
Abstract
BACKGROUND:
Contrast-enhanced ultrasound (CEUS) has been used as an additional imaging technique in order to clarify rare focal splenic lesions (FSL). CEUS is a safe and cost-effective modality for assessment of perfusion.
OBJECTIVE:
To validate contrast enhancement pattern and evaluate the diagnostic accuracy of CEUS in unclear FSL.
METHODS:
CEUS examinations of the spleen in 50 patients between 2012 and 2018 were included in the study. Examinations were performed using B-mode, colour-coded Doppler ultrasound (CCDS) and CEUS after injection of sulphur hexafluoride microbubbles and interpreted in consensus by two experienced radiologists. Reference standard was defined as histopathological report and clinical course (treatment response, long term follow up).
RESULTS:
All patients were successfully examined by CEUS without an adverse reaction. CEUS presented the correct differentiation of benign and malignant alterations in 49/50 (98%). Lesion washout was found in all malignant but also 16.7% of all benign lesions. Matched to the histopathological report and clinical follow up, CEUS represented a sensitivity of 100% (95% -CI, 57–100), a specificity of 98% (95% -CI, 88–100), a positive predictive value (PPV) of 83% (95% -CI, 44–97) and a negative predictive value (NPV) of 100% (95% -CI, 92–100).
CONCLUSION:
CEUS may provide additional information by visualization of dynamic contrast enhancement pattern to differentiate benign and malignant lesions. Nevertheless, established criteria for malignancy (early enhancement or washout) in FSL should be considered with caution since they are also found in benign lesions.
Introduction
Contrast-enhanced ultrasound (CEUS) is used in a variety of clinical patterns and has recently shown its effectiveness for characterization of focal lesions [1]. CEUS is easy to perform and a cost-effective choice compared to cross sectional imaging for characterization of lesions with a lower occurrence of allergic reactions than gadolinium or iodine [2]. Using the high accuracy of microbubble contrast agents, the visualization and differentiation of liver lesions and their detection rates has improved recently [3, 4]. Therefore, CEUS has been recommended within guidelines by the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) in characterizing unclear findings of focal liver lesions in computed tomography (CT) and magnetic resonance imaging (MRI) [5]. Solid focal splenic lesions (FSL) are mostly clinically silent and detected incidentally by ultrasound (US). Thus, FSL represent a relatively rare occurrence compared to lesions of the liver or kidney. Although most of these lesions are known as benign lesions such as hemangioma, their differentiation from malignant tumors might be challenging and should be confirmed before they can be disregarded [6]. Malignant alterations such as metastases of the spleen are relatively uncommon with a low incidence of 1.1% to 1.3% of splenectomy specimens [7]. Because of limitations in differentiating benign from malignant lesions by B-mode ultrasound, CEUS has become an additional option that is equivalent to CT or MRI [8, 9]. Although several studies with focus on the use of CEUS in abdominal trauma and splenic injury are published, data of diagnostic performance in non-traumatic splenic alterations is limited [10–13]. In diagnostic workup of FSL, cross sectional imaging is often mandatory to clarify clinically important differential diagnosis [14–16]. Although B-mode and colour-coded Doppler ultrasound (CCDS) are well known tools for detection of focal lesions in general, B-Mode US of the spleen is limited for depicting and characterizing focal lesions by a low contrast between the lesion and normal parenchyma. However, the CEUS features of benign vascular splenic neoplasms are variable [11–13] and require further investigation. Therefore, the aim of this single-center study was to validate enhancing pattern and diagnostic performance for differentiating splenic alterations on real-time CEUS.
Materials and methods
Study cohort
This retrospective study was approved by the local institutional ethical committee (EA4/148/18). Oral and written informed consent of all patients was obtained before examination. All study data were collected in compliance with the principles expressed in the Declaration of Helsinki 2002.
A total of 56 patients between 2012 and 2018 received an ultrasound examination of the spleen using B-mode, CCDS and CEUS. While only patients with complete follow up data were included in the final retrospective analysis, six patients were excluded due to loss of follow up. An active malignancy was defined as active cancer or anti-tumor therapy within the last 6 months or metastatic state at time of examination.
CEUS examination protocol
For gray-scale B-mode, the spleen was examined with a 1–6 MHz convex array transducer looking for detection, lesion size, echogenicity and homogeneity of the lesions using high-end ultrasound systems (Aplio500/Aplio i900; Canon Medical Systems Corporation, Tochigi, Japan). Colour-coded and Power Doppler ultrasound were employed to determine vascularization of the masses. Spleen was examined in modified longitudinal and transversal planes, if necessary, also by inter- and trans-costal scanning in deep inspiration and with optimized scanning positions.
CEUS examinations were performed during clinical routine using high-end ultrasound systems with up-to-date CEUS specific protocols available at the time of the examination. The examinations were performed at 1–6 MHz using i8X convex array transducer (Canon, Otawara, Japan). Ultrasound B-mode images were optimized using spatial compounding, frequency-based compounding, ApliPure™ level 5, differential Tissue Harmonic Imaging (dTHI©), and Precision Imaging© with level 4 Speckle Reduction (SR). CEUS images were performed at 1 to 5 MHz, 10fps. Each ultrasound system was configured with a very low MI (0.06 to 0.07) to avoid early microbubble-destruction. A bolus of 1.2–2.4 ml of ultrasound contrast agent (SonoVue®, Bracco Imaging, Milan, Italy) was repeatedly injected up to three times until satisfying cine loops were acquired. Baseline B-mode US, CCDS and CEUS (i.e. qualitative assessment of contrast enhancement pattern) were performed by a single high-experienced radiologist with more than ten years’ experience in CEUS (EFSUMB level 3). The loops and images were read by two experienced radiologists in consensus.
Image interpretation
All B-mode US images, CCDS and CEUS loops were retrospectively evaluated in consensus by two experienced radiologists (M.H.L., T.F.), one of them EFSUMB level 3 examiner. B-mode US features were homogenicity, echogenicity, lesion shape, maximal lesion size and number of lesions. In case of more than one lesion, the reference lesion in CEUS examination was used for evaluation of lesion size and vascular pattern. CCDS included central, peripheral or no hypervascularization. CEUS features included early arterial contrast enhancement, contrast enhancement compared to the surrounding splenic tissue (hyper- or hypoenhancement), wash-out during parenchyma phase and contrast enhancement pattern (peripheral-nodular, centrifugal, centripetal, general hypoenhancement compared to regular surrounding tissue).
Reference standard
All pathologies underwent imaging follow-up (35/50 ceCT, 12/50 ceMRI, 3/50 CEUS) and clinical surveillance including paraclinical parameters (laboratory tests, tumor markers etc.) served as reference standard. Five out of these 50 patients underwent both additional imaging and surgical exploration/biopsy with the respective histopathologic results serving as reference standard. A minimum follow-up was performed up to one year. Negative tumor markers with stable or diminishing lesion size after one year were considered to indicate a benign nature of the lesion. All radiological reports were approved by board-certified radiologists.
Multisclice CT protocol
Overall, 35/50 patients underwent multiphase CT examinations (arterial, and/or portal-venous and venous/delayed phase) using a standard protocol with a 64–128 detector CT scanner (Siemens Medical Systems, Forchheim, Germany), a minimum slice thickness of 0.625 mm and reconstruction interval 2 mm. The contrast agent was injected into an antecubital vein as a bolus, using a dual head power injector with a flow rate of 4,5–5 ml/s. 100–120 ml (Ultravist®, Bayer Healthcare, Berlin, Germany) with an iodine concentration of 370 mg/ml was administered, followed by 50 ml saline. The acquisition direction was cranio-caudal.
MRI protocol
MRI was performed with 1.5 T and 3.0 T systems using phased-array body coils in 12/50 patients. The examination protocols comprised T2-weighted (w) standard 2D sequences with and without fat saturation (FS) and T1-w unenhanced 2D sequences with and without FS (including in-/opposed phase technique). T1-w 3D sequences with FS were acquired in breath hold technique before and during arterial, portal venous, and venous phase, respectively after intravenous application of Gadubutrol acid (Gadovist, Bayer Pharma, Berlin Germany; body weight adapted; manual or automatic injection at approximately 1–2 mL/s flow rate followed by 40 mL saline flush).
Statistical analysis
Continuous variables were tested for normal distribution using the Kolmogorov-Smirnov-test; variables not following a normal distribution are reported as median and interquartile range (IQR) and were compared using the Mann-Whitney U-Test. Categorical variables were compared using student’s t-test or chi2 test, as appropriate. The obtained CEUS results and matched histopathological reports from each patient were analyzed retrospectively for diagnostic accuracy by testing sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV).
A two-sided significance level of α 0.05 was defined appropriate to indicate statistical significance. All statistical analyses were performed using the SPSS software (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.).
Results
All patients were successfully examined by CEUS without an adverse reaction (median age 55 years [IQR, 33–69]; 59.6% male patients). Baseline characteristics of all study patients (n = 50) and further imaging findings in focal lesions (n = 35) excluding cystic lesions, infarctions or hematoma (which do not represent specific contrast enhancement pattern) are presented in Table 1.
Baseline characteristic and imaging findings of all study patients stratified to tumor dignity
Baseline characteristic and imaging findings of all study patients stratified to tumor dignity
Continuous variables are given as median (Interquartile range), categorical variables are given as absolute/total numbers (n/N) and percentages in brackets. Abbreviations: CCDS denotes colour Doppler ultrasound; CEUS, contrast-enhanced ultrasound.
Out of 50 patients with splenic alterations, CEUS demonstrated five cases with malignant splenic alterations. All five malignant focal lesions demonstrated complete hypoenhancement compared to regular surrounding tissue and progressive washout during parenchyma phase (Fig. 1), while only one lesion (Mb. Hodgkin) presented early peripheral contrast enhancement in arterial phase. In one case, the suspicious malignant alteration demonstrated by CEUS was elucidated in ceMRI and histopathologic confirmed as sarcoidosis. In patients with history of trauma (n = 4) CEUS ruled out a splenic laceration in all cases, confirmed by cross sectional imaging. While two of these patients had additional inconclusive findings (focal lesion) on ceCT, CEUS revealed one incidental finding of a diffuse B-cell lymphoma (presented with hypoenhancement compared to splenic tissue and washout during parenchyma phase, Fig. 2) and one hemangioma, which was confirmed by additional ceMRI and follow-up. Moreover, CEUS ruled out focal spleen lesions in five patients with unclear splenomegaly (n = 1) and suspicion of lymphoma (n = 3) or infarction (n = 1) to elucidate unclear B-mode ultrasonography findings in external institutions. Three patients represented atraumatic spontaneous splenic rupture after surgery (two patients with sigmoid colon perforation and one patient with ovarial cancer) confirmed by CEUS. (Fig. 3)
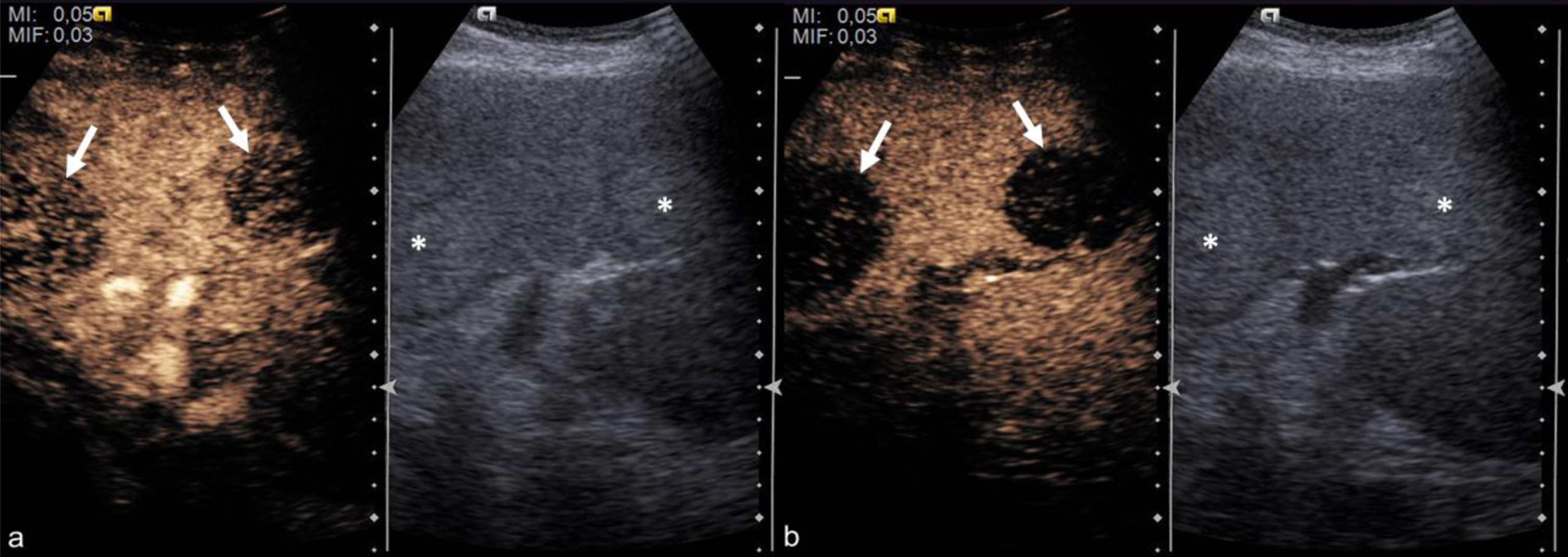
CEUS of the spleen in a patient with hair cell leucemia and splenomegaly. CEUS contrast enhancement pattern showing hypoenhancement in arterial phase after 20 seconds (a) and progressive washout in parenchyma phase after 55 seconds (b). Abbreviations: CEUS denotes contrast-enhanced ultrasound.
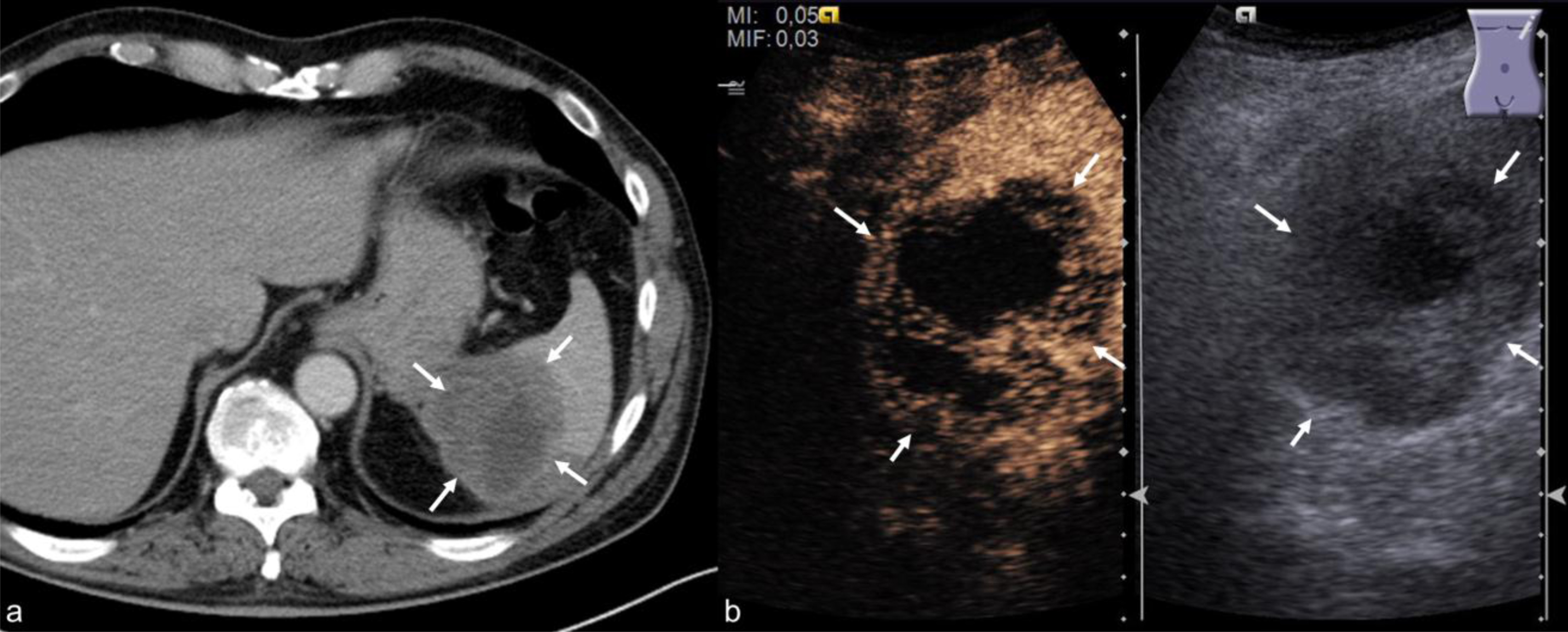
Patient with history of trauma 3 weeks prior ceCT and CEUS. Hypodense, inhomogeneous area (borders marked with arrows) of the spleen on ceCT (a) showed inconclusive findings in differentiation of hematoma or focal lesion, while CEUS clearly depicted solid contrast-enhancing tissue within the area (b) and stated malignant lesion instead of hematoma. The lesion was histopathological confirmed as a B-cell lymphoma. Abbreviations: ceCT denotes contrast-enhanced computed tomography; CEUS, contrast-enhanced ultrasound.
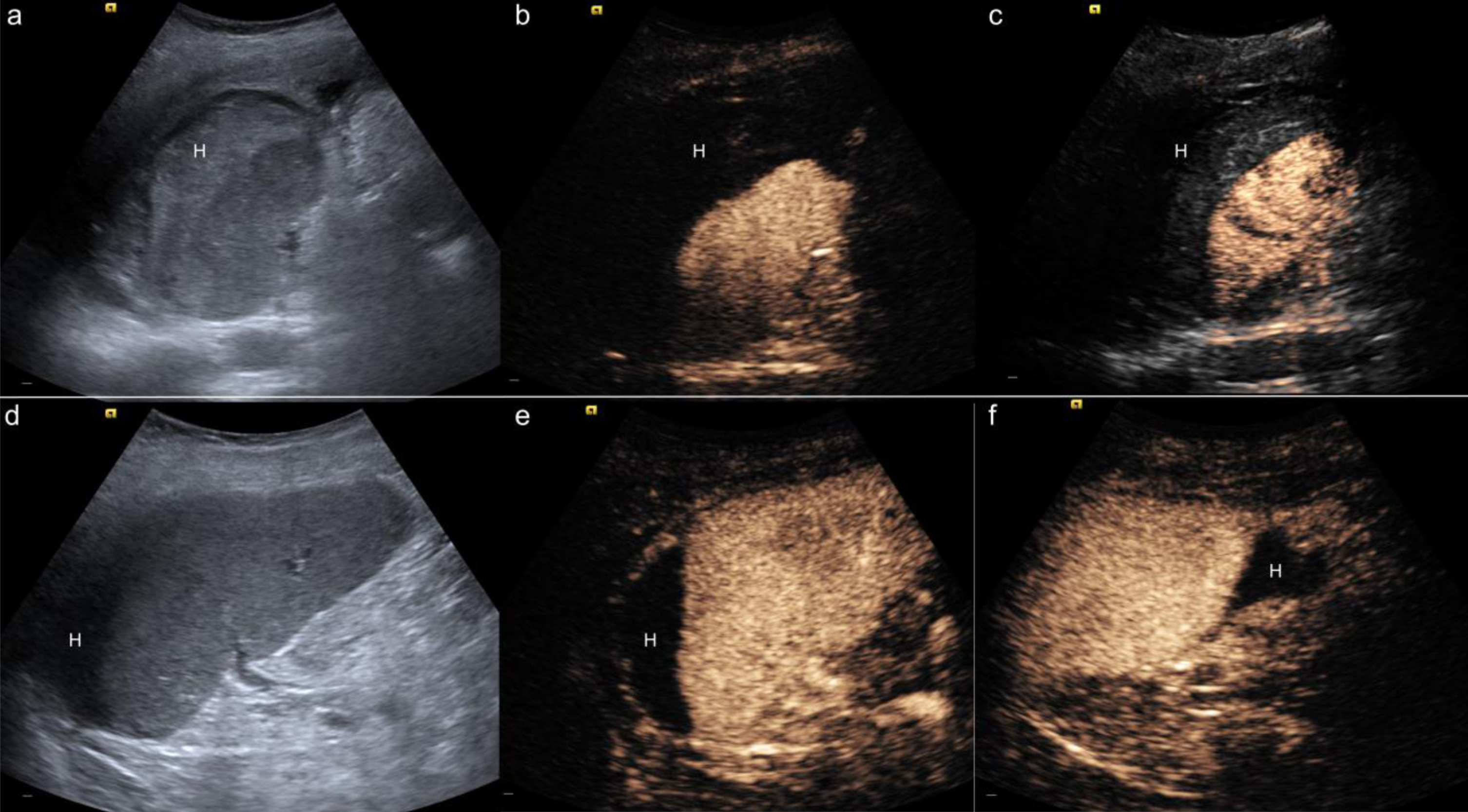
Two representative cases of spontaneous hematoma (H) after surgery in patients with ovarian cancer (a–c) and sigmoid perforation (d–f). a–c) Hyperechogenic area around the spleen showed no contrast enhancement on CEUS after surgery in a patient with ovarian cancer. d–f) In contrast, hypoechogenic area around the spleen showed no contrast-enhancement and showed hematoma after surgery of sigmoid perforation. Abbreviations: CEUS denotes contrast-enhanced ultrasound.
Overall, 13/50 patients with a FSL had an active malignancy (n = 11/50) and two patients history of cancer (one Seminoma, one acute myeloid leucemia). In these patients with incidental findings on cross-sectional imaging (ceCT = 10/13 patients, ceMRI = 3/13 patients), CEUS ruled out malignancy in 10/13 lesions presenting four hemangiomas, three cystic lesions, one splenoma (Fig. 4) and two splenic infarctions (Fig. 5) while three patients had confirmed infiltration of lymphoma (Mb. Hogkin, non-hodgkin lymphoma and hair cell leucemia, Fig. 1).
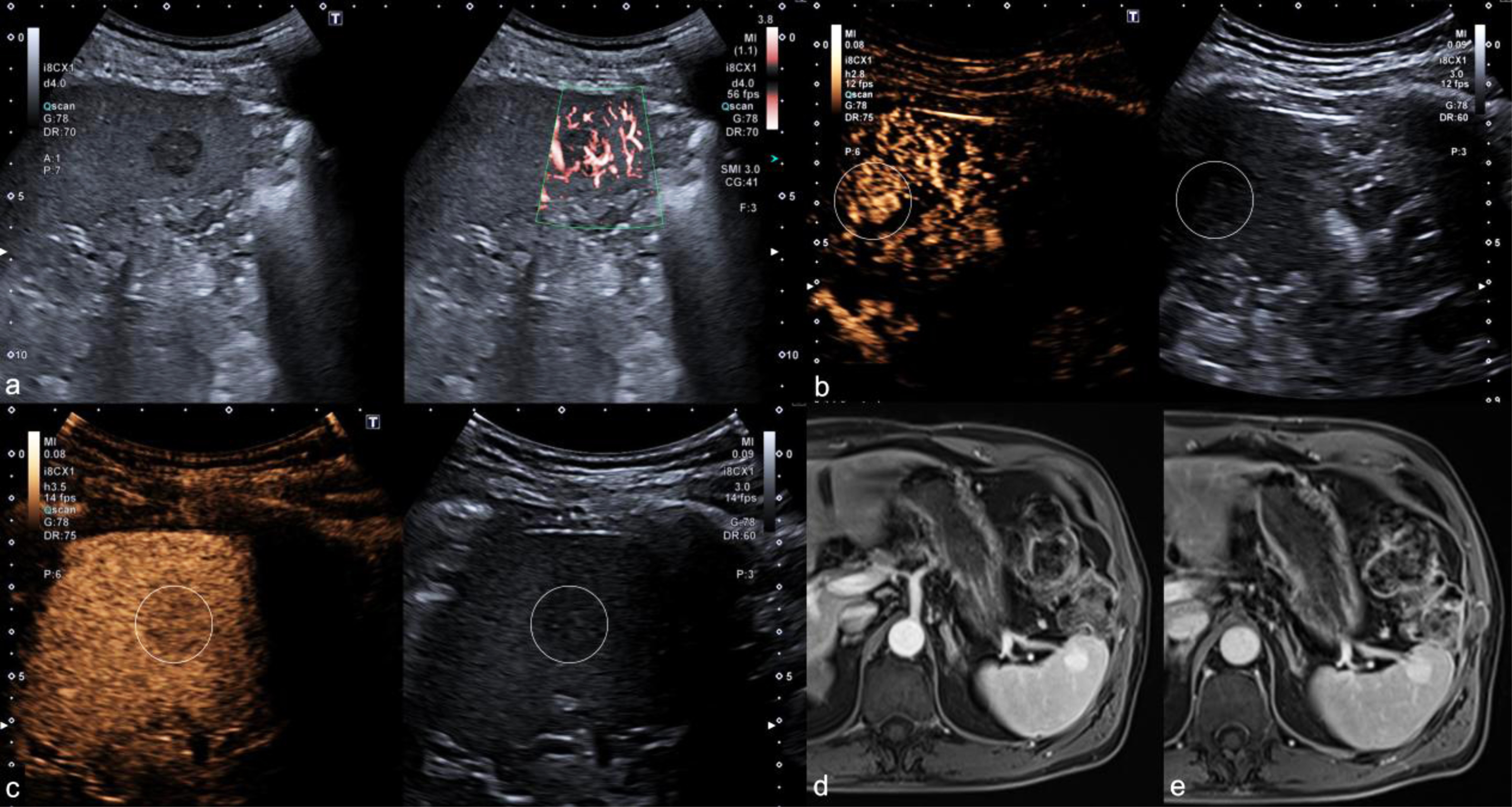
Representative case of benign splenoma. a) Hypoechogenic lesion of the spleen showed prominent peripheral vascularization using high-sensitive Doppler ultrasound SMI. b) CEUS showed early contrast enhancement in arterial phase 12 seconds after contrast application. c) Minimal lesion washout during late phase 90 seconds after contrast application on CEUS. d–e) Additional MRI depicted hyperenhancement in both arterial and venous contrast-phase. Abbreviations: SMI denotes Superb Microvascular Imaging; CEUS, contrast-enhanced ultrasound; MRI, magnetic resonance imaging.
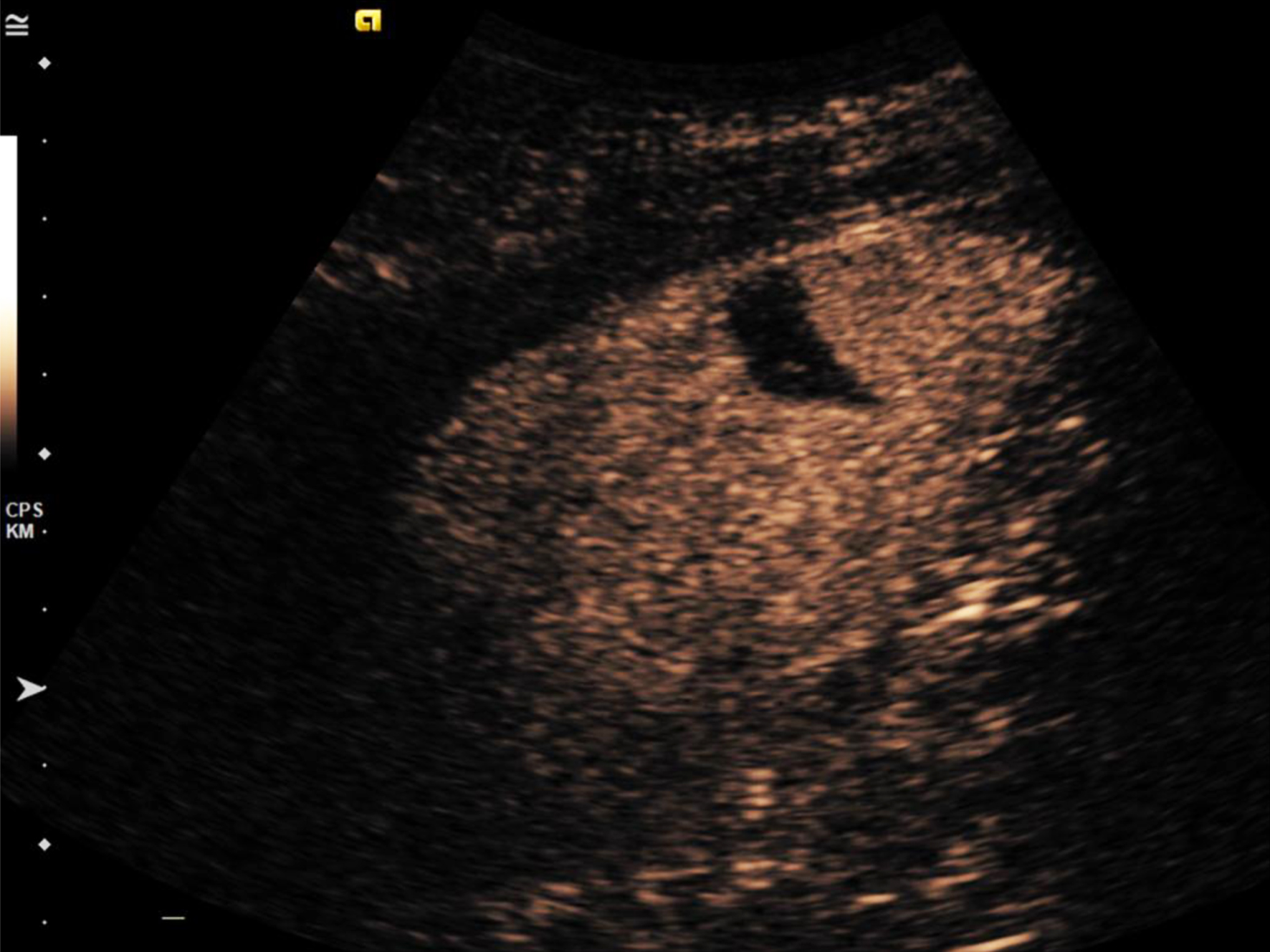
Splenic infarction on contrast-enhanced ultrasound. Splenic infarction demonstrated by a wedge shaped area of non-contrast enhancement in a patient with pancreatic cancer and chemotherapy.
Lesion washout in parenchyma phase was present in all malignant alterations (n = 5) and also in benign lesions such as two hemangiomas, one hamartoma and a rare case of sarcoidosis, all confirmed by cross sectional imaging and histopathology (Table 2). While only one case of Hodgkin lymphoma presented with early contrast enhancement in arterial phase, early enhancement was more frequently seen in benign FSL (n = 13; six hemangiomas, four splenomas, two hamartomas and one case of sarcoidosis). CCDS was able to show hypervascularization in nine benign lesions with early hyperenhancement on CEUS. Overall, 11/35 FSL showed centripetal contrast filling (all benign lesions), four hemangiomas demonstrated with centrifugal contrast filling. Two lesions which final diagnosis remained unclear in both CEUS and cross-sectional imaging (considered to indicate a benign nature with stable lesion for minimun of two years follow) showed no clear contrast enhancement pattern in CEUS and were isoechogenic compared to the surrounding splenic tissue without lesion washout.
Contrast-enhancement pattern of solid focal spleen lesions*
*Focal splenic alterations excluding cystic lesions, infarction and hematoma.
CEUS presented the differentiation diagnostic accuracy of 98% with correct differentiation of benign and malignant pathologies in 49/50 patients missing one case of sarcoidosis rated as malignant on CEUS. When matched to the histopathological report and clinical follow up for evaluation of malignancy, CEUS represented a sensitivity of 100% (95% -CI, 57–100), a specificity of 98% (95% -CI, 88–100), a positive predictive value (PPV) of 83% (95% -CI, 44–97) and a negative predictive value (NPV) of 100% (95% -CI, 92–100).
Our study demonstrates an excellent performance of additionally used CEUS in differentiation of benign and malignant alterations of unclear splenic pathologies. CEUS presented the correct differentiation of benign and malignant pathologies in 49/50 (98%). A sensitivity of 100%, a specificity of 98%, a PPV of 83% and a NPV of 100% calculated in this study demonstrated that CEUS is not only easy and fast to perform but also a feasible addition to B-mode ultrasound and CCDS. This diagnostic performance of 100% sensitivity was comparable to a recent published study by Schwarze and colleagues, also interpreted by a high-experienced radiologist (EFSUMB level 3) [17] and higher compared to results by Stang et al. (Sensitivity 94%, specificity 84%) and Yu et al. (Sensitivity 91,1%, specificity 95%). All patients were examined without any adverse reaction (e.g. allergic reaction). Moreover, it is a safe tool because CEUS examinations do not use radiation and the contrast agent applied has no renal, thyroid or cardiac toxicity.
Traumatic pathologies
B-mode US and CCDS can demonstrate morphologic and hemodynamic changes in splenic lacerations. Additionally, CEUS is a well-established criterion for the diagnosis of traumatic splenic lesions [18]. Therefore real time contrast enhancement pattern on CEUS may provide further diagnostic information if B-Mode ultrasound appearances are uncertain [19, 20]. In our study, CEUS ruled out splenic laceration in all patients and may serve as a feasible tool especially for young patients with isolated splenic trauma. During follow-up CEUS can depict a change in size or shape of infarction [21]. Changes in lesion features during follow-up confirm the differential diagnosis from other splenic lesions and allow conservative management in these patients.
Evaluation of unclear splenic lesions
CEUS has shown advantages over contrast-enhanced MRI including unmatched temporal resolution due to continuous real-time imaging in detecting unclear renal lesions [22]. Higher sensitivity has been shown in combining CEUS with MRI in the characterization of focal liver lesions [23] while CEUS and MRI alone have shown equal results in differentiating liver lesions [9]. Compared to CEUS, MRI is more time consuming especially in the diagnostic workup of acute alterations and may not be widespread available in smaller non-university hospitals. Our study showed excellent results by CEUS in combination with prior ceCT or ceMRI and knowledge of clinical information, indicating that incidental findings on B-mode US may get a fast and easy additional imaging evaluation using CEUS as secondary imaging modality. Furthermore, incidental findings on single-phase ceCT could benefit from additional fast and cost-effective CEUS imaging for evaluation of lesion perfusion.
Data of the differentiation of focal splenic lesions using CEUS is rare. CEUS allows visualization of splenic microvascularization and may thus aid in the preoperative assessment of splenic lesions with hypovascularization in the parenchymal phase as an important feature in the diagnosis of malignancy [24]. Lesion washout in parenchyma phase was present in all malignant alterations (n = 5) and also in benign lesions such as two hemangiomas, one hamartoma and a rare case of sarcoidosis, all confirmed by cross sectional imaging and histopathology. Similar to Bachmann et al., CEUS was superior to CCDS in the visualization of vascularization especially in benign splenic lesions (43.3% hyperenhancement by CEUS vs. 31% hypervascularization by CCDS in benign lesions) [25].
Caremani et al. demonstrated that hypoenhancement of a focal splenic lesion had a positive predictive value of 87% for a neoplasia. Although late phase washout is a typical sign of malignant lesions, less pronounced washout could also be visualized in many benign lesions [1]. Therefore, clear differentiation between benign and malignant lesions due to contrast enhancement in CEUS is currently challenging [1, 13]. CEUS may be useful in the assessment of splenic lesions where CCDS comes to its limits because splenic tumours may appear avascular.
Benign lesions appear as anechoic masses or echogenic lesions due to gas or calcification [26]. Vascular tumors (hemangioma and hamartoma) are the most common benign lesions while secondary tumors (lymphoma and metastases) are the most common malignant lesions [27, 28]. While only one case of Hodgkin lymphoma presented with early contrast enhancement in arterial phase and progressive early washout during parenchyma phase, early enhancement was more frequently seen in benign FSL (n = 12; six hemangiomas, three splenomas, two hamartomas and one case of sarcoidosis). Although progressive centripetal filling is unusual in splenic hemangiomas [1], 11/35 FSL showed centripetal contrast filling (all benign lesions) whereof four hemangiomas demonstrated with centrifugal contrast filling.
While especially small situated hypoechoic tumors appear with short filling time or circumferential vessel with a rapid centripetal filling on CEUS, the visualization of specific contrast enhancement pattern in small lesion is limited [23, 26]. Lymphoma of the spleen could show a variety of morphologic findings and benign alterations like septic embolism could also mimic a malignant FSL. CEUS and evaluation of perfusion kinetics therefore allows a better detection especially of lymphoid lesions within surrounded splenic tissue [29, 30]. While two patients had inconclusive findings (focal lesion) on ceCT, CEUS revealed one incidental finding of a diffuse B-cell lymphoma in a patients after bike accident two weeks before examination with persistent left upper abdominal pain (presented with enhanced solid tissue compared to splenic tissue and washout during parenchyma phase, Fig. 2). Incidentally, lymphoid lesions may show a small irregular rim of enhancement during the early arterial phase [31, 32]. Furthermore, intralesional vessels and large areas of necrosis due to irregular neovascularization favor a diagnosis of malignancy, which may explain the different perfusion kinetics on time intensity curves [1].
While malignant lesions represented greater median tumor size (p = 0.342) and more often complete hypoenhancement (p = 0.421) in this study without reaching statistical significance (due to a small number of rare malignant lesions), washout on CEUS was seen in all malignant lesions (p = 0.001). Thus, differentiation of benign and malignant lesion may base on a combination of echogenicity, heterogenicity and contrast enhancement. The use of multiparametric US including shear wave elastography, microflow imaging and CEUS may be a promising tool in the diagnosis of splenic alterations in the future [33, 34]. CEUS could potentially avoid unnecessary biopsy of the spleen, which are associated with higher risk for bleeding due to high blood flow compared to liver biopsy. Furthermore, it represents a preferred modality for young patients with a low rate of allergic reaction and without use of radiation exposure.
Limitations
Due to the study design there are limiting factors of this work that need to be addressed. This study was designed as a retrospective, monocentric analysis with one high experienced radiologist evaluating spleen alterations using CEUS imaging; although it is questionable how a prospective approach would have raised quality. During period of time different ultrasound systems and probes were used for imaging studies in our institution. The multi-frequency ultra-wideband transducers used in this study cover the same bandwidth as two conventional transducers providing superior sensitivity and resolution for both near and far field in both B-mode US and CEUS. The ability shows the use of one transducer across a wider range of patient types, providing better imaging regardless of the patient conditions which may increase lesions detection and visualization of microbubbles. Although we assessed a broad spectrum of pathologies, we had rather small numbers of malignant lesions, which might influence statistical evaluation.
Conclusion
This single-center investigation of additional CEUS in unclear splenic alterations acknowledged that combination of CEUS and clinical information is a feasible and accurate tool to differentiate between benign and malignant alterations. Although FSL are often incidental findings on cross-sectional imaging, CEUS may provide additional information on vascularity providing real time contrast enhancement pattern and patients with contraindications to CT or MRI may benefit from this image modality. Nevertheless, established criteria for malignancy (early contrast enhancement or lesion washout) should be considered with caution since they are also found in benign lesions.
Footnotes
Acknowledgments
None.