
Abstract
Orthokeratology (Ortho-K) is an over-night hard contact lens therapy, which physically reshapes the corneal curvature in order to stabilize or temporally eliminate myopia in patients. We hypothesize that the prolonged physical contact and mechanical pressure induced by the Ortho-K lenses may create lasting inadvertent effects and damages (microangiopathy), and may bring about unwanted changes in the microvasculature of the bulbar conjunctiva. Computer-assisted intravital microscopy (CAIM) was used to view, document (via videotaping) and objectively quantify (via computer-assisted image analysis) the real-time dynamic and morphometric characteristics of the conjunctival microcirculation in long-term (at least over one year) Ortho-K patients (n = 11) and matched non-user control subjects (n = 8). Ortho-K patients were instructed to wear their lenses overnight following standard protocol. During the study, the conjunctival microcirculation of the left eye of all Ortho-K lens users was viewed, frequently re-focused and videotaped, without and with the lens in place, as outlined in Methods. The matched control subjects (non-lens wearing) were videotaped and studied in like manner. The dynamic and morphometric characteristics of each user and control subject were analyzed, quantified and summated as a severity index (SI) collectively for comparison. SI of Ortho-K lens users (4.18±1.08) differed significantly from SI of control subjects (1.75±1.39, p≤0.05). In addition, changes in the conjunctival microcirculation (e.g., flow velocity, vessel diameter, shape change, etc) were viewed and videotaped immediately after the myopic patients put on the Ortho-K lenses. Eight of the 11 Ortho-K lens users displayed significant percentage changes (p≤0.05) in flow velocity and 10 of 11 displayed significant percentage changes (p≤0.05) in vessel diameter, without and with the Ortho-K lenses. The results clearly indicated that significant microvascular changes via tissue remodeling occurred, and were caused directly by the physical presence of the Ortho-K lenses.
Keywords
Introduction
The prevalence of myopia, or near-sightedness, is a growing problem in the global pediatric population, with an abundance of cases reported as early as seven years of age [1]. This trend can be easily observed in locations such as Hong Kong, China where 36.71% of the children are reported to have the condition [2]. In the United States, there had been a 49.8% increase in myopia in the general population over the course of the last 30 years. Although myopia can be managed by a refractive correction protocol (e.g., prescription-corrective spectacles, contact lenses or refractive surgery, including photorefractive keratectomy, LASIK, etc), it cannot successfully treat or manage degenerative myopia, an aggressive deterioration in visual acuity caused by rapid myopic progression. If left untreated, degenerative myopia may lead to permanent vision loss, choroidal neovascularization, glaucoma, cataracts, and retinal detachment [3]. In such cases, Orthokeratology (Ortho-K) is often recommended as an alternative and aggressive treatment modality to prevent degenerative myopia by halting its rapid progression and to achieve visual acuity.
Close follow-up is also imperative on the ocular health of Ortho-K patients. Common ocular health concerns associated with Ortho-K exists, including infectious keratitis, with high incidences of pseudomonas and acanthamoeba infections. In recent years, Ortho-K was reported to account for 19.1 to 38.8% of infectious keratitis cases [3]. Treatment of ocular infections involves using prescribed antimicrobial drugs, which will not prevent future infections and may produce unwanted side effects. Further investigations in ocular health related to Ortho-K have shown significant adverse changes in the eye, including development of astigmatism, increase in corneal epithelial defects and decrease in endothelial cell density leading to corneal edema [4]. Although the effectiveness of Ortho-K to treat and manage aggressive myopia has been demonstrated, the adverse ocular risks and complications associated with its use cannot be ignored and under-estimated. The Ortho-K lens sits on top of the corneal surface and creates repeated mechanical interactions with the bulbar conjunctiva. Real-time investigations on the pathologic changes arising from this rigid lens/underlying blood vessel interaction and the resulting microangiopathy have not been investigated or quantified in an in vivo real-time setting to assess the immediate as well as long-term impact of Ortho-K on the microvasculature of the bulbar conjunctiva.
In a previous study on contact lens users in this laboratory, soft gas-permeable contact lenses had been shown to physically occlude blood flow in the conjunctival vessels and effectively changed the blood flow velocity, vessel diameter and vessel distribution [5]. The changes in the dynamic and morphometric characteristics of the vessels were hypothesized to be caused by the sustained pressure and physical contact of the edge of the contact lenses against the surface of the bulbar conjunctiva [5]. The physical changes in the underlying vessels and the impediment of blood flow in an occluded vessel could easily be seen in videotape sequences and were visually self-explanatory in the development of vessel tortuosity. As for the other changes (e.g., vessel tortuosity) – according to the late Professor Benjamin Zweifach (a world-renowned microcirculation expert) – one might consider this lens/vessel interaction as a condition which differed from the normal state of the microcirculation, and would result in vascular remodeling to maintain local homeostasis [6, 7]. If the interaction was from a transient occurrence or insult, the changes would be temporary and would subsequently disappear when the interaction was removed. However, when the interaction was sustained, significant remodeling would take place and the changes would persist and became permanent, even when the interaction was later removed, indicative of tissue (in this case, vascular) remodeling and adaptation due to sustained mechanical pressure and vascular occlusion. For example, sustained blockage of a conjunctival vein/venule would physically cause irreversible vessel tortuosity. Accordingly, we hypothesize that Ortho-K lenses could cause significant microangiopathy in the microvasculature of the bulbar conjunctiva in Ortho-K lens users – due to the physical interaction of the lenses and the underlying conjunctival microcirculation – and that significant tissue remodeling would take place in long-term Ortho-K patients.
Materials (Subject recruitment and Design)
Subject recruitment
A total of 11 long-term Ortho-K patients/lens users and eight matching historical non-contact lens users as control subjects were recruited from the Dr. Brian D. Tracy Eye Clinic (a private optometry practice) and the Department of Ophthalmology, UC Davis School of Medicine in Sacramento, CA. The inclusion criteria for the recruitment required Ortho-K subjects to have used Ortho-K lenses continuously for at least one year. Any subject with a medical history of vascular disease (e.g., hypertension, diabetes mellitus, or sickle cell anemia, etc) was excluded from the study. Similarly, any control subject with a medical history of vascular disease, a contact lens user, or had undergone refractive surgery, was excluded. The recruitment and the study protocol had been approved by the UC Davis Human Subject Use Committee and the Eye Clinic review protocol. Signed consent was obtained from each subject. This study was conducted in accordance with the Declaration of Helsinki Human Use guidelines. Patient confidentiality was maintained throughout the study and in this report.
Design
Eleven Ortho-K lens users and eight control subjects were studied. The conjunctival microcirculation of each Ortho-K subject or control subject was viewed and videotaped according to the CAIM protocol, as described in detail in previous publications [5, 8–11] and outlined briefly in Methods. Videotaping was focused on the peri-limbal region of the bulbar conjunctiva of the left eye in all subjects. Special emphasis was placed on the conjunctival vessels in different locations within the peri-limbal region, where the vessels were in contact with, or adjacent to, the edge of the Ortho-K lenses.
Due to the unique protocol of Ortho-K, the lenses were used as an overnight treatment and management modality. Therefore, each Ortho-K subject was asked to wear the Ortho-K lenses overnight and to remove the lenses in the morning accordingly [12], and to bring the lenses with them to the clinic. The left eye of all Ortho-K lens users was viewed and videotaped, with re-focusing as needed to ensure image clarity and sharp image display, based on the following specific time-frames: Upon arrival at the clinic without wearing the Ortho-K lenses – each patient was videotaped for 15 minutes, focusing on the arterioles and venules in the peri-limbal region of the bulbar conjunctiva. This step would generate a view of most of the vessels interacting with, or adjacent to, the edge of the Ortho-K lens. Immediately after inserting the Ortho-K lens – each patient was videotaped for at least 30 minutes, relocating the previously videotaped vessels in Step (1) and focusing on points of interaction (at least five interaction sites) between the edge of the lens and the same underlying microvasculature in the peri-limbal region videotaped in Step (1). Relocated and videotaped the interaction sites repeatedly for 30 minutes, with special emphasis on the dynamic* and morphometric# changes adjacent to the interaction sites between the lens and the underlying microvasculature. Selected videotape sequences were analyzed for dynamic* (e.g., blood flow velocity, intermittent flow, trickle flow) and morphometric# (e.g., shape, diameter, tortuosity, hematoma adjacent to damaged vessels, hemosiderin deposits/spots, etc) characteristics. The results generated were interpreted individually, averaged, analyzed, and summated as an SI for comparison with the control subject(s)
Each control subject was studied and continuously videotaped for at least 30 minutes [see Design]. Selected videotape sequences were used to generate individual SI for the control subjects. The SI and results from all control subjects were studied in like-manner as Ortho-K lens users, and all results were used individually, averaged for comparison, and analyzed for statistical significance. Interesting features and visible microangiopathy from the videotape sequences were frame-captured as individual image frames for analysis, comparison and displayed, as shown in Fig. 1 and 3.
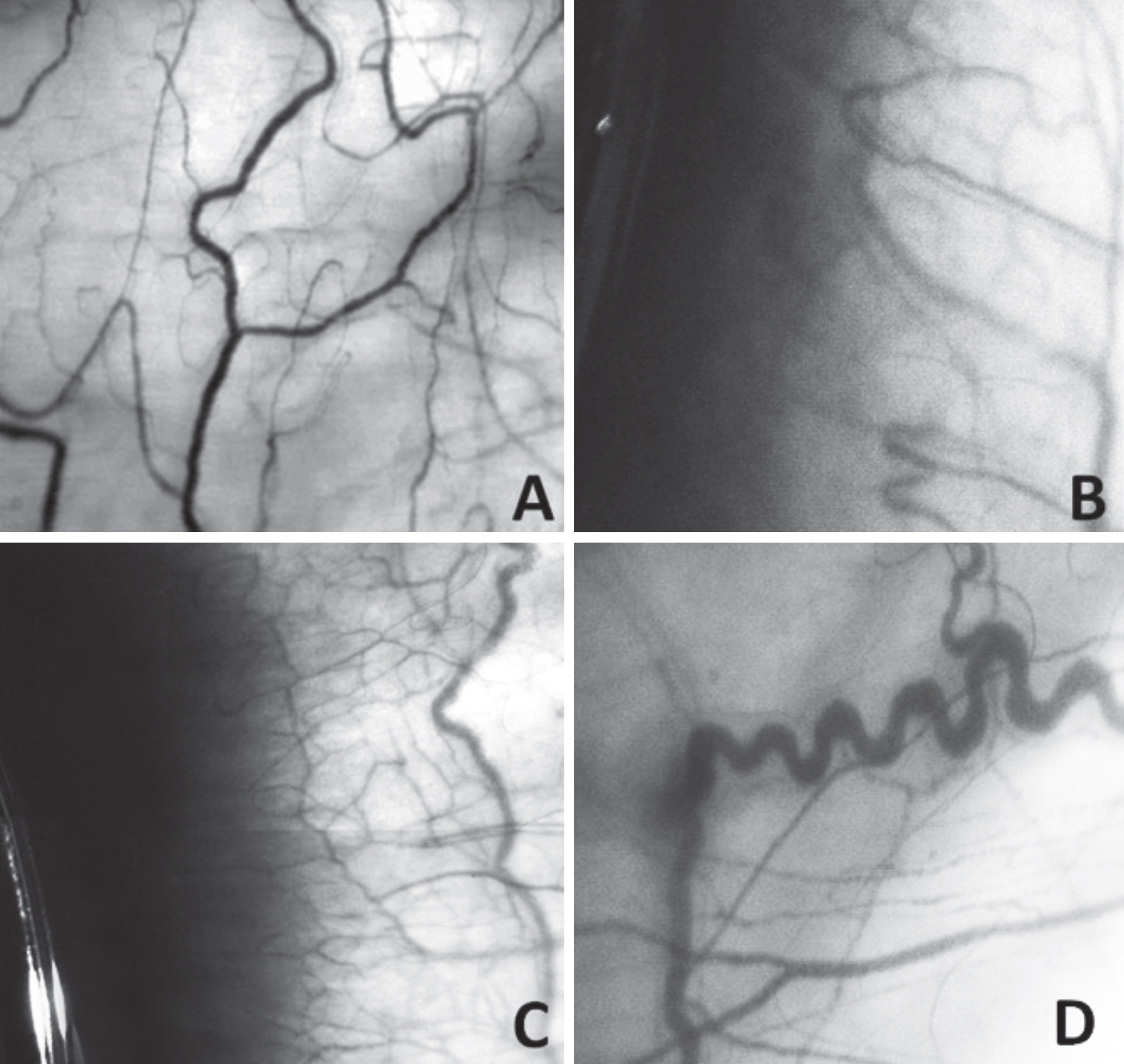
Frame-captured images of the conjunctival microcirculation acquired via computer-assisted intravital microscopy. (4.5x optical magnification; 125x on-screen magnification; full frame area = 8.53 mm2). These images were selected from videotape sequences of the conjunctival microcirculation in (A) a control subject and (B), (C) and (D), three different long-term Ortho-K patients. (A) A historical image from this laboratory of the conjunctival microcirculation of a control subject. Note the even distribution of normal-sized arterioles and venules, and the absence of microangiopathy. This could be considered as an image of a close-to-idealized microcirculation, and could serve as an excellent reference for comparison. (B) and (C) were images of the microcirculation of two Ortho-K lens users, with the lenses still in place, as the light-reflecting edge of the lenses could be located on the left side of each frame. Significant microangiopathy (vessel distribution, diameter, density, neovascularization, etc) could be recognized when compared with (A). In addition, significant damages occurred close to the edge of the lenses and a large hematoma resulted, covering the entire left side of the frame in both images. Hemosiderin deposits could be seen as gray-colored dots diffusely located along the edge of the hematoma. (D) An image of the conjunctival microvasculature showing extremely abnormal vessel presentation and distribution. At the point where the vessel was damaged (and healed) or blocked, one could see the permanent result of an occluded vessel where its down-stream flow had been impeded, resulting in a significantly tortuous vessel configuration upstream. This tortuous vessel configuration persisted, even though the Ortho-K lens was not inserted in this case. Hemosiderin deposit could be seen arising from the damaged site and spanning across the entire vessel. Note that the area farthest away at the lower right corner of the image did not show any hemosiderin deposit and presented an ischemic outlook.
Computer-assisted intravital microscopy (CAIM) was used as a research platform, as described in detail in previous reports [5, 8–11] and briefly described below. CAIM has been adapted to observe and document (via videotaping) the real-time conjunctival microcirculation of the Ortho-K patients (without and with Ortho-K lenses) and control subjects as outlined in Design. All videotape sequences were viewed in their entirety and well-resolved sequences were selected and objectively quantified via computer-assisted image analysis for their dynamic and morphometric characteristics. Using CAIM, data acquisition was obtained through quantitative and objective assessments of the videotape sequences on any microangiopathy present in each patient or control subject, and the results were reported as an SI, which represented a summary computation of microangiopathy and an indication of induced vasculopathy for each subject. This technology and protocol had been previously verified and applied to study polymer-hydrogel soft contact lenses and biomarkers for the detection of vascular diseases, such as diabetes, sickle cell anemia and hypertension [5, 8–10]. Most conjunctival vessels normally appeared in different shapes and forms (e.g., tortuous, wide diameter, loops, turns, damaged, box-car, etc), and could be identified for longitudinal (follow-up) evaluations, with each vessel itself serving as its own reference control. With the application of this non-invasive and longitudinal technology, quantifiable real-time changes to the microvasculature of the bulbar conjunctiva could be investigated to better understand Ortho-K.
Videotaping procedure
The videotaping time-frame outlined in Design was adopted. For every videotaping session, each Ortho-K or control subject was asked to relax for at least five minutes and cautioned against touching or rubbing the left eye. Non-medicated, sterile saline drops were administered in case of eye irritation and excessive drops were blotted. Each subject was asked to place his/her forehead securely against a forehead-chin restraint. The front-lens element of the CAIM system was carefully positioned to provide a focused, clear and well-resolved view of the conjunctival microcirculation of the left eye to give an 8.53 mm2 area view of the microvascular location of interest. Various locations of interest were videotaped (e.g., abnormally-shaped vessels, interacting sites where the edge of the lens made contact with underlying vessels, damaged vessels, hematoma, tortuous vessels, wide vessel diameter, etc) in each subject, using a charge-coupled device (CCD) video-camera (COHO Model CCD-6415-3000) connected online with a digital video-recorder (SONY GV-HD700). A fiber-optics light source (Fiber-Lite Model 3100) coupled with a Kodak #58 Wratten anti-red filter was used to enhance contrast of the vessels against background for sharp image display. The basic design of CAIM was based on macro-optics as an operational platform so that focusing for image sharpness and field clarity could only be obtained by adjusting the physical distance between the front-lens element and the bulbar conjunctiva. As such, this allowed video images to be clearly obtained at the same magnification for all videotapes for comparison. Approximately 15–45 minutes of high-resolution videotape-recordings at various locations in the bulbar conjunctiva of each patient or control subject (see time-frames outlined in Design) were made for subsequent viewing, measurement and image analysis.
Data analysis
All videotape recordings were viewed in their entirety and sequences of interest were selected for subsequent visual and computer-assisted image analysis and measurements. At least three videotape sequences with excellent image display (see Fig. 1 and 3) from each subject and each relevant time-frame were analyzed and all measurements were averaged. Specific microangiopathy (e.g., abnormal vessel diameters, intermittent blood flow, stagnation of blood flow due to lens occlusion, microaneurysms, damaged vessels, hematoma, vessel tortuosity, etc) was identified from the videotape sequences and used to compute an SI. The same videotape sequences were also analyzed using image analysis software (AVID; co-developed at UC Davis and Scripps Institute) to objectively compare all results for statistical significance.
Statistics
Analysis of variance (ANOVA) was used to compare differences between groups. A p-value of≤0.05 was considered statistically significant.
Results
Macro-optics, infinity-corrected lenses and a CCD video-camera were used as the basic image-acquisition platform of the CAIM system. Because of the unique microscopic design, well-resolved, sharply-focused and crisp videotape sequences with the same magnification were made on the real-time microvasculature in the bulbar conjunctiva of the human eye for subsequent analysis, as shown in Fig. 1A, 1B, 1C and 1D. Significant pathologic changes (microangiopathy) in the conjunctival microcirculation in Ortho-K lens users, as compared with control subjects (non-Ortho-K and non-contact lens users), could easily be seen in frame-captured images from selected videotape sequences. Figure 1A showcased a very well organized network of arterioles and venules in the peri-limbal region of a control subject. The vessel morphometry was normal and adverse features (e.g., wide vessel diameter, damaged vessel, vessel tortuosity, flow-stagnation, trickled flow, etc) were not seen throughout. Flow velocity in the microcirculation was normal and comparable to historic values obtained in our laboratory [5, 8–11]. In fact, a very well-organized and uniformly distributed microvascular network was displayed throughout this image frame. The vessels travelled in a smooth course and vessel tortuosity was absent. This frame presented an image of the conjunctival microcirculation with a near-idealized microvascular presentation and could be considered an excellent control image for reference. In this frame-captured image, the SI was computed as 0, as no microvascular abnormality existed. Comparing Fig. 1B, 1C and 1D with Fig. 1A, one could immediately see significant departures from the near perfect microvasculature. Various microvascular abnormalities were observed in Ortho-K lens users, including vessel distribution, vessel diameter, vessel tortuosity, damaged vessel, hematoma, hemosiderin deposits, stagnation of blood flow, and very slow to trickled flow in some cases. In addition, the distribution of arterioles and venules in Fig. 1D (as compared to Fig. 1A), demonstrated an ischemic environment with uneven vessel distribution.
In Fig. 1B, 1C and 1D, hematoma and hemosiderin spots from damaged vessels could be identified in different locations, as compared with a clear non-contaminated background in Fig. 1A. At the left edge of Fig. 1B and 1C, one could see the light-reflecting edge of the Ortho-K lenses. There were subsequent vessel damages around areas where the edge of the lenses was in contact with the underlying conjunctival vessels. A large dark-colored patch of hematoma resulted in each case, covering the entire left edge of the image. On the edge of the hematoma away from the lens, one could identify an abundance of hemosiderin spots, appearing as grayish color dots close to the hematoma. Figure 1D showed an area of the peri-limbal region of an Ortho-K patient with the lens removed. It clearly showed a tortuous vessel changing its course and shape as it approached the region where the edge of the Ortho-K lens made contact and occluded the flow. The lens contact point left a previously damaged but now healed location (note the small dark patch where the relatively tortuous vessel straightened out its meandering course) – no hematoma was present as it was probably very small and/or was resolved. However, an abundance of hemosiderin deposit (as little dots) could be seen, spreading from the damaged location of the vessel, and spanning the entire course of the vessel. It was significant to note that the tortuous shape of the vessel persisted (via tissue remodeling), despite the fact that the Ortho-K lens was not present.
A summation of the presence of all microangiopathy in the conjunctival microcirculation in each Ortho-K lens user and control subject was used to create a quantitative SI for Ortho-K lens user and control subject comparison. SI of the Ortho-K lens users (4.18±1.08) differed significantly from the SI of control subjects (1.75±1.39; p≤0.05) as shown in Fig. 2, indicative of the significant differences in the microvasculature of Ortho-K lens users and control subjects.
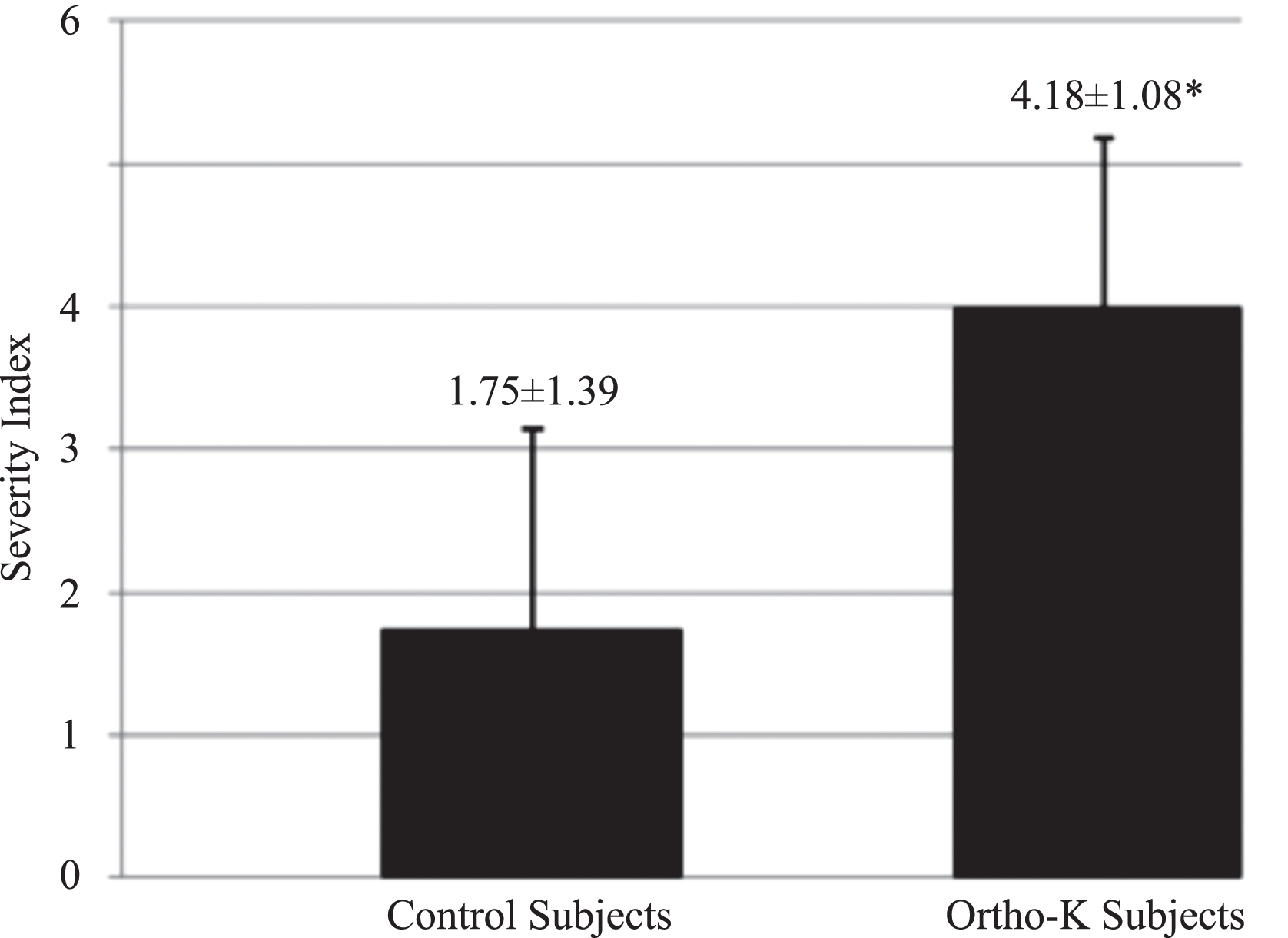
Quantitative comparison of microangiopathy (computed as SI) between control and Ortho-K subjects. Note the significantly elevated SI in Ortho-K subjects compared with the low SI of control subjects.
A circulatory system (in this case the microcirculation) consisted of vessels with deformable walls, which could adapt and change to different configurations when their down-stream flows were blocked. The blocked vessel could change from a relatively straight path to one of significant tortuosity when its down-stream flow was physically blocked and the blockage was sustained. In Fig. 1D, such a situation occurred. Over time, tissue remodeling occurred and the tortuous configuration of this vessel persisted, even when the constraint (the edge of the lens interacting with the vessel) was removed and the hematoma was resolved. Therefore, tortuous vessels were always found in long-term Ortho-K lens users as well as in all contact-lens users, even when the videotapes were made without the lenses in place at the time of videotaping. Not just in the case of vessel tortuosity, basically all other microangiopathy induced by long-term use of the lens(es) persisted even without the lens in place. While long-term changes occurred and persisted due to tissue remodeling, it was interesting to note that immediate changes in vessel dynamics (e.g., blood flow velocity) and morphometry (e.g., vessel size/diameter) would occur when an Ortho-K lens was inserted. However, these transient changes would disappear if the lens was removed shortly. This case scenario represented a simple stop and go phenomenon and did not arise because of tissue remodeling.
The recent prevalence of progressive myopia and the increased use of Ortho-K as a treatment protocol necessitate further studies on Ortho-K and possible adverse and unexpected side-effects on the microvasculature of the bulbar conjunctiva in the eyes of long-term Ortho-K lens users. According to the literature in tissue remodeling, induced microvascular changes in lens users are reversible if the lens use is short-term and transient. However, according to the standard protocol, Ortho-K lens use is long-term and sustained. Therefore, any microvascular abnormalities induced by the Ortho-K lens will be permanent and will create definite adverse effects on ocular health and safety. Known adverse effects include, but not limited to, corneal staining, abrasion, and microbial keratitis. These adverse effects are important and cannot be ignored or underestimated, but have not been adequately investigated. Results from this study have laid down the foundation which can lead to further in-depth investigations. In addition, the effectiveness of CAIM to be used as a real-time and quantitative tool offers a non-invasive method to conduct such studies.
It was obvious that the sustained, physical contact of the edge of the Ortho-K lenses and the underlying vessels caused the pathological damages observed and documented in this study. Whether the damages arose from improper fitting, properties of the lens material(s), reverse geometry lens design, or the physical nature of the edge of the lenses, these parameters have not been studied and are not fully understood. Results from this study can be used as a basis to develop these associations. We hypothesize that the material(s) used to make the lenses, the mechanical invasiveness of the edge of the lenses and its geometry may have inadvertent effects on the outcome of ocular health, and should be fully understood. In addition, the mechanical forces and physical interactions between the lenses and the underlying microvasculature could not be ignored, and proper fitting of the lens would be crucial to prevent microvascular damages and maintain ocular health.
With all the damaging results generated in this study as shown in Fig. 1 (B, C and D), questions may be raised on why Ortho-K lenses are still utilized and why are there not more ocular health complications associated with Ortho-K treatment. A hypothesis, based on biomechanical interpretation, can be made referring to a basic principle in physics interacting with mother nature. Because of the physiology of the eye, a natural layer of tear is constantly maintained on the surface of the bulbar conjunctiva – it is a wetting layer of physiological fluid, which serves a lubricating-and-protective purpose. When a wetted Ortho-K lens is inserted, a water lens via surface tension will be formed, connecting the inside surface of the lens, the edge of the lens and the surface of the bulbar conjunctiva. The weight of the Ortho-K lens and physical forces will exert pressure downward to distribute the fluid and create a dynamic fluid exchange between the tear on the surface of the bulbar conjunctiva and inside surface of the lens. With a proper Ortho-K lens fitting, the presence of a dynamic water-lens with adequate fluid exchange can be maintained to cushion the edges of the lens and to prevent excessive physical pressure on the microvasculature of the bulbar conjunctiva. This hypothesis was verified as shown in Fig. 3. Figure 3A showed a segment of a conjunctival vessel without the Ortho-K lens put in place. This vessel had a normal vessel diameter (63.45μm) compared to the same vessel with a significantly lesser diameter (46.58μm) indicative of flow impediment 20 minutes after the lens was inserted (Fig. 3B). The change in vessel diameter (without and with the Ortho-K lens) was significant (63.45μm to 46.58μm; p≤0.05). However, in Fig. 3C, the same vessel segment videotaped one minute after Fig. 3B was made –21 minutes after the lens was inserted – (with the lens still in place and the camera focused on the same location), the vessel had regained its normal steady flow and reverted significantly close to its original diameter (70.2μm; p≤0.05). With reference to Fig. 3B, Fig. 3C showed the result of a successful adaptation (not remodeling) process based on the design of the Ortho-K lens. Because of proper Ortho-K lens fitting by the optometrist, the water lens was formed and fluid-exchange equilibrium was maintained as expected, successfully cushioning the mechanical force exerted by the edge of the lens and preventing the formation of contact hot-spots. With adequate cushioning, the physical impact of the lens was negated and normal blood flow resumed after a period of adjustment to maintain dynamic fluid-exchange equilibrium (in this case, ∼20 + minutes). Figure 3C differed significantly from Fig. 1D. The inadvertent effect of the Ortho-K lens and normal blood flow and normal vessel diameter returned after a short adjustment period because of good lens fitting in Fig. 3C. The microangiopathy in Fig. 1D persisted even without the lens in place, probably due to poor lens fitting, resulting in sustained physical insults to the vessel itself and the microangiopathy became permanent because of tissue remodeling.

Comparison of diameter changes in the same conjunctival vessel at three different time frames. (4.5x optical magnification; 125x on-screen magnification; full frame area = 8.53mm2). (A) Ortho-K lens was absent. (B) Ortho-K lens was present = 20 minutes after insertion. (C) Ortho-K lens was present = 21 minutes after insertion. In all cases as shown in (A), (B) and (C), the significant tortuosity of the vein/venule, which was caused by a sustained long-term physical blockage of the vessel by the edge of the lens, persisted with or without the lens in place.
Hypoxia may contribute to the vascular remodeling observed in Ortho-K. While Dk/t values of 87 to 125 have been recognized as acceptable oxygen transmissibility levels, Ortho-K lenses have been measured to have highly variable oxygen transmission properties, with lenses citing Dk/t values of 47, 67 and 91 in lenses studied [13–15]. Hypoxia is an important factor involved in angiogenesis and vascular remodeling, but the relationship of hypoxia (and different lens materials per se) to microangiopathy and ocular health is poorly understood. Thus the development of gas-permeable Ortho-K lenses with better oxygen transmissibility is warranted.
The argument exists that myopia can be managed simply by using prescription spectacles or soft contact lenses. It is obvious and true that spectacles and soft contact lenses can definitely improve visual acuity. However, they cannot slow down the rapid progression of myopia in most patients. Refractive surgery can also be used to improve visual acuity by correcting refractive errors. In most cases, this procedure appeals to myopic patients due to improved physical look and independence from wearing spectacles or contact lenses. However, refractive surgery has no therapeutic value to manage degenerative and rapid myopia progression, and is only employed when there is stabilization to myopia. In addition, refractive surgery carries certain risks and complications inherent in any surgical procedure. Recently, Ortho-K has become an important alternative modality to address rapid myopia progression as well as treating myopia itself. It is important to study all the possible effects of Ortho-K on bulbar conjunctiva integrity and long-term ocular health outcome to better understand this treatment modality and to use it safely to treat degenerative myopia without complications.
Footnotes
Acknowledgments
We would like to acknowledge the valuable assistance of the nurses and staff of the Dr. Brian D. Tracy Eye Clinic and the Department of Ophthalmology at UC Davis Medical Center. Their co-ordination and cooperation were very much appreciated. The roles played by the Ortho-K patients, the control subjects and their families were immeasurable and the study could not be successful or completed without their participation. We would like to express our gratitude for the financial support from the Department of Pathology and Laboratory Medicine Hugh Edmondson Fellowship, which was generously awarded to this unit for conducting the research study in our research-mentorship program.