
Abstract
BACKGROUND:
Contrast-enhanced ultrasound (CEUS) has been used as an additional imaging technique in order to evaluate focal liver lesions. CEUS is easy and fast to perform, overcomes the limitations of B-mode US.
OBJECTIVE:
To evaluate the diagnostic potential of contrast-enhanced ultrasound (CEUS) in focal liver lesions (FLL) with unclear findings on computed tomography (CT) or magnetic resonance imaging (MRI).
METHODS:
In this single-center retrospective study, 146 patients with at least one FLL underwent additional CEUS of the liver to clarify inconclusive cross-sectional imaging findings. Ultrasonography was performed using B-mode imaging and CEUS after injection of sulphur hexafluoride microbubbles (second-generation contrast agent) within two months after ceMRI or ceCT and interpreted by an experienced radiologist (EFSUMB level 3). Histopathological reports, long-term follow-up or clinical course served as reference standard.
RESULTS:
Thirty-eight of the 146 patients had malignant and 108 benign FLL. Overall, CEUS had 92% sensitivity (95% -CI, 79–97) and 98% specificity (95% -CI, 93–99) with an AUC of 0.95 in correctly characterizing the lesion as malignant or benign. Sensitivity increased to 98% (95% -CI, 96–100) for benign lesions and decreased to 92% (95% -CI, 78–98) for malignant lesions. CEUS showed the highest diagnostical accuracy in lesion <1 cm with an AUC of 1.000, while the lowest accuracy was achieved in lesions >2 cm with an AUC of 0.924 due to a decreasing specificity of 86% (95% -CI, 87–100).
CONCLUSION:
CEUS correctly distinguished malignant from benign FLL in cases with inconclusive cross-sectional imaging findings and achieved high levels of diagnostic accuracy. CEUS has added diagnostic value especially in small lesions ≤1 cm while specificity remains limited in larger lesions.
Introduction
Ultrasound is widely used as the primary imaging method in the diagnostic workup of abdominal conditions in general, although contrast-enhanced computed tomography (ceCT) and magnetic resonance imaging (ceMRI) represent the gold standard in diagnostic algorithms for the assessment of focal liver lesions (FLL) [1]. Further, ceCT is also the standard imaging tool to evaluate local tumor extent and thoracoabdominal metastasis. Under the primacy of “the correct diagnosis as early as possible” the number of curative surgical resections and ablation procedures has increased during the past decades [2]. Therefore, accurate determination of the tumor extent in the liver is an important prerequisite for choosing the best therapeutic approach (surgical resection vs. local interventional treatment such as brachytherapy or radiofrequency ablation).
Over the last 15 years, increasing evidence has emerged that contrast-enhanced ultrasonography (CEUS) may contribute to the characterization of FLL [3, 4]. The diagnostic power of CEUS has improved with the advent of the non-destructive low-acoustic-power ultrasound mode and new generations of ultrasound contrast agents based on sulphur hexafluoride microbubbles [5]. Due highly accurate visualization of microbubble contrast agents as they distribute in blood over a defined time period, benign liver lesions like hemangiomas and focal nodular hyperplasia (FNH) can be diagnosed with almost 100% certainty, and CEUS has been shown to be superior to ceCT or ceMRI in certain cases [5–7].
Most FLL are detected incidentally during routine abdominal imaging examinations for other conditions (e.g., ultrasound), in staging or follow-up examinations in oncologic patients, or in the setting of surveillance programs for chronic liver disease (e.g., cirrhosis) [1, 8]. While liver lesions are a common incidental finding in cancer patients, ceCT and ceMRI are limited in the visualization of contrast enhancement patterns especially in small lesions to distinguish between benign liver lesions and metastasis [8]. The diagnostic ability of B-mode and Doppler ultrasound is also limited, while CEUS was shown to potentially improve detection rates as well as lesion characterization significantly [9–15]. Despite the influence of difficult examination conditions, CEUS has been shown as an excellent diagnostic procedure for the assessment of liver lesions in the hands of an experienced investigator [16].
Therefore, CEUS was included into the hepatocellular carcinoma (HCC) guidelines of the American Association for the Study of Liver Diseases (AASLD) in 2005; however, it was removed again in 2011 as a reaction to results published by the Barcelona Clinic Liver Cancer (BCLC) group in 2010 following reports indicating a high potential for misdiagnosis [17–19]. Consequently, the European Association for the study of Liver (EASL) guidelines excluded CEUS in 2012 [20]. Although CEUS re-appeared in the EASL guidelines in 2018, evidence is still moderate and recommendations are weak [8]. The European Federation of Societies for Ultrasound in Medicine and Biology [EFSUMB) first recommended CEUS in 2004, confirming this recommendation in their updated guidelines of 2008 and 2012 for use in characterizing FLL in the following situations: incidental findings in patients with a history for malignancy and contraindications to and/or unclear findings in CT and MRI [3, 22]. Dynamic 3D-CEUS can further be used for evaluation of the perfusion of FLL avoiding adverse factors of sampling, while stable and reliable 3D CEUS parameters showed a good correlation with those of 2D-CEUS [23].
The purpose of this study was to investigate the potential added diagnostic performance of CEUS in characterization of FLL in either malignant or benign in patients without a clear diagnosis in ceCT or ceMRI.
Material and methods
Study cohort
Our institutional review board approved this single center retrospective analysis (registration number EA4/148/18). Oral and written informed consent was obtained from all patients before the ultrasound examination. All study data were collected in compliance with the principles expressed in the 2002 Declaration of Helsinki. The study population consisted of 146 patients who underwent CEUS of the liver after inconclusive cross-sectional imaging findings (ceCT, ceMRI) between 2012 and 2018 (inclusion criteria). Patients under the age of 18 were excluded. All cross-sectional imaging scans were interpreted by board certified radiologists with at least six years of experience in abdominal imaging. The ultrasound protocol included B-mode ultrasound, color-coded Doppler ultrasound (CCDS), and CEUS. Cancer was defined as patients with active malignancy or on anti-tumor therapy within the last six months before the examination or known metastatic disease. A study flowchart is provided in Fig. 2.
CEUS and examination protocol
For gray-scale B-mode imaging and lesion detection, the liver was examined using convex array transducer, assessing lesions in terms of size, echogenicity, and homogeneity. Color-coded and power Doppler ultrasound were employed to determine vascularization of detected masses. CEUS examinations were performed as routine clinical procedures using high-end ultrasound systems (Aplio500/Aplio i900; Canon Medical Systems Corporation, Tochigi, Japan; Acuson Sequoia, Siemens Healthineers, Mountain View, CA, USA) with state-of-the-art CEUS-specific protocols available. All convex transducers employed in study patients were required to be for abdominal use with a frequency range of 1–6 MHz. Of note, the multi-frequency ultra-wideband convex transducers (i8CX1, Canon Aplio i-series) used in this study cover the same bandwidth as two conventional transducers providing superior sensitivity and resolution for both near and far field in both B-mode US and CEUS. The ability shows the use of one transducer across a wider range of patient types, providing better imaging regardless of the patient conditions which may increase lesions detection and visualization of microbubbles. The low-mechanical-index (<0.1) technique was used to avoid early microbubble destruction. A bolus of 1.0–1.6 ml of ultrasound contrast agent (SonoVue®, Bracco Imaging, Milan, Italy) was repeatedly injected up to three times until high-quality cine loops were acquired. Following contrast agent injection, the liver was scanned for at least six minutes to capture reference lesions enhancement patterns and washout in the late contrast phase. Baseline B-mode US, CCDS including superb microvascular imaging (SMI), and CEUS were performed and interpreted by a single highly experienced radiologist with more than 15 years’ experience in CEUS imaging (EFSUMB level 3]. In case of multiple FLLs, the reference lesion of each CEUS examination were used in this study.
All lesions in CEUS were characterized according to the Guidelines and Good Clinical Practice Recommendations for CEUS in the Liver [4]. Sustained enhancement in the portal and late phases is typically observed in almost all solid benign liver lesions. They can be further characterized by their enhancement patterns during the arterial phase, (e.g., enhancement of the whole lesion [typical of focal nodular hyperplasia] or initial peripheral globular/nodular enhancement (in hemangiomas). For differentiation of malignant lesions, hypoenhancement in the late phases was observed corresponding to the wash out phenomenon characterizes malignancies. While almost all metastases show this feature, regardless of their enhancement pattern in the arterial phase, only few exceptions to this rule have been reported, mainly in atypical/well differentiated HCC.
Multisclice CT protocol
Overall, 71/146 patients underwent multiphase phase CT examinations (arterial, and/or portal-venous and/or venous / delayed phase) using a standard protocol with a 64 detector CT scanner (Somatom Sensation 64, Siemens Medical Systems, Forchheim, Germany) and a minimum slice thickness of 0.625 mm and reconstruction interval 2 mm. The contrast agent was injected into an antecubital vein as a bolus, using a dual head power injector with a flow rate of 4,5-5 ml/s. 100–120 ml (Ultravist®, Bayer Healthcare, Berlin, Germany) with an iodine concentration of 370 mg/ml was administered, followed by 50 ml saline. The acquisition direction was cranio-caudal.
MRI protocol
MRI was performed with 1.5 T and 3.0 T systems using phased-array body coils. The examination protocols comprised T2-weighted (w) standard 2D sequences with and without fat saturation (FS) and T1-w unenhanced 2D sequences with and without FS (including in-/opposed phase technique). T1-w 3D sequences with FS were acquired in breath hold technique before and during arterial, portal venous, and venous phase, respectively) after intravenous application of either gadoxetic acid (Gd-EOB-DTPA, Primovist or Eovist; Bayer Pharma, Berlin, Germany), Gd-BOPTA (Multihance, Bracco Imaging, Italy) or Gadubutrol (Gadovist, Bayer Pharma, Berlin Germany) (body weight adapted; manual or automatic injection at approximately 1-2 mL/s flow rate followed by 40 mL saline flush). In the hepatobiliary phase, T1-w imaging was repeated for gadoxetic acid 20 minutes and for Gd-BOPTA 60 minutes after contrast administration.
Reference standard
Histopathological reports were available in 20 patients, while the major portion of lesions were categorized as benign or too small for biopsy. In all other cases without histopathology, the reference standard was imaging long-term follow-up (>two years) for detection of lesion progress in combination with clinical surveillance including paraclinical parameters (laboratory tests, tumor markers etc.). All radiological reports were approved by board-certified radiologists.
Statistical analysis
Categorical variables were compared using the chi2 test, as appropriate. The CEUS findings and matched histopathological reports from each patient were retrospectively analyzed for diagnostic accuracy by testing sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) by means of a ROC-Curve analyses. A two-sided significance level of α= 0.05 was assumed to indicate statistical significance. Statistical analysis was performed with XLSTAT (Version 2011.0.01; Addinsoft SARL, New York, USA) and SPSS software (IBM; New York, USA).
Results
Patient demographics
A total of 146 patients were eligible for analysis (female: 61.2% (90/146); male: 38.8% (56/146). Mean age was 52.8y±16.5. Before the CEUS examination, patients underwent ceCT (71/146, 47.7%), ceMRI (39/146, 26.5%) in domo and 36/146 (25.2%) patients CT and/or MRI ex domo and overall 50/146 (34.0%) patients had more than one FLL. If patients with inconclusive findings on external performed cross sections imaging where referred by external radiologists for additional CEUS, patients received only B-mode US and CEUS in our institution Active malignancy was present in 44.9% (66/146) of the patients. The most common malignancies were breast cancer in 34.8% (23/66), colorectal cancer in 12.5% (8/66), and hepatocellular carcinoma (HCC) in 10.5% (7/66). Mean reference lesion diameter in US/CEUS was 3.0±2.3 cm. Subdivided by lesion size, 41.8% (61/146) had lesions smaller than 2 cm and 58.2% (85/146) lesions ≥2 cm. When dichotomized in lesions ≤1 cm vs. >1 cm 11% (16/146) were lesions ≤1 cm and 89% (130/146) >1 cm.
Detailed baseline characteristics are compiled in Table 1.
Baseline characteristics of the entire study population
Baseline characteristics of the entire study population
*Defined as active or anti-tumor therapy within the last 6 months or metastatic state. As some patients presented with more than one malignancy, there are more tumor entities than tumor patients. Abbreviations: CRC, colorectal carcinoma; HCC, hepatocellular carcinoma; MM, malignant melanoma; NEC, neuroendocrine carcinoma; FNH, focal nodular hyperplasia; HCA, hepatocellular adenoma.
Entire study population
25.9% (38/146) of all lesions were classified as malignant while 74.1% (108/146) were classified as benign. The malignant lesions were either metastasis, accounting for 81.5% (31/38), or HCC, accounting for 18.5% (7/38). The most common benign lesions were hemangiomas with 68% (74/108), followed by FNH with 17.5% (19/108) and complex cysts with 6.5% (7/108). Hepatocellular adenoma (HCA) and/or adenomatosis were present in 2.75% (3/108), while one benign lesion each (0.9%) was a single (0.9%) echinococcus cyst, an infarction (Zahn), and a dysplastic nodule (1/108) (Table 1). For all FLL in the entire study population, CEUS achieved 92% sensitivity (95% -CI, 79–97), a 98% specificity (95% -CI, 93–99), a positive predictive value of 95% (95% -CI, 82–99), and a negative predictive value of 97% (95% -CI, 92–99) in characterizing the lesions correctly as malignant or benign ROC analysis yielded an AUC of 0.959 (Tab. 2 / Figs. 1a and 2).
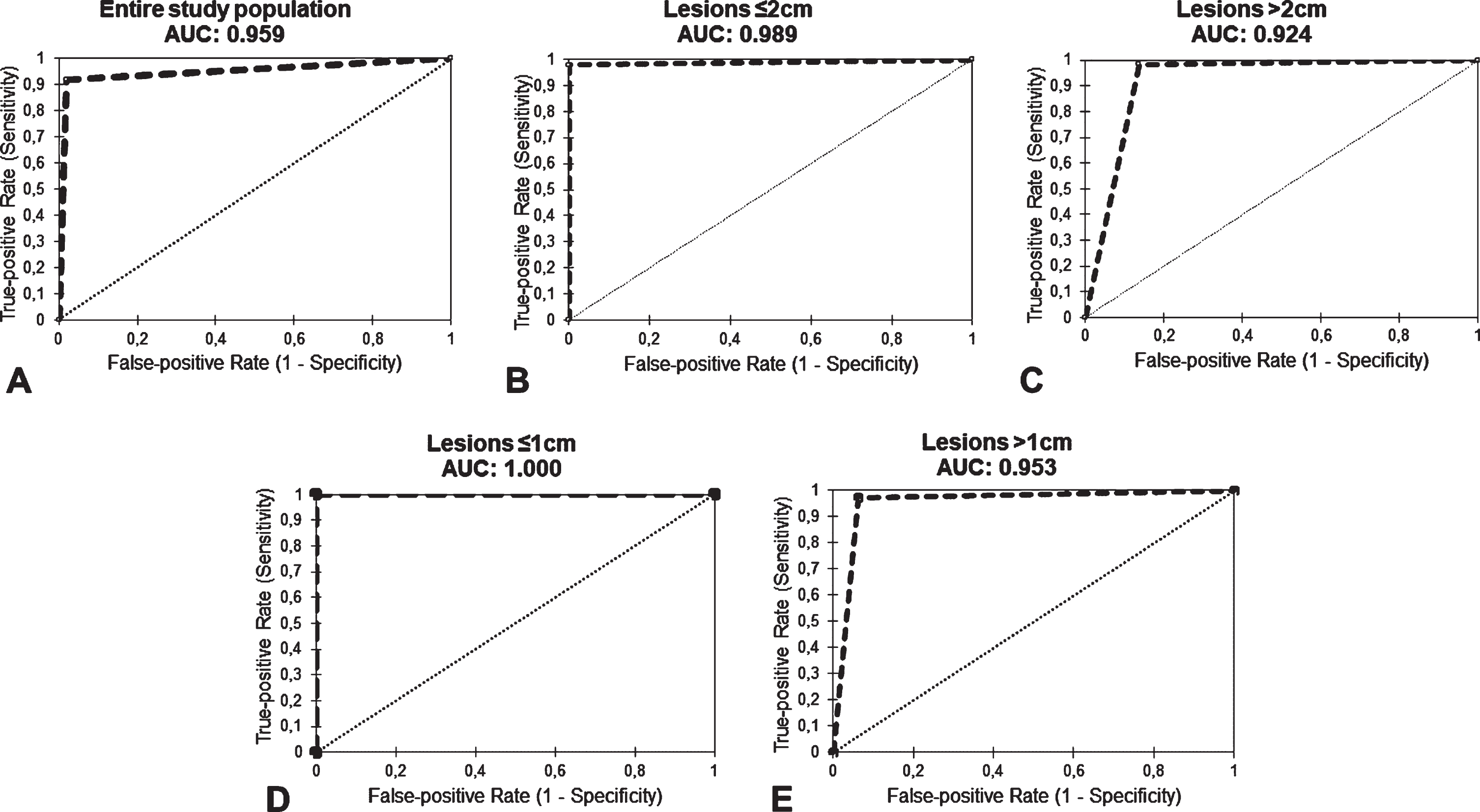
Diagnostic accuracy determined by single-variate ROC curve analysis for correct characterization of malignant vs. benign FLL in the entire study population (A), in lesions with a diameter of ≤2 cm (B), lesions with a diameter >2 cm (C), in lesions with a diameter of ≤1 cm (D) and lesions with a diameter >1 cm (E).
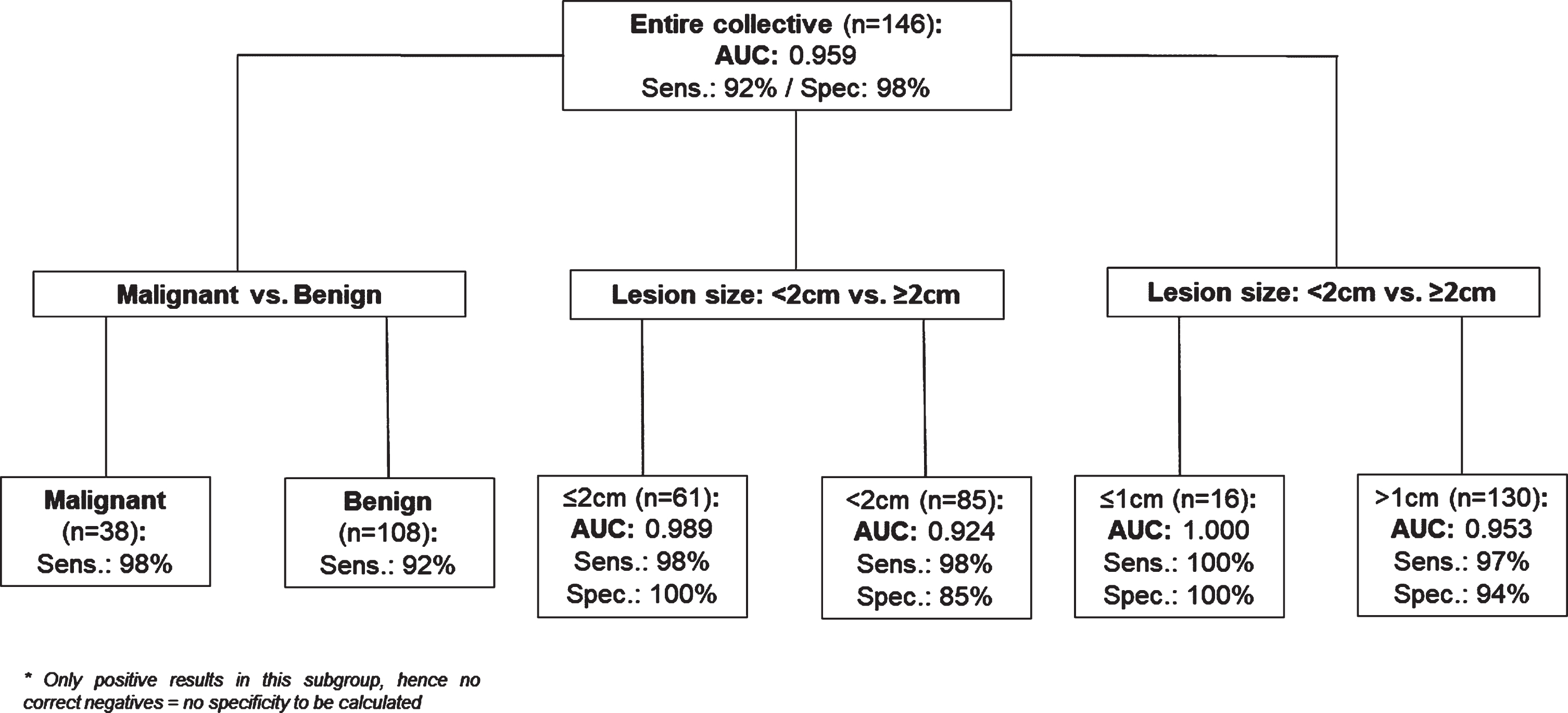
Flowchart – Results of the entire population and divided into subgroups.
Subdivided into malignant (n = 38) versus benign (n = 108) lesions, CEUS achieved a sensitivity of 92% (95% -CI, 78–98) in the malignant subgroup and 98% (95% -CI, 93–99) in the benign subgroup. The malignant subgroup included 31 metastases, identified with 90% sensitivity (95% -CI, 74–97) and seven HCC with 100% sensitivity. Most benign lesions were hemangiomas (n = 79), which were identified correctly with 99% sensitivity. Of note, 6.75% (5/74) of all hemangiomas were defined as atypical (hyalinized/sclerosed hepatic hemangioma or additional fatty infiltration) showing inhomogeneity and mixed echogenicity on B-mode US. The second most common benign lesions were FNH (n = 19). Among them, complex cysts (n = 7) were detected with 100% sensitivity. The data are summarized in Table 2.
Diagnostic accuracy of contrast-enhanced ultrasound (CEUS) in entire study population and in subgroups with benign / malignant lesions and lesion <2 cm vs. ≥2cm
Diagnostic accuracy of contrast-enhanced ultrasound (CEUS) in entire study population and in subgroups with benign / malignant lesions and lesion <2 cm vs. ≥2cm
Abbreviations: AUC denotes area under the curve; PPV, positive predictive value; NPV, negative predictive value; HCC, hepatocellular carcinoma; FNH, focal nodular hyperplasia; RN, regenerative nodule.
For small FLL, defined as lesion diameter <2 cm, CEUS achieved a sensitivity of 98% (95% -CI, 87–100), a specificity of 100% (95% -CI, 100–100), a positive predictive value of 100%, and a negative predictive value of 94%. ROC analysis yielded an AUC of 0.951 (Fig. 1b). For lesions ≥2 cm, AUC decreased to 0.924 due to a decrease in specificity from 100% to 86% (95% -CI, 87–100). Sensitivity was 98% (95% -CI, 81–100) (Table 2 / Figs. 1c and 2).
Lesion diameter -≤1cm vs. >1cm
For FLL ≤1 cm CEUS achieved a sensitivity of 100%, a specificity 100%, a positive predictive value 100% and a negative predictive value of 100%. Calculated ROC-analyses reported an AUC of 1.00 (Fig. 1d). For lesions >1 cm AUC decreased to 0.953, due to a lack of specificity from 100% to 94% (95% -CI, 79–99). Sensitivity was 97% (95% -CI, 91–99) (Table 2 / Fig. 1e).
Discussion
In this study CEUS is a highly accurate diagnostic imaging tool for characterizing FLL as malignant or benign, especially in patients with liver lesions previously classified as unclear based on cross-sectional imaging findings. Our findings may contribute to the importance of ensuring broad availability of CEUS and improving training programs.
The primary endpoint of our study was to assess CEUS in terms of its ability to classify unclear FLL as malignant or benign. In the entire study population, we found CEUS to have an astonishingly high diagnostic accuracy with an AUC of 0.959 and 92% sensitivity and 98% specificity. The results are in line with one of the first analyses of FLL performed over ten years ago in 68 patients by Soye et al., who reported similar levels of accuracy (95% sensitivity and specificity) [6]. Nevertheless, doubts about correct identification of some entities by CEUS still exist [8].
For a long time, the benefit of CEUS was doubted because of the risk of misdiagnosing HCC as cholangiocarcinoma [8, 24]. Newer studies using more refined analysis of contrast dynamics report more convincing results regarding the ability of CEUS to correctly identify HCC. Applying these refinements, Terzi et al. found a PPV of 98.5% for HCC in a retrospective multicenter study of more than 1000 patients while sensitivity was 62% [25]. Due to lower detection rates, however, ceMRI and ceCT are still the reference standard in detecting and staging HCC. CEUS is recommended in patients with contraindication to ceMRI or ceCT or previous inconclusive findings in these modalities [8, 26]. We determined levels of diagnostic accuracy separately for malignant and benign liver lesions. For malignant lesions (n = 38), sensitivity was 91% with a PPV of 100%, while seven of the malignant lesions were HCC. In these seven HCC lesions, we achieved 100% sensitivity and PPV. The remaining 31 malignant lesions were metastases, detected with 90% sensitivity. Unlike HCC lesions, metastases do not have defined washout times and dynamics. Therefore, we estimate them to be the most difficult to diagnose correctly with contrast-enhancing imaging in general. In patients with hepatic metastasis though, CEUS does not have to diagnose the correct entity but to define the lesion as malignant and to reliably differentiate it from HCC and benign entities for further management and treatment planning (Fig. 3). Of course, our patient population was pre-sorted as all lesions were unclear FLL based on prior imaging. Nonetheless, we think that 90% sensitivity for correct detection of metastasis is a promising result.

Contrast-enhanced ultrasound (CEUS) examination of an 80-year-old male patient with a history of urothelial carcinoma and a correctly diagnosed, histopathologically proven well-differentiated hepatocellular carcinoma (HCC) (white circle). CEUS was performed after injection of 1.6 ml SonoVue® (Bracco Imaging, Milan): a) Inhomogeneous, hypoechogenic focal liver lesion (FLL) in right liver lobe. b) Heterogeneous hyperenhancement in arterial contrast phase at 19 sec after contrast agent injection. c,d) No relevant washout in portal venous contrast phase at 87 sec after contrast injection (c) and discrete washout in late phase at 4:10 min after contrast injection (d).
For identification of benign lesions, sensitivity was even higher with 98% for all 109 patients. Needless to say that the 74 hemangiomas in our population strongly influenced our results by achieving high sensitivity levels, as CEUS in hemangioma in the choice of imaging modality (besides CT and MRI) and is even recommended in oncologic patients or those with liver disease [1]. FNH was the second most common benign liver lesion. In FNH MRI has still the highest diagnostic accuracy with levels of specificity of up to 100%. Nevertheless, sensitivity is degraded, especially by the absence of a central scar in small FNH [1, 27]. Two other studies emphasized diagnostic accuracy in FNH lesions smaller than 3.1–3.4 cm for CEUS but also found accuracy to decrease in larger lesions [28, 29]. In our study, CEUS correctly classified all 19 FNH as benign (sensitivity: 100%). Soussan et al., who compared the diagnostic performance of CEUS and MRI, concluded that the two modalities should be used as complementary tools to improve diagnostic accuracy in inconclusive cases [27]. As demonstrated by Beyer and colleagues in a collective of 83 patients, the number of false-negative results can be decreased using a combination of the CEUS and MRI with liver specific contrast medium [30]. Furthermore, the combination of Shear wave velocity (elastography), Alpha-fetoprotein (AFP) and enhancement rate resulted in a better diagnostic performance distinguishing between benign and malignant liver lesions compared to the use of any single technique or the combination of any two of these parameters [31].
Our study findings indicate, that CEUS performed by an experienced investigator may be a sufficient tool to clarify unclear cross-sectional imaging findings also in cancer patients.
Sporea et al. demonstrated similar accuracy for differentiation between malignant and benign liver lesions in tumors with diameter ≤2cm and those with diameter >2cm [32]. While cross-sectional imaging modalities are limited in small lesions due to failure to visualize specific contrast enhancement patterns, CEUS is a real-time examination with the ability to demonstrate typical contrast enhancement pattern in arterial phase and washout in the late contrast phase (Fig. 4). Thus, our results indicate that CEUS is not only a tool for characterization of single liver lesions but may also be useful in the detection of smaller malignant lesions based on enhancement patterns with late washout. Like Sporea et al. we also dichotomized lesion size into <2 cm vs. ≥2 cm [6]. While CEUS had nearly perfect diagnostic accuracy in smaller lesions (AUC: 0.989), its performance decreased in larger lesions due to lower specificity. This is consistent with the observation of Roche et al. and Bertin et al. who also concluded that the diagnostic accuracy of CEUS depends on lesion size and decreases with increasing size which may be related to higher variability and more heterogenicity of contrast enhancement patterns [28, 29]. The results are also in line with Seitz and Strobel et al. who investigated the accuracy in FLL in a multicentric design based on indefinite diagnosis on B-mode ultrasound and power Doppler ultrasound [33]. Nevertheless, accuracy about differentiating atypical hemangioma, some hepatocellular adenoma subtypes from hepatocellular remains a problem and has a potential of diagnostical distortion. The combination of CEUS and MRI may be able to solve the problem. As mentioned above Beyer et al. compared the performance of CEUS vs. MRI and achieved comparable levels of accuracy, also concluding that both methods are reliable and should be combined [30].
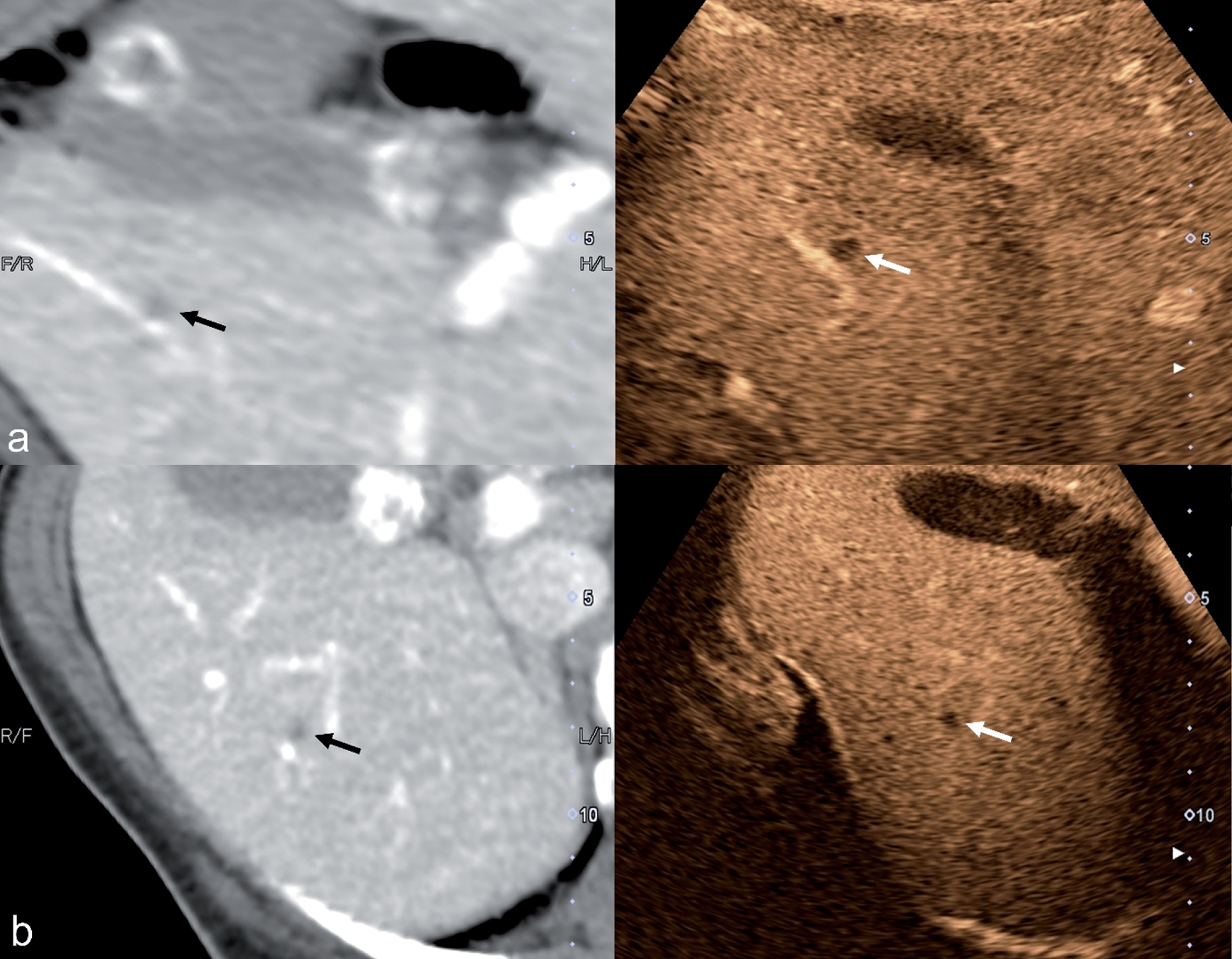
Contrast-enhanced ultrasound (CEUS) examination after injection of 1.6 ml SonoVue® (Bracco Imaging, Milan): of a 66-year-old female patient with breast cancer: Two small focal liver lesions (FLL)<7 mm remained unclear on prior single-phase contrast-enhanced computed tomography (ceCT). Hypodense lesions on single venous phase scan of the abdomen in the right liver (a and b / left image) obtained at initial CT staging. Both lesions show no arterial hyperenhancement in using CEUS but demarcation with washout in portal venous phase after 62 sec (a, right side) and 66 sec (b, right side). Therefore, these lesions were correctly diagnosed as breast cancer metastases, ruling out small benign cystic lesions. This diagnosis was confirmed by tumor progression and subsequent liver biopsy.
In small lesions according to the EFSUMB Guidelines defined as ≤1 cm [22], CEUS showed an excellent performance in our study cohort for both detection and differentiation of benign and malignant based on washout during parenchyma phase. Nevertheless, the results do not reflect the accuracy of US machines used in the clinical routine but the use of ultra-wideband multi-frequency convex transducers in combination with an experienced investigator may influence this outcome. However, due to the missing wash-out specifically in small lesions CEUS may have the same limitations as all US techniques, f.e. in patients with extreme meteorism and obesity, especially in the visualization of small and deeply localized lesions. Therefore, CEUS is not suitable for all patients [34].
While several studies demonstrate similar diagnostic performance for CEUS and cross- sectional imaging modalities in the assessment of FLLs, an economic analysis found CEUS to be a cost-effective replacement for ceMRI: Westwood et al. concluded that the use of CEUS instead of ceCT was cost-effective in the characterization of incidentally detected FLLs, with similar costs and effects for the detection of liver metastases [35]. CEUS is safe and easy to perform and overcomes the limitations of gray-scale ultrasound and CCDS. Thus, CEUS has been introduced into the daily clinical routine because it is cost-effective and able to rapidly generate additional image without radiation exposure according to Westwood et al. [35]. Moreover, it is a safe tool because the contrast media applied has no cardiac or renal toxicity and can be used in patients with chronic renal failure and thyroid dysfunction. It is also noteworthy that microbubble contrast agents have a lower rate of allergic reactions (< 0.009%) compared to contrast media based on gadolinium or iodine and do not use [36–38].
The first limitation of this study is the user dependency and relatively high experience level needed when performing ultrasound in general and specifically CEUS. In this study all examinations were performed by a high-experienced radiologist (EFSUMB Level 3) with more than 15 years of experience using ultra-wideband Multi-Frequency convex transducers (Canon Aplio i-series) providing better imaging compared to standard transducers which may increase lesions detection and visualization of microbubbles or contrast enhancement pattern. Secondly, the collective was pre-selected in terms of unclear defined FLL. Third, the secondary readers were aware of the study design and patients diagnosis, however the first investigator was blinded to the final diagnosis.
Conclusion
The relevance of CEUS imaging in the assessment of both malignant and benign liver lesions has increased dramatically over the past decade. In this study CEUS characterized FLL correctly as malignant or benign with high diagnostic power in a population of patients with inconclusive cross-sectional imaging findings. We recommend CEUS for further lesion characterization in cancer patients when small lesions remain unidentified using single- and biphasic contrast dynamics at initial staging. CEUS not only had added diagnostic value for lesion detection but also for classifying FLL as either malignant or benign, especially in small lesions, while its specificity in larger lesions remains limited.