal to the stylomastoid foramen. After histological processing and digitalization of 99 specimens available, 97 were selected eligible for fascicle counts and 87 fulfilled quality criteria for a semi-automated computer-based axon quantification software using ImageJ/Fiji.
RESULTS:
An average of 3.82 fascicles (range, 1 to 9) were noted (n = 97). 6684±1884 axons (range, 2655– 12457) were counted for the entire group (n = 87). Right facial halves showed 6364±1904 axons (n = 43). Left facial halves demonstrated 6996±1833 axons (n = 44) with no significant difference (p = 0.73). Female cadavers featured 6247±2230 (n = 22), male showed 6769±1809 axons (n = 40). No statistical difference was seen between genders (p = 0.59). A comparison with different studies in literature is made. The nerve diameter in 82 of our specimens could be measured at 1933±424 μm (range, 975 to 3012).
CONCLUSIONS:
No donor nerve has been described to match axonal load or fascicle number of the extratemporal facial nerve main trunk. However, the masseteric nerve may be coapted for neurotization of facial muscles with a low complication rate and good clinical outcomes. Nerve transfer is indicated from 6 months after onset of facial paralysis if no recovery of facial nerve function is seen.
Keywords
Introduction
The facial nerve is a key promoting nerve to transduce voluntary and involuntary human emotions into facial expressions [1]. Linking the brain with 21–24 mimic muscles the facial nerve mediates important verbal and non-verbal communication from the individual subject to its human environment [2]. Facial expression may be divided into 6 categories: sadness, anger, joy, fear, disgust, and surprise. Dysfunction of the VII. Cranial nerve in contrast, may cause severe impairments including asymmetry of facial expressions, limited eye closure, oral incontinence, dysarthria and social limitations [3]. Sequalae suffered from persistent malfunction of the facial nerve may successfully be eased with modern plastic surgical nerve transfers, direct neurotization, cross-face-nerve-grafting (CFNG) and free functional muscle transplants to re-establish facial dynamics in early persistent and chronic cases [4–7]. Introduced by Scaramella and Smith in 1971 an important step in facial reanimation surgery was taken with cross-face-nerve-grafts (CFNG) aimed at reducing these symptoms [8–10]. Early persistent facial paralysis is characterized by an irreversible palsy of the facial nerve, thus lacking neural stimuli for mimic musculature but muscular perfusion is still intact [11–13]. This transient condition is accessible to nerve transfers and cross-face-nerve-grafting re-establishing facial dynamics in function and symmetry. Usage of a new motor source to reanimate an existing muscle (i.e. through cross-face nerve grafting or masseter nerve transfer) is termed “neurotization” [14]. Critical for reanimating target musculature is axonal capacity of donor and recipient nerves [15]. “Axonal capacity” or “axonal load” are defined by the number of axons found in a histological cross section of one specific nerve branch.
The facial nerve itself is known to show great variety in its arborization pattern. Selective coaptation of CFNG to distal branches in order to regain ocular and oral functions have been described [16, 17]. In favor of using precise terminology to distinguish zygomatic and buccal branches in their transition zone a new clinically oriented anatomical definition was recently suggested by Kehrer et al. defining any branch topographically lying clearly superficial to the zygoma or touching it as a zygomatic and any inferior neighboring branch as buccal of origin [18].
However, in cases of complete paralysis and certainty that the proximal stump of the facial nerve will remain dysfunctional e.g. after ablative tumor treatment, transection through temporal bone trauma, permanent Bell’s palsy (idiopathic facial paralysis) or cases with no option for anastomosis, a suitable donor nerve may be coapted to the distal stump of the facial nerve trunk for successful neurotization of mimic muscles.
To further clarify the histoanatomic basis of this facial reanimation procedure we conducted a human cadaver study examining macro and micro anatomical features of the facial nerve trunk including its axonal capacity in a large series of human cadavers. Comparing axonal loads an in-depth look into literature is undertaken for possible donor nerve branches to the facial nerve trunk.
Material and methods
From 6/2015 to 9/2016 in a group of 53 fresh frozen cadavers a total of 106 facial halves were dissected at Departments of Anatomy, University Medical Center Utrecht/The Netherlands, University of Halle/Germany, University of Graz/Austria and University of Regensburg/Germany. All human specimens were derived from bodies that entered the Departments of Anatomy through a donation program. From these persons written informed consent was obtained during life that allowed the use of their entire bodies for educational and research purposes. Institutional review board approval was obtained. Nerve biopsies of the extratemporal facial nerve trunk were available from 99 specimens. Strict quality of the histological cross-sections for inclusion into the study were defined including complete staining of the entire cross-section area, full exposure of the section on the histological slide and entirely orthogonal cuts of the nerve branch cross-section with respect to its longitudinal axis showing a clear image of orthogonally cut axons. Of 99 specimens available, 82 were suitable for measuring nerve diameter, 97 were eligible for fascicle counts and 87 histological sections fulfilled all quality criteria and were included into the axon quantification method of this study. The gender of human cadavers was known in 62 cases. For the remaining 25 facial halves gender identification was not possible. The study was approved by the Institutional Review Board Committee of the University of Regensburg and is designed in accordance with the Helsinki Declaration. The manuscript complies with the ethical guidelines of Clinical Hemorheology and Microcirculation [19].
Surgical dissection of human cadavers
Dissections were performed under 4x-loupe magnification and using fine surgical, as well as microsurgical instruments. Following a pretragal incision, cranially extended beyond the hairline and caudally below the angle of the mandible, skin flaps were undermined to the nasolabial fold beyond the medial border of zygomatic muscle (ZM). After identification of the main trunk of the extracranial facial nerve at the tragal pointer [20] a hemiparotidectomy was performed and followed by an antegrade microsurgical preparation of all facial nerve branches except the cervical branch in the sub SMAS plane. A biopsy of the facial nerve trunk was taken 1 cm distal to the stylomastoid foramen.
Histological processing, digitalization, axonal quantification and measuring diameter
Facial nerve trunk biopsies were first fixated in a modified EM-fixation solution described by Ito und Karnovsky [21]. The fixation is comprised of 2.5% PFA and 2.5% glutaraldehyde. The pH-value is then controlled and adjusted to 7.4 if necessary.
After a time period of 12–24 hours the fixation solution is eliminated a 0.1M natriumcacodylat-buffer. Secondary fixation is done with osmium ferrocyanide for 2.5 hours. This is followed by rinsing the biopsies with bidest. water. Gradually EtOH and later Acetone are added in several steps to dehydrate the specimens. Finally, the biopsies are embedded in Epoxy Resin (EPON H). Polymerization is achieved by incubating at 60°C for two days with infiltration of 100% EPON H. Semi-thin sections (1 μm) were cut with a microtome using a diamond blade performing 16 slices. These are dried overnight and stained with PPD (p-phenylenediamine) for 30 minutes.
After drying the specimens were digitalized using a digital microscope (Zeiss, model Axio Imager Z1) with objectives Zeiss EC Plan-Neofluar 5x/ 0.15; ∞/ 0.17 and Zeiss Plan-APOCHROM AT 20x/ 0.8; ∞/ 0.17 as well as Okular E-PL 10x/25 Br. foc. Using the „Zeiss Axio Cam MR“ camera sections were digitalize at optimal lighting of 3200K and transferred with software „Axio Vision 4.8 (6-2009)“ on a computer system (Fujitsu-Siemens). Digital picture material was first saved as „Carl Zeiss Vision images“ (*.zvi) and subsequently converted to „Tagged Image Files“ (*.tif) with Axio Vision 4. Grey color pictures in 200x magnification of each section were obtained for axon quantification. Table 1 provides an overview of histological processing of facial nerve trunk biopsies. Axonal load was determined through manual count and a semi-automated computer-based method using a specialized axon quantification software ImageJ/Fiji programmed to simplify nerve morphometry [22]. Fascicles were counted manually. The diameter (in μm) of nerve cross-sections including epineurium was measured with Zeiss AxioVision Microscope Software using the mean of two orthogonal vectors. The software was first calibrated under 2.5x magnification. Slides with poorly defined edges or lacerations were excluded.
Histological processing of facial nerve trunk biopsies
Histological processing of facial nerve trunk biopsies
Statistical analysis was performed with SPSS (IBM Corp. Released 2010. IBM SPSS Statistics for Macintosh, Version 19.0. Armonk, NY: IBM Corp.).
Several fascicles were noticed in all almost all specimens. Of 97 histological sections acceptable for counts an average of 3.82 fascicles (range, 1 to 9) were noted. After exclusion of specimens of insufficient quality, 87 biopsies could be examined for axon quantification. At 1 cm distal of the stylomastoid foramen 6684±1884 axons (range, 2655 to 12457) were counted. 43 specimens were taken from right facial halves showing 6364±1904 axons. Histological sections from 44 left facial halves demonstrated 6996±1833 axons, which showed no significant difference compared to right facial halves (p = 0.73). A subgroup of 22 specimens had been taken from female cadavers showing 6247±2230 axons. The remaining 40 specimens from male cadavers showed 6769±1809 axons. No statistical difference was seen between genders (p = 0.59). The diameter of 82 specimens could be measured at 1933±424 μm (range, 975 to 3012).
Figure 1 illustrates a schematic drawing of the microsurgical basis of masseter-to-facial nerve trunk transfer (V-to-VII-transfer) performed in early persistent cases of facial paralysis.
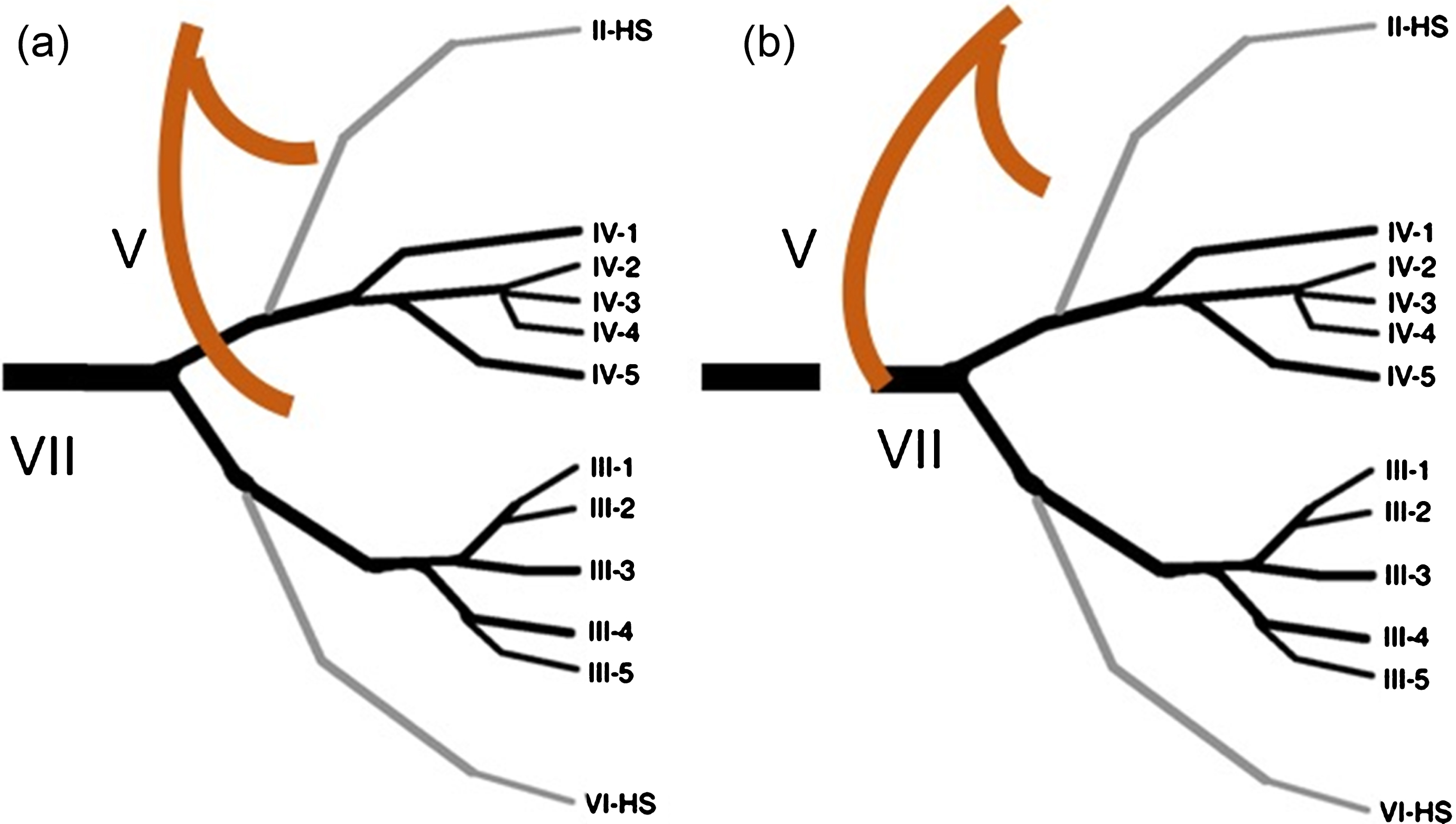
Schematic drawing of V-to-VII nerve transfer. A: The masseteric nerve (V) usually consists of a horizontal and a descending branch. Distal to its main trunk the facial nerve (VII) separates at the pes anserinus into a primary temporozygomatic branch and a primary cervicofacial branch before further branching into 5 subordinated twig systems: frontotemporal, zygomatic, buccal, marginal mandibular and cervical (not depicted). The V. and the VII. Cranial nerve, even though coursing in different tissue planes of the face share a close proximity to each other and may be coapted tensionless. B: In V-to-VII Nerve transfer the distal part of the descending branch of the masseteric nerve (V) is cut. Also, the main trunk of the facial nerve (VII) about 1 cm distal from the stylomastoid foramen to the beginning of its extratemporal pathway is transected. The proximal facial nerve plexus is dissected free performing a superficial hemiparotidectomy. Both nerve stumps are then deflected towards each other and coapted. Additional Cross-face-Nerve-grafts (CFNG) diverting fibers from the contralateral facial nerve to the paralyzed facial half may be used for zygomatic branches to address functions of eye closure and blink as well as elevation of the oral commissure.
Figures 2 and 3 illustrate histological cross-sections of the facial nerve’s main trunk after staining with PPD at 200x magnification demonstrating different numbers of fascicles. Figure 4 shows a histological cross-section of the main branch of the masseter nerve shortly after passing the incisura mandibulae before separating into a descending and a horizontal twig. Table 2 provides an overlook on axon counts found for the facial nerve trunk in literature and compares staining, magnification of specimens, axonal load and number of specimens.

Cross-section of an extratemporal facial nerve main trunk 1 cm distal to stylomastoid foramen. Left facial nerve main branch, in 200x magnification, colored with PPD (p-phenylenediamine) histologic stain and digitalized as a black and white Image with Zeiss Axio Imager Z1. Epi- and perineurium have been removed to eliminate artefacts for nerve quantification. A total of 6227 axons were counted in this this cross section featuring two larger and three smaller fascicles (5 fascicles in total).
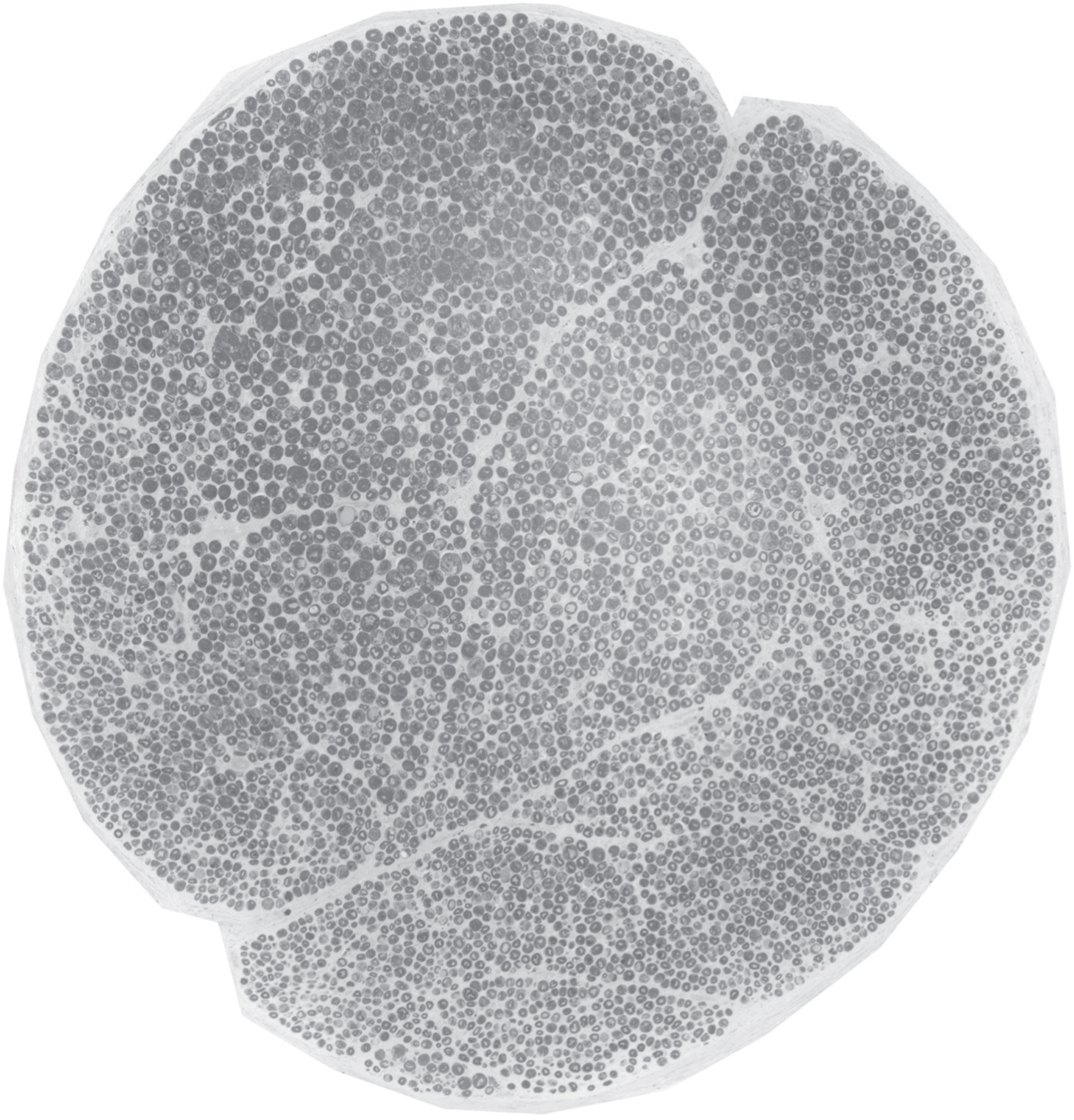
Cross-section of an extratemporal facial nerve main trunk 1 cm distal to stylomastoid foramen. Right facial nerve main branch, in 200x magnification, colored with PPD (p-phenylenediamine) histologic stain and digitalized as a black and white Image with Zeiss Axio Imager Z1. One large fascicle is seen incorporating 5964 Axons.

Cross-section of a masseteric nerve main branch at the level of the incisura mandibulae. Left masseteric nerve main branch, in 200x magnification, colored with PPD (p-phenylenediamine) histologic stain and digitalized as a black and white Image with Zeiss Axio Imager Z1. This cross section was taken from the main nerve branch at the level of the incisura mandibulae before the nerve usually branches off a vertical and a descending twig. In facial reanimation procedures using V-toVII transfer usually the distal end of the descending branch is used for coaptation with no sequalae.
Review of axonal counts of the extratemporal facial nerve trunk in literature
Our study could complement previous studies with a high biopsy count and subgroups of facial side orientation as well as sex. FN = facial nerve.
Figures 5 and 6 provide macroscopical views of the extratemporal facial nerve trunk and the masseteric nerve. A clinical picture of a V-to-VII-nerve branch procedure is shown in Fig. 7 demonstrating the size mismatch of donor and recipient nerve.
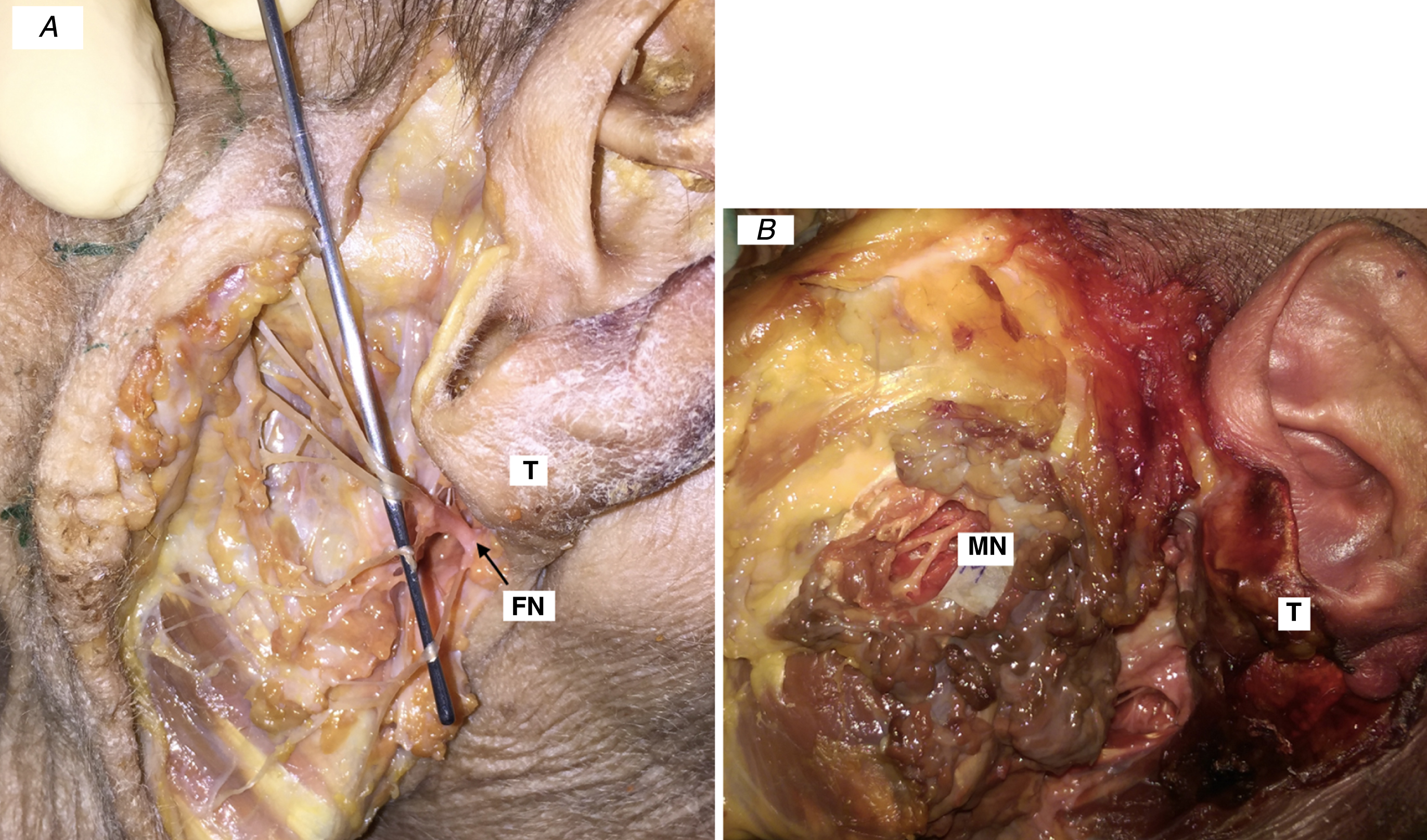
Macroscopical view of the extratemporal facial nerve trunk and masseteric nerve. A: facial nerve: macroscopical view of the extratemporal facial nerve trunk shortly after exiting the styloimastoid foramen. B: Image of masseteric nerve shortly after passing the incisura mandibulae displaying a horizontal and a descending branch in a human cadaver. T = tragus, FN = facial nerve main trunk, MN = massteric nerve.
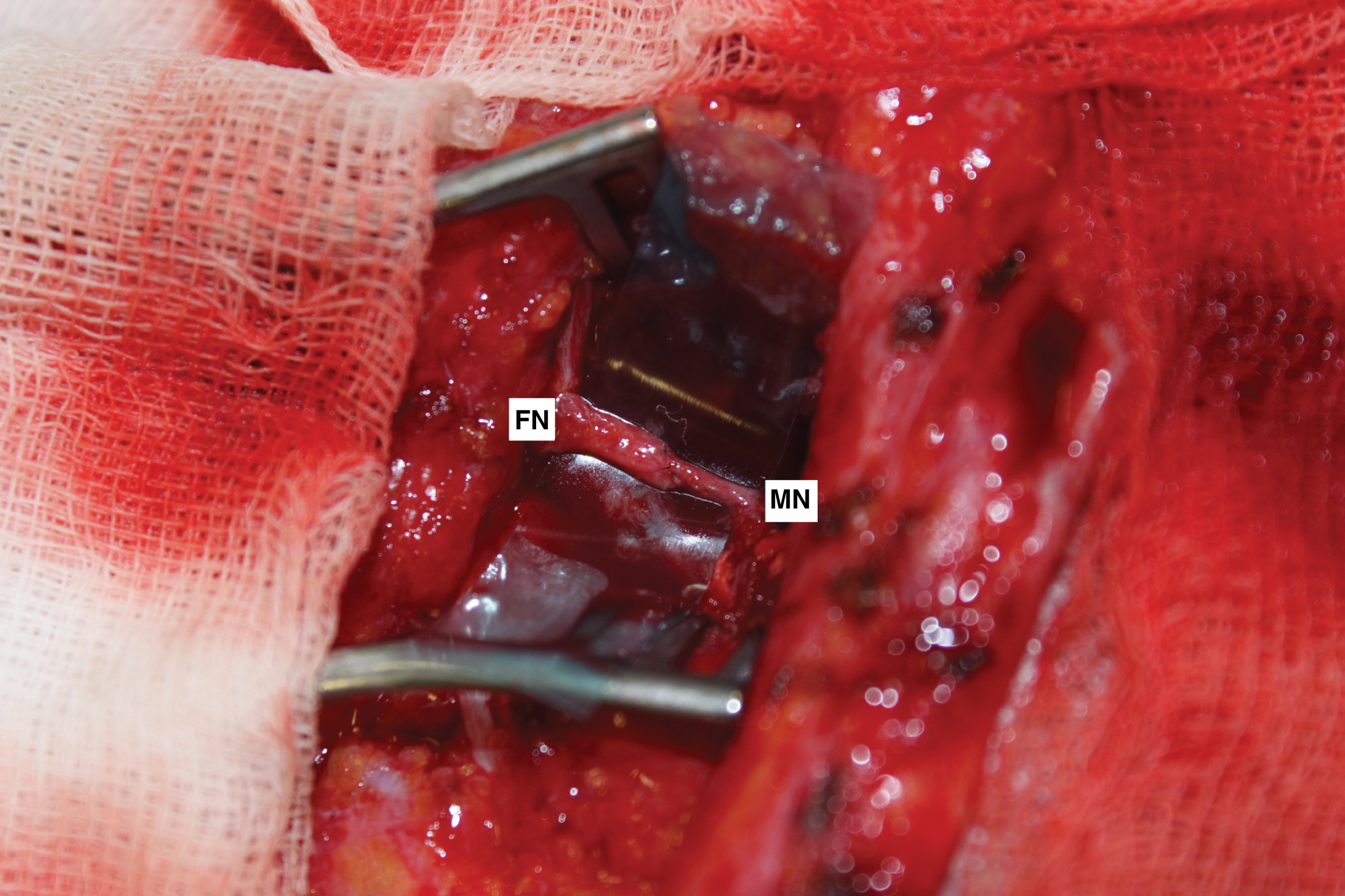
V-to-VII-nerve branch procedure. Clinical picture of a V-to-VII-nerve branch procedure in an early case of persistent facial nerve paralysis after resection of an acoustic neuroma at the skull base in a 47 y/o female patient. Note the differences in diameter of the extratemporal FN trunk (left) and the descending branch of the masseteric nerv (right) after microsurgical coaptation. FN = facial nerve, MN = masseteric nerve.
Facial reanimation procedures in facial paralysis patients have been performed by reconstructive surgeons for centuries [23]. Modern refinements comprise specific detailed nerve transfers, direct neurotization, multiple cross-face-nerve grafts and a variety of donor nerves [24–27]. Through maintaining a continuous blood supply despite denervation in persistent facial paralysis mimetic muscles are capable of being reinnervated possibly for at least 15 months and longer even though their natural stimulus through the facial nerve has persistently been lost [28]. However, a gradually progressive atrophy with degeneration of motor-endplates is seen following denervation [29]. Operative timing has therefore been shifted toward an earlier reconstruction. More recent studies suggest the timing of facial reanimation procedures earlier than in past times, re-encouraging nerve transfers after 6 months after onset of facial paralysis if no recovery of facial nerve function is seen [28, 30–32]. A predictive model using rate of functional improvement as the independent variable was described by Rivas et al. and found to anticipate poor outcome before 1 year in more than 50% of cases with 97% sensitivity and 97% specificity [33]. Consequently, if no recovery in a facial paralysis patient is seen of at least one House-Brackmann grade after 6 months of observation with an anatomically facial nerve in continuity demonstrating a House-Brackmann grade V or worse, an operation for nerve transfer should be planned [34]. Studies have also demonstrated beneficial effects of nerve transfer to the proximal stump of the facial nerve in patients exceeding a time period of 18 months after onset of facial paralysis [35]. Axonal load has a direct influence on the outcome on function [36].
Hypoglossal nerve transfer played an important role for neurotization in the past, however, its use is associated with sequalae as hemilingual atrophy and tongue dysfunction [37]. The hypoglossal nerve transfer was commonly utilized in the past using an interposition nerve graft performing an “hypoglossal jump graft” anastomosis or as a hemihypoglossal transfer [38, 39]. According to Mackinnon and Dellon’s study it could possibly contribute 9202±2182 donor axons [40]. It may also be used in a “babysitter role” coapting the facial nerve trunk in an end-to-side fashion to the nerve as described by Terzis [41, 42].
The spinal accessory nerve has been employed to supply donor axons treating facial paralysis [24, 43]. It may provide an axon capacity of 1394±519 at distal transection level for donor nerve harvesting [44]. However, sequalae as synchronous movements with shoulder elevation and weakness of the shoulder function have been reported [43].
A newer and possibly ideal alternative are masseteric nerve branches for donor nerve supply to mimetic muscles [45, 46]. V-to-VII-transfers have quickly gained an increasingly protagonist role in nerve transfers for neurotization of mimetic muscles [47]. Natural smile results have been reported in literature with masseter nerve transfer [47]. The mechanism made accountable for this competence is thought to be brain plasticity [48]. Some patients can dissociate their smile from jaw-clenching when a branch of the radix motoria by the trigeminal nerve is chosen. Furthermore, even spontaneous smiling has been described with the use of masseter nerve [49]. However, masseter nerve transfer may also have shortcomings, as namely a possible animation deformity while chewing and being less reliable in providing the emotional, spontaneous smile that the facial nerve does powering a functional free muscle flap [48]. However, in a comprehensive review by Murphey et al. overlooking 183 patients masseteric nerve transfer showed low morbidity and relative ease of surgery compared with the other nerve transfers. Only 12 complications were reported in this study. Four patients had masseter atrophy, 2 complained of ocular discomfort with chewing [50]. The risk of synkinesis seems lower with masseteric nerve transfer than hypoglossal [51, 52]. In a pooled analysis by Murphey, facial tone and dynamics have been reported to recover at 5.76 months after V-to-VII-nerve transfers in the in main facial nerve trunk subgroup [50]. Restoration of pleasing resting facial tone with powerful commissure excursion may be expected [47].
In cases of complete facial paralysis, the distal stump of the facial nerve is coapted to the descending branch of masseteric nerve. Masseteric axonal load is described to supply as many as 1500–2700 axons as a donor nerve branch [46, 51]. The microsurgical repair site usually shows an inevitable size and fascicle mismatch. As a clinical rule of thumb, there is a 50% loss of axons at each coaptation site. Thus, approximately only 50% of the original axons successfully regenerate through the repair site [53]. Theoretically, the same number of axons of the donor nerve would be needed to deliver enough axonal load to all facial muscles restoring the original functional properties, however, no known donor nerve is able to supply as much as 6000 axons distal to the coaptation site. Examining peripheral facial nerve branches in an animal model using rabbits Spector et al. could demonstrate that a minimal number of 12% motor axons of the original axonal capacity are needed to innervate mimic muscles [54].
Additionally, comparing fascicles and axonal capacity in both, donor and recipient nerve stumps, incongruent numbers have to be expected. The facial nerve incorporates several fiber qualities including branchial motor (muscles of facial expression, posterior belly of digastric muscle stylohyoid muscle, stapedius muscle), visceral motor (salivation— lacrimal, sub-mandibular, and sublingual nasal mucosa or mucous membrane), general sensory (sensory to auricular concha external auditory canal tympanic membrane) and special sensory (chorda tympani nerve— taste to anterior two-thirds of the tongue) [55].
In our study, we could examine 3.82 fascicles in the facial nerve trunk. Consequently, in V-to-VII nerve transfer several facial nerve fascicles carrying different fiber qualities receive axonal input from a monofaszicular masseteric nerve carrying exclusively motor fibers. Relevant for microsurgical repair, Kempe et al. had described three major divisions into fascicles: the orbicularis oris muscle (fascicle 1), orbicularis oculi muscle (fascicle 2), and the remaining mimic musculature (fascicle 3) by electrical stimulation [56]. The axonal load found in our cadaver study is comparable to other studies found in literature reporting 5300 to 7000 axons [57–61].
Of 6683 axons/cross section found in our specimens, it is not certain what percentage of these are exclusively branchial motor axons to mimetic muscles and what number of them have different fiber qualities. In its entire intra and extracranial course the facial nerve consists of different functional nerve fibers such as motor, vegetative, sensory and sensitive fibers [62]. The specimens taken as facial nerve main branches in this study were taken shortly after its exit point at the stylomastoid foramen. At this point, the facial nerve contains a somatosensory portion innervating the ear and special visceral efferent innervation to the digastricus muscle, the stylohyoid muscle and lastly the muscles of facial expression [62, 63]. Hence, nerve fibers and fascicles counted in this study mainly belonged to the mimic portion of the facial nerve. Nevertheless, an organization into fascicles is apparent and already described in several studies [58, 64]. As described by Captier the fascicular distribution and spatial organization of the fascicles was extremely heterogeneous [58]. In their study the number of fascicles and their organization changed in each segment every 2 mm. These findings illustrate the complexity of microsurgical repair in trauma or tumor cases. Their group even found differences between facial sides in the same subject demonstrating variations of fascicle number and diameter [58]. Interestingly we found a significant difference in axon load between right and left facial halves in our study.
As described by the group of Hembd et al. with increasing age axonal load of the facial nerve diminishes [57]. They defined three different age groups showing axon counts for the facial nerve trunk of 5748 axons (22–59 years), 5352 (61–79 years) and 5001 (80–97 years). Their group also did not find a difference in axonal load for facial sides or gender [57].
We found a facial nerve diameter at its extratemporal trunk measuring close to 2 mm. Histological processing and staining includes a shrinkage rate of around 20%. so that in a clinical situation the nerve diameter may be expected to be around 2.3 mm on average. Very few publications in literature may be found about clinical diameters of facial nerve branches. In an ultrasound examination series of 104 healthy individuals by Li et al. roughly comparable diameters were described, stating a mean diameter of 1.6±0.3 mm at the extratemporal facial nerve trunk [65]. A study of 23 formaldehyde-fixed cadavers by Salame et al. reported 2.66±0.55 mm (range, 1.10 to 3.39) [66].
Disclosure and funding sources
There were no sources of support in the form of grants, equipment, drugs or of other nature. No conflicts of interest.
Footnotes
Acknowledgments
This study is dedicated to Prof. Dr. Friedrich Jung, who recently celebrated his 70th birthday, honoring his life accomplishments for research and basis science.
We acknowledge those who donated their bodies to science. The authors thank Mr. Florian Zeman of the Center of Clinical Studies, University of Regensburg, for his contribution to the statistics of this study.