
Abstract
BACKGROUND:
Platelet function analysis is crucial in assessing the hemostatic status to evaluate congenital and acquired platelet function defects. The Anysis-200 analyzer is a new automated lab-on-a-chip-based platelet function analyzer.
OBJECTIVE:
We aimed to evaluate a new platelet function analyzing system, the Anysis-200 in comparison to the Platelet Function Analyzer (PFA)-200 in cardiac patients.
METHODS:
Citrated blood was collected from 174 patients who visited the Department of Cardiology. The Anysis-200 consists of two kits, the microchips with collagen and epinephrine-coated membrane (C/EPI) or adenosine diphosphate-coated membrane (C/ADP). Platelet clogging in the Anysis-200 is measured by the blood migration distance obtained by a camera, which is compatible with the closure time in the PFA-200. We performed Anysis-200 and PFA-200 analyzers simultaneously and compared the results.
RESULTS:
The sensitivity and specificity of the Anysis-200 C/EPI kit in comparison to the PFA-200 C/EPI kit were 63.41% and 91.43%, respectively. Regarding the C/ADP kit, the sensitivity and specificity of the Anysis-200 were 58.97% and 74.29%, respectively. The agreement rate between the Anysis-200 and PFA-200 for C/EPI was 83.35% and 70.14% for C/ADP.
CONCLUSIONS:
The Anysis-200, which applies a novel method to detect platelet clogging, has shown moderate to fair agreement with the PFA-200. This test is potentially useful for screening cardiac patients with an abnormal platelet function.
Introduction
The instantaneous recruitment of platelets upon vessel damage prevents bleeding through the rapid formation of a platelet plug in physiological hemostasis. Platelets play an important role in maintaining normal hemo-stasis via various mechanisms. At the injured vascular region, an abnormal flow condition occurs, with high shear rates and platelet aggregation and adhesion during the pre-coagulation process [1]. Malfunction of these mecha-nisms can result in excessive bleeding. Platelet function tests have been used to evaluate congenital and acquired platelet function defects [2]. Platelet function tests have also been applied to monitor antiplatelet therapies, and to assess hemorrhage risk and the need for blood products in patients receiving antiplatelet medication in perioperative settings [3, 4].
There are various methods to analyze platelet function, and light transmission aggregometry (LTA) is regarded as the “gold standard” method [5]. However, LTA is labor intensive and time-consuming, which restricts its use in routine laboratory testing [6, 7]. More convenient point-of-care tests (POCTs) to analyze platelet function have been developed [8], including the Platelet Function Analyzer (PFA)-200 (Siemens, Mississauga, Ontario, Canada), the Multiplate analyzer (Roche Diagnostics, Rotkreuz, Switzerland), and the Plateletworks kit (Helena Laboratories, Beaumont, Texas, USA). Although these platelet function tests have been widely used, the POCT platelet function test remains poorly standardized, with agreements between tests reported to be 38.7% to 62.8% [9].
Recently, the Anysis-200 analyzer (RheoMeditech, Inc., Seoul, Korea), a POCT system for platelet function tests has been developed [10]. The Anysis-200 analyzer is an easy-to-use automated lab on-a-chip microfluidic system, which uses the migration distance (MD) of blood through a microchannel to analyze platelet adhesion and aggregation. The MD, which is comparable with the closure time (CT) obtained by PFA-200, is automatically analyzed based on the images obtained by a camera. The aim of this study was to evaluate the feasibility of the Anysis-200 in screening cardiac patients with abnormal platelet functions in comparison to the PFA-200, one of the most widely performed platelet function tests.
Materials and methods
Patient samples
Whole blood samples from a total of 174 patients were collected from the Korea University Guro Hospital between October 2018 and April 2019. Cardiac patients referred for PFA-200 collagen-epinephrine (C/EPI) and/or PFA-200 collagen-adenosine diphosphate (C/ADP) assay were included in our study. The exclusion criteria were as follows: platelet count <100×109 /L or >500×109/L; Hct <35% or >50% within the previous 6 months data; and abnormal PT and aPTT. Among the 174 samples, 146 were evaluated with the C/EPI kit, of PFA-200 and Anysis-200, and 144 were evaluated with the C/ADP kit of the PFA-200 and Anysis-200. The patients were divided into a normal and abnormal group based on the PFA-200 platelet function test results. The study protocol was approved by the Institutional Review Board of the Korea University Guro Hospital, and written informed consent was obtained from all the participants before enrollment into the study.
Blood sampling was carried out using 21-gauge needles and collected in 3.2% sodium citrate tubes (0.109 mol/l buffered sodium citrate, BD Vacutainer Systems, Franklin Lakes, NJ, USA) for PFA-200 and Anysis-200 assessments. After collection, the tubes were gently inverted (three to six times). During transportation, special care was taken to avoid platelet agitation, and the blood samples were stored at room temperature and analyzed after 30 min of collection.
Anysis-200 platelet function analyzer
Platelet function tests for the Anysis-200 analyzer were recently developed using a microchip-based system (Fig. 1). The microchip consists of the following three components: a rotating stirrer for shear-induced platelet activation, an agonist-coated microbead-packed tube for platelet-adhesion and -aggregation, and a running channel. A brief description of the microfluidic system operation is as follows. When vacuum pressure is applied in the test chip, the blood sample is aspirated into a sample chamber, on which agonists such as either epinephrine or ADP are coated on the top surface of the sample loading chamber. Then, the stirrer rotates, the agonists can be easily mixed with the blood sample, and platelets may be activated. In addition, due to the rotating rectangular-strip stirrer feature, shear-induced platelet activation may occur.
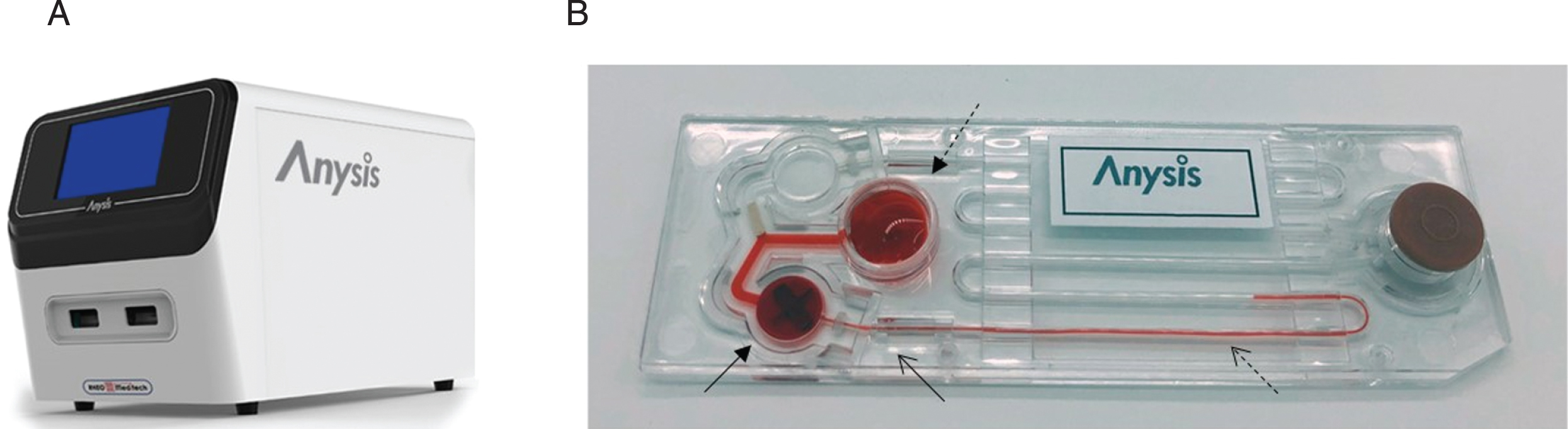
The Anysis-200 platelet function analysis system. This system includes the Anysis-200 hardware
After the mixing and shearing process, the blood sample is aspirated into the running channel, which includes the collagen-coated microbead-packed tube. Activated platelets may adhere on the collagen-coated surface, aggregate with one another, and eventually block the flow passage of the microbead-packed tube. Using a CCD camera, the blood sample MD is monitored and analyzed. The MD in the Anysis -200 test is comparable with the CT obtained by the PFA-200 test. The MD is represented in millimeters, whereas the CT is represented in seconds.
For each test, a total of 250μL of whole blood was pipetted into a sample loading chamber, and the MDs were automatically measured within four minutes. There are two types of Anysis-200 test kits, C/EPI- and C/ADP-coated membranes. The cut-off value for MD is 228 mm and 190 mm for C/EPI and C/ADP, respectively, according to the manufacturer’s instructions. Any measured values greater than the cut-off MD were considered abnormal.
Assessment on the PFA-200 (Siemens Canada, Mississauga, Ontario, Canada) was conducted using 800μL of from citrated blood sample with cartridges containing C/ADP- and C/EPI-coated membranes for platelet activation. The CT values (s), defined as the time taken by platelets to occlude the orifice and block the blood flow, were measured. Prolonged CTs were defined as CT > 250 s (C/EPI) and > 110 s (C/ADP), according to the manufacturer’s instructions. Any closure time greater than 300 s was reported as 300 s.
Statistical analysis
Normally distributed data were expressed as a mean±standard deviation. The sensitivity and specificity were analyzed considering the results from the PFA-200 as true positive and negative. Pairwise agreement between the two platelet function assays was assessed using Cohen’s kappa coefficient. Cohen’s kappa coefficient results were interpreted as follows: values ≤0, no agreement; 0.01–0.20, none to slight; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, substantial; and 0.81–1.00, almost perfect agreement [11]. P < 0.05 was considered statistically significant. All statistical analyses were performed using Medcalc version 12.1.4 software (Medcalc Software, Mariakerke, Belgium).
Results
Patient characteristics are shown in Table 1. For the PFA-200, the mean CT values were 127 s (range 72 to 300 s) for C/EPI and 98 s (range 62 to 175 s) for C/ADP. The coefficient of variation (% CV) values were 46.82% for C/EPI and 21.43% for C/ADP (Table 2). Among the 146 samples tested with the PFA-200C/EPI kit, 41 samples (28.0%) showed higher CT values than the cut-off (>250 s). Of the 144 samples evaluated using the PFA-200C/ADP kit, 39 samples (27.1%) resulted in CT values higher than the cut-off (>110 s).
Patient characteristics
Patient characteristics
Abbreviations: PFA-200, Platelet function analyzer-200; C/EPI, collagen-epinephrine; C/ADP, collagen-adenosine diphosphate.
The distribution of migration distance value and closure time analyzed by Anysis-200 and PFA-200
Abbreviations: C/EPI, collagen-epinephrine; C/ADP, collagen-adenosine diphosphate; SD, standard deviation; % CV, coefficient of variation.
The overall mean MD value of the Anysis-200 was 194 mm (range 119 to 268 mm) for C/EPI and 179 mm (range 112 to 268 mm) for C/ADP. Anysis-200 showed % CV of 23.20% and 27.37% for C/EPI and C/ADP kit, respectively (Table 2). The mean MD of the Anysis-200C/EPI kit was 177 mm (range 119 to 268 mm) and 235 mm (range 136 to 268 mm) in the normal and abnormal groups, respectively (Table 2). Regarding the MD of the Anysis-200C/ADP kit, the mean value was 167 mm (range 112 to 268 mm) and 209 mm (range 123 to 268 mm) in the normal and abnormal groups, respectively (Table 2). The distribution of CT and MD values among patients with or without coronary artery disease is shown in Supplementary Table 1.
Considering the results of the PFA-200 to determine the true positive and negative, a cut-off value equal to or greater than 228 mm for C/EPI and 190 mm for C/ADP indicated abnormal platelet results with a sensitivity of 63.41% (n = 26/41, 95% CI, 46.94% –77.88%) for C/EPI and 58.97% (n = 23/39, 95% CI, 42.10% –74.43%) for C/ADP. The specificities for C/EPI and C/ADP were 91.43% (n = 96/105, 95% CI, 84.35% –96.01%) and 74.29% (n = 78/105, 95% CI, 64.83% –82.32%), respectively.
The agreement between the results of the Anysis-200 and that of the PFA-200 varied between test kits. The Anysis-200C/EPI kit showed a higher agreement rate (83.35%; 95% CI, 76.54% –89.17%; Cohen’s kappa coefficient, 0.574) than the C/ADP kit (70.14%; 95% CI, 61.96% –77.47%; Cohen’s kappa coefficient, 0.305; Table 3).
Comparison of the Anysis-200 and PFA-200 results
Abbreviations: PFA-200, Platelet function analyzer-200; C/EPI, collagen-epinephrine; C/ADP, collagen-adenosine diphosphate; CI, confidence interval.
This is the first study to assess the use of Anysis-200 for screening patients with abnormalities in platelet function. Here, the performance of the Anysis-200 was comparatively evaluated with that of the PFA-200, one of the most widely used methods for platelet function assessment.
Recently, an increasing number of new assays for platelet function have been developed. The newly developed platelet function tests enable rapid on-site evaluation and have become important tools that are commonly used in clinical hemostasis diagnostics. The platelet function tests apply different methodologies to detect platelet aggregation in response to agonists. The PFA-200 is designed to be a surrogate of in vitro bleeding time, which monitors the decrease in blood flow rate as platelets form a hemostatic plug under high shear stress conditions in response to epinephrine or ADP. The parameter is measured as a CT [12]. The Multiplate analyzer applies an electrical impedance that measures the electrical resistance caused by platelet adherence and aggregation on the metal sensor wires of the Multiplate test cell [13]. Plateletworks is a method based on the platelet counting ratio technique, which compares platelet counts within a control ethylenediaminetetraacetic acid tube and after aggregation with platelet agonists within citrated tubes [14]. Although these different platelet methodologies have impacted the diagnosis and management of patients affected by inherited and acquired bleeding disorders, implementation of a platelet function test involving more than one method is recommended for reliable interpretation because platelet cells may be easily activated during blood sampling and a number of preanalytical variables can produce platelet artifacts affecting the different platelet functions [15–17].
The platelet function tests that use a microfluidic system, such as the PFA-200, mostly adopt once-through flow systems using a flow-induced shearing mechanism to activate platelets [18–21]. However, due to the inherent characteristics of a capillary flow, the shear stress distribution is not uniform and causes the heterogeneous activation of platelets, which may result in poor reproducibility. In order to homogeneously activate platelets, the Anysis-200 adopts a rotational Couette flow system, which is frequently adopted in rheometry for measuring viscosity. Our previous paper reported a custom-designed rectangular stirrer with an embossing rotation axis that can generate efficient mixing as well as suitable shear stress [22].
Comparison of the C/EPI and C/ADP kits of the Anysis-200 and the PFA-200 has showed moderate to fair agreement. The agreement rate was higher with the C/EPI (83.35%) than with the C/ADP kit (70.14%). According to the previous study, the agreement between the PFA-200 and Multiplate analyzer C/ADP kits was reported to be 51.30% (Cohen’s kappa coefficient –0.147) [9]. Regarding the PFA-200C/ADP and Plateletworks ADP kits, the agreement rate was 56.30% (Cohen’s kappa coefficient 0.089) [9]. The Multiplate analyzer and Plateletworks do not adopt EPI as an agonist; therefore, a direct comparison of the results is difficult. In accordance with data from the literature, the Anysis-200 showed better agreement with the PFA-200 compared to the Multiplate analyzer and Plateletworks. However, although relatively higher agreement between the Anysis-200 and PFA-200 was observed compared to other methods, the findings of this study show that the platelet function test results vary depending on the principle of the test and highlights that further standardization and quality control for platelet function tests are necessary for more reliable results in the future.
The limitation of this study is that we did not further confirm the samples, which showed discrepant results between the Anysis-200 and PFA-200, with other platelet function tests. Confirmation with light transmission platelet aggregometry would further support the feasibility of the Anysis-200 in comparison to the PFA-200. Moreover, this is a pilot study to assess the diagnostic performance of the Anysis-200 in the detection of patients with abnormal platelet function and further validation is necessary to define the specific applications of this test.
In conclusion, the new platelet function test system, the Anysis-200, showed fair to moderate agreement with the PFA-200, which is a better agreement compared to that of other previously developed assays. The Anysis-200 is a rapid, easy-to-perform platelet function assay, which can supplement existing well-known platelet function tests and can potentially be useful for screening cardiac patients with abnormal platelet functions.
Footnotes
Acknowledgments
This study was supported by a grant from the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (H15C1512) and a grant of the Establish R&D Platform Project through the 365 Korea University Medical Center and Korea University Guro Hospital (grant number: O1903851).
Conflicts of interest
No potential conflicts of interest relevant to this article were reported.