
Abstract
Background:
N-terminal pro-B-type natriuretic peptide (NTproBNP) appears to be a useful tool for diagnosing hemodynamically significant patent ductus arteriosus (hsPDA) in preterm infants. However, a consensus for its application has not been reached.
Objective:
The present study aims to evaluate the role of NTproBNP in predicting hsPDA in preterm infants, and explore the optimal cutoff value and testing-time.
Methods:
A prospective blind study of 120 preterm infants with birth weights of < 1,500 g was conducted at the NICU of Peking University Shenzhen Hospital. Blood samples were successively collected on the first three days after birth for NTproBNP analysis. Echocardiographies were performed on day three of life to confirm the status of the ductus arteriosus. A receiver operating characteristic curve (ROC) analysis was performed to determine the ability of NTproBNP to recognize hsPDA.
Results:
NTproBNP was significantly higher in infants with hsPDA, than in infants in the control group, on both day two (P < 0.001) and day three (P < 0.001). On day two, a NTproBNP cutoff value of 3,689.0 pmol/L offered an optimal predictive value for hsPDA, while on day three, the optimal cut-off value for hsPDA was 2,331.5 pmol/L. The investigators proposes day three of life (48–72 hours) as the optimal testing time.
Conclusion:
The NTproBNP biomarker during the early neonatal period can be a useful tool for screening and assessing hsPDA in premature infants, especially on day three of life.
Introduction
Patent ductus arteriosus (PDA) on the 4th day of life would persist in approximately 10% of infants with gestational age (GA) between 30 and 37 weeks, in 80% of infants with GA between 25 and 28 weeks, and in 90% of preterms born at 24 weeks of GA [1]. However, among infants with birth weights of < 1,500 g (very low birth weight infants, VLBWIs), 85% needs treatment [2]. The prolonged condition of PDA in preterms can be associated with important complications, such as severe respiratory distress syndrome (RDS), prolonged need for assisted ventilation, pulmonary hemorrhage, bronchopulmonary dysplasia (BPD) [3], necrotizing enterocolitis (NEC), renal function damage, intraventricular hemorrhage (IVH), periventricular leukomalacia (PVL), cerebral palsy (CP), or death [4]. Meanwhile, in terms of the possibility of spontaneous closure of the ductus and side effects of treatments, and regardless of whether drugs were given or surgery was performed, the most reasonable strategy at present appears to be reserving treatment only for hemodynamically significant PDA (hsPDA) [5]. Although some studies suggested that the causative relationship between PDA and complications of prematurity [7], many infants with hsPDA have serious hemodynamical complications, so these infants must be diagnosed. Echocardiography remains as the diagnostic gold standard, but requires expensive equipment and the assistance of a trained operator, which is not available all the time in all neonatal units.
Brain natriuretic peptide (BNP) and amino-terminal pro-B-type natriuretic peptide (NTproBNP) are synthesized and released into the circulation by cardiac ventricular myocytes in response to pressure overload, volume expansion and increased myocardial wall stress. Within these myocytes, the precursor proBNP (108 amino acids) is converted to the biologically active form, BNP (77–108 amino acids), and the inactive NTproBNP fragment (1–76 amino acids), while NTproBNP has a longer half-life (60-120 minutes vs. 22 minutes), is more stable in vitro [8], and may serve as a better marker than BNP for assessing ventricular dysfunction and volume overload [9]. It is known that in hsPDA, significant shunting of blood occurs from the systemic to the pulmonary circuit, resulting in changes in pressure overload and myocardial wall stress. Therefore, subsequent studies have been conducted to prove that NTproBNP can be a useful biomarker for diagnosing hsPDA in premature neonates.
Recently, a systematic review [10], which included 11 NTproBNP studies, concluded that the sensitivity and specificity of NTproBNP for diagnosis of hsPDA was 90% (95% CI: 0.79–0.96) and 84% (95% CI: 0.77–0.90), respectively. However, these studies varied by methodological quality, type of commercial assay, thresholds, age at testing, gestational age, and whether an assay was used. Thus, there is presently no consensus on its optimal values and proper testing-time. The present prospective and blinded study was undertaken to establish a range of plasma NTproBNP concentrations found in VLBWIs suffering from PDA, and determine how and when to use these as a screening tool for predicting hsPDA.
Methods
Subjects
The study was performed in the neonatal intensive care unit (NICU) of Peking University Shenzhen Hospital from January 2015 to December 2017. The enrollment criteria were as follows: (1) preterm infants with a birth weight of < 1,500 g; (2) preterm infants admitted within six hours after birth. The exclusion criteria were as follows: (1) major congenital heart anomalies, other than PDA, and foramen ovale or atrial septal defects; (2) life-threatening congenital malformation; (3) renal dysfunction with serum creatinine concentration > 1.5 mg/dL (132μmol/l).); (3) serious persistent pulmonary hypertension with vasodilator dependence (such as nitic oxide inspiration, magnesium sulfate, or prostaglandin intravenous injection); (4) death within three days after birth.
Ethics
The present study was approved by the Peking university Shenzhen Hospital ethics committee, and a consent was obtained from the parents before enrolling the infants into the study.A written informed consent was obtained from legal guardians of all participants.
Study design
Sampling of plasma NTproBNP
Blood (0.5 mL in tubes containing lithium heparin) was collected by venous blood sampling, along with other routine blood sampling, in order to avoid extra needle sticks and excessive blood sampling at 6–24 hours (day one), 24–48 hours (day two), and 48–72 hours (day three) after birth. Then, these were immediately analyzed. Plasma NTproBNP was measured by electrochemiluminescence immunoassay using a Roche Elecsys 2010 analyzer (Roche Diagnostics, Burgess Hill, UK). The analytical range was 0.6–4,130 pmol/L (5–35,000 pg/ml, 1 pmol/L = 8.457 pg/ml). All NTproBNP results were withheld by the laboratory until the recruitment was closed on December 2017, in order to ensure that the clinical investigators were blinded to the NTproBNP results.
Echocardiography
All infants enrolled in the present study were evaluated by echocardiography on day three by two experienced investigators who were blinded to the NTproBNP concentration. Echocardiographies were performed using a 5–10 MHz probe (Phillips IE33; Phillips Medical Systems, NA, Bothell, WA, USA). A two-dimensional color Doppler, pulse-wave Doppler and M-mode echocardiogram was simultaneously performed [11]. If PDA was diagnosed, the point of maximal constriction of the color flow jet was measured in millimeters by frame analysis, in order to assess the ductus arteriosus (DA) size. The left atrium (LA) and aortic root (AO) dimension were measured in the parasternal short axis view at the level of the aortic valve, and the LA/AO ratio was calculated.
HsPDA was defined as a DA size of≥1.5 mm, with at least two additional clinical features, including heart murmur, persistent tachycardia (heart rate > 160/min), hyperactive precordium, bounding pulse, pulse pressure > 25 mmHg, and chest radiographic evidence of cardiomegaly or pulmonary congestion [12, 13]. Otherwise, asymptomatic patent ductus arteriosus asPDA was defined as PDA that did not meet the above criteria.
Statistical analysis
The analysis was performed using SPSS version 19.0 (SPSS Inc, Chicago, IL, USA). Categorical data were presented in numbers (%), and compared using Chi-square test or Fisher’s exact test. Continuous data were presented in median (range) or mean (SD), and compared using Student’s t-test (for unmatched groups) and paired Student’s t-test (for paired data), in order to compare continuous variables. The logistic regression model was used to evaluate the association between multiple factors (the factors in Table 1) and hsPDA. Pearson’s correlation coefficient was used to test for correlations between NTproBNP and echocardiographic variables. The receiver operator characteristic (ROC) curve was created to select the best cut-off point (threshold value) of NTproBNP for detecting hsPDA. Repeated-measured ANOVA analysis was performed for data with continuous changes. A P-value<0.05 was considered statistically significant.
Demographic and clinical characteristics of the study cohort
Demographic and clinical characteristics of the study cohort
Values are expressed as mean (±SD) or *Median (range); GA: Gestational Age; BW: Birth Weight; Infection refers to Chorioamnionitis or/and EOS;NRDS: Neonatal Respiratory Distress Syndrome; PS: Pulmonary Surfactant, PIH: Pregnancy Induced Hypertension. MV: Mechanical Ventilation.
Baseline characteristics
A total of 155 preterm infants were recruited in the present study. Among these infants, 120 infants (48 male and 72 female infants, mean gestational age was 30.6±1.5 weeks, and mean birth weight was 1.26±0.2 kg) were eligible for evaluation. Among these 120 infants, 83 infants (71.7%, 83/120) were detected with PDA (including 43 infants with hsPDA and 40 infants with asPDA), while 37 infants (28.3%, 37/120) had no PDA. Furthermore, among these 120 infants, 43 infants were assigned to the hsPDA group (43/120, 35.8%), while 77 infants were assigned to the non-hsPDA group (77/120, 64.2%). The complete data collected and information are presented in Figure 1. The demographic and clinical characteristics between the hsPDA group and control group are presented in Table 1. Infants in the hsPDA group were relatively more seriously ill with smaller gestational age (29.9±1.7 weeks vs. 31.0±1.2 weeks, P = 0.000), had lower Apgar scores (one minute: 7 [6, 8] vs. 8 [6.5, 8.0], P = 0.006; five minutes: 9 [8, 9] vs. 9 [8, 10], P = 0.013), and had more incidences of neonatal respiratory distress syndrome (NRDS; 76.7% vs. 51.9%, P = 0.011) and applications of pulmonary surfactant (PS; 67.4 vs. 45.5%, P = 0.023). However, the multivariate regression analysis revealed that these factors were independent predictors of hsPDA (P < 0.05).
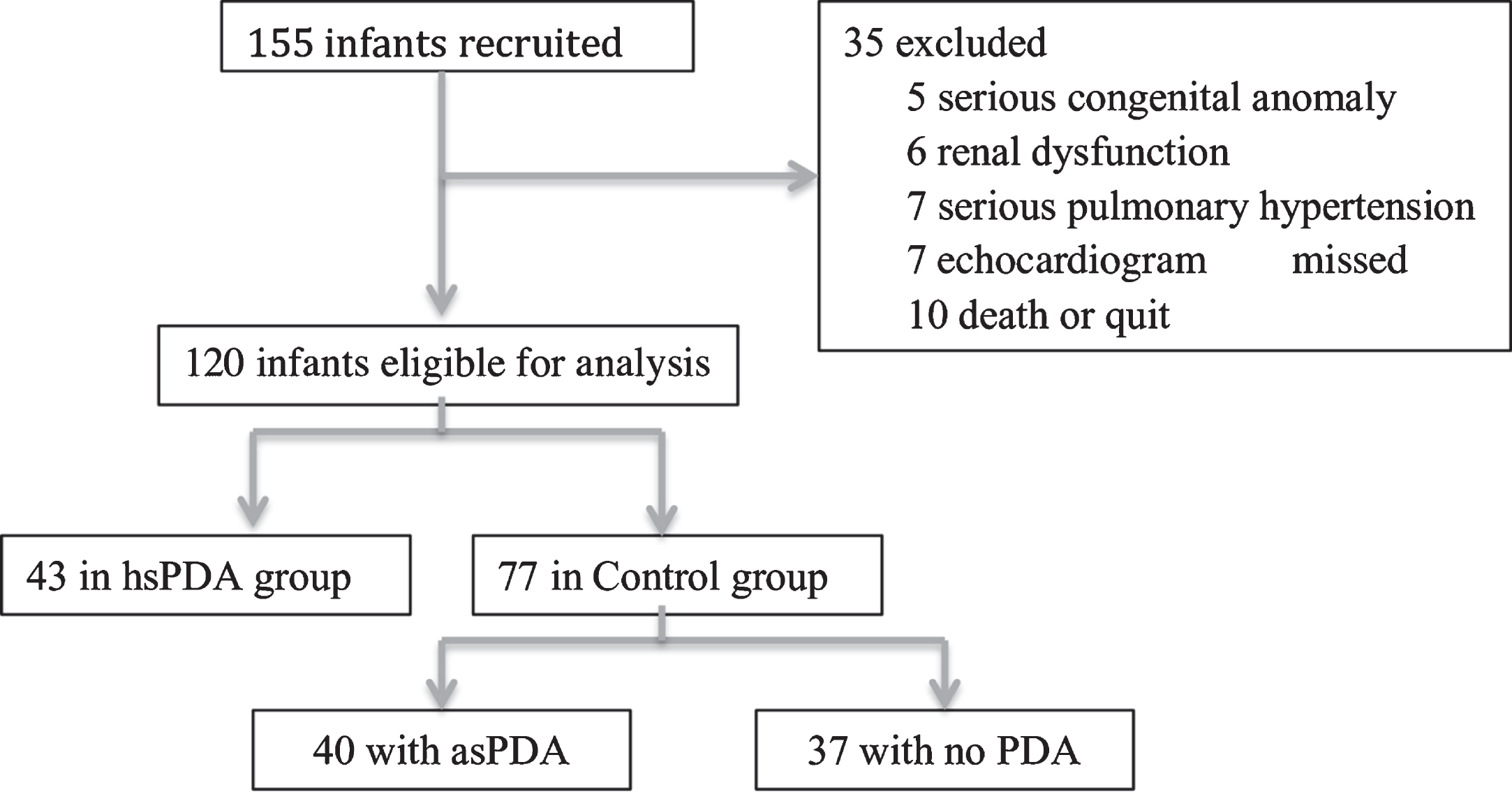
Study population based on 155 preterm infants consecutively admitted to Peking University ShenZhen Hospital from Jan 2015 to Dec 2017.
The plasma levels of NTproBNP were found to be significantly higher in the hsPDA group in the first three days after birth (P < 0.001, Table 2). In the subgroup analysis of 43 infants with hsPDA and 40 infants with asPDA, no significant difference was found on day one (P > 0.05). However, on day two and three, the NTproBNP value of infants in the hsPDA group was significantly higher, when compared to that of infants in the asPDA group (P < 0.001, Table 3).
Comparison of NTproBNP values in hsPDA group and non-hsPDA group(pmol/L)(mean±SD)
Comparison of NTproBNP values in hsPDA group and non-hsPDA group(pmol/L)(mean±SD)
Comparison of NT-proBNP values in hsPDA group and asPDA group(pmol/L) (mean±SD)
Figure 2 illustrates the successive change in NTproBNP level in the first three days after birth. This indicated a peak in day two of life, which was about to decline from day three. The repeated-measures ANOVA analysis revealed significant differences among these changes in three days (ɛ= 0.649, p < 0.001). The plasma NTproBNP concentration in the hsPDA group rapidly increased from 2050.0±590.0 pmol/L to 5,716.8±2267.0 pmol/L on day two (paired t-test, t = 10.009, P < 0.001), and this remained at a high level of 5,505.10±2,210.20 pmol/L on day three, but remained lower than that on day two (paired t-test, t = 2.154, P < 0.05). However, for infants without hsPDA, the plasma NTproBNP concentration between day one and two had no significant difference (paired t-test, t = 0.956, P > 0.05), but this significantly decreased on day three (paired t-test, t = –6.686, P < 0.05). NTproBNP in the non-hsPDA group remained at a relatively lower level from days one to three, with a significant narrower range, when compared to the hsPDA group (day three to day one, t = 11.358, P < 0.001). The logistic regressive analysis revealed that NTproBNP was an independent predictor of hsPDA, both on day one and day two (day one: OR = 1.001 [0.999, 1.003], P > 0.05; day two: OR = 1.001 [0.999, 1.002], P > 0.05). NTproBNP on day three was a risk factor of hsPDA (OR = 1.003 [1.001, 1.005], P < 0.05).
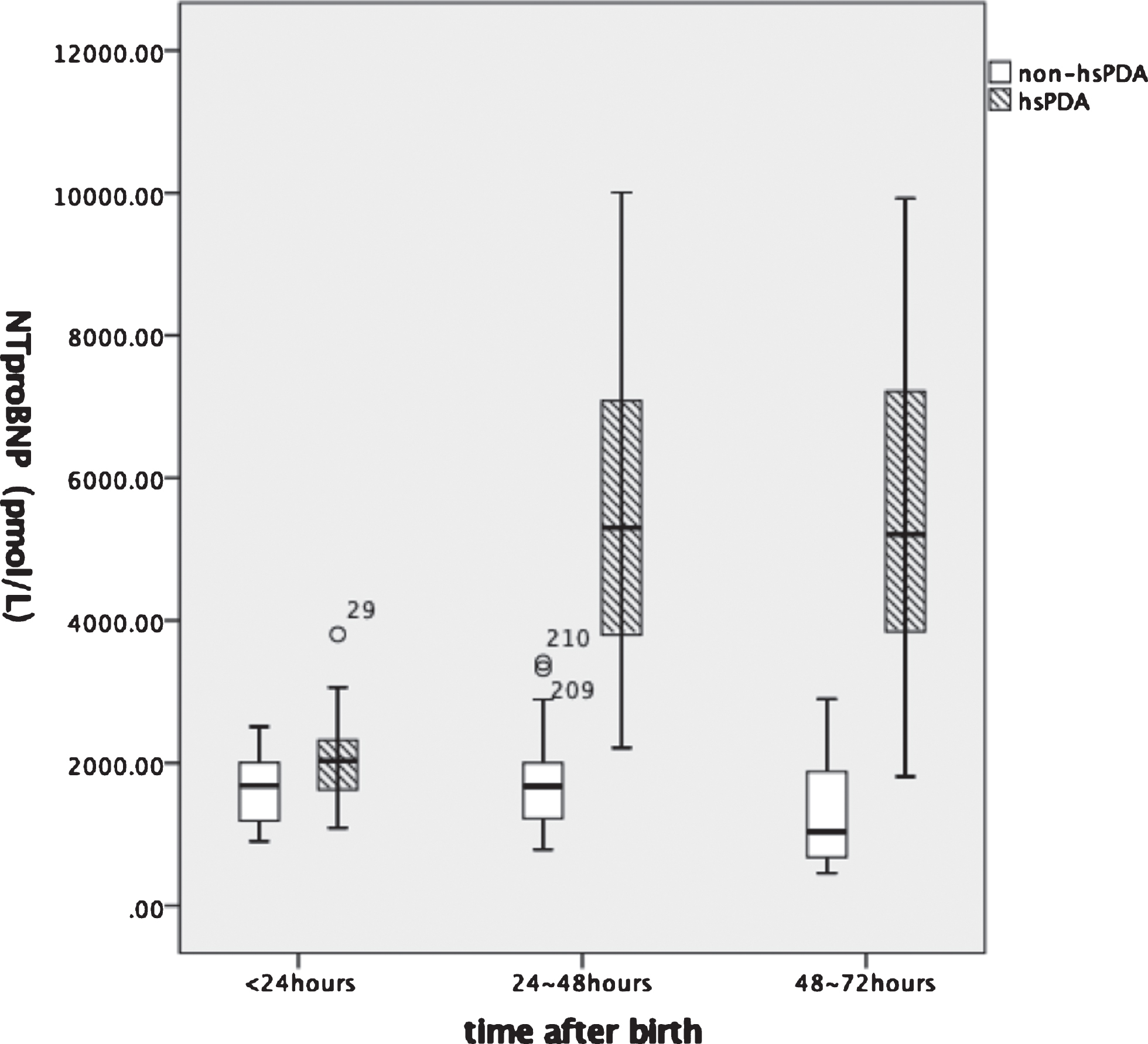
The variation trend in the first 3 days after birth in hsPDA group and control group.
Using the ROC curve (Figure 4), a cutoff NT–proBNP value on day two of 3,689.0 pmol/L offered an optimal predictive value for HsPDA, with a sensitivity and specificity of 83.7% and 93.5%, respectively (area under the curve [AUC]: 0.943; 95% confidence interval [95% CI]: 0.903–0.984; P < 0.001). However, on day three, the optimal cutoff value for hsPDA was 2,331.5 pmol/L (sensitivity: 97.7%; specificity: 89.6%; AUC: 0.987; 95% CI: 0.973–1.000; P < 0.001).
Infants in the hsPDA group were detected with a higher DA size and LA/AO ratio, when compared to the asPDA group (DA: 2.03±0.5 mm vs. 1.23±0.2 mm, t = 8.941, P < 0.001; LA/AO ratio: 1.32±0.1 vs. 1.12±0.1, t = 10.071, P < 0.001). When coupled with these values among all 83 infants detected with PDA, NTproBNP values were found to have a significant correlation with DA, both on day two (r = 0.890 [0.840, 0.929], P < 0.001) and day three (r = 0.889 [0.836–0.929], P < 0.001). Furthermore, NTproBNP values had a significant correlation with the LA/AO ratio (day two: r = 0.617 [0.482–0.725], P < 0.05); day three: r = 0.642 [0.510–0.753], P < 0.05), as presented in Figure 3. However, when only infants with hsPDA were taken into consideration, it was found that there was a positive correlation with DA (day two: r = 0.767 [0.615–0.858], P < 0.001; day three: r = 0.789 [0.667–0.871, P < 0.001]), but there was no significant correlation with the LA/AO ratio (day two: r = 0.2 [–0.109–0.524], P > 0.05); day three: r = 0.149 [–0.192–0.452], P > 0.05).
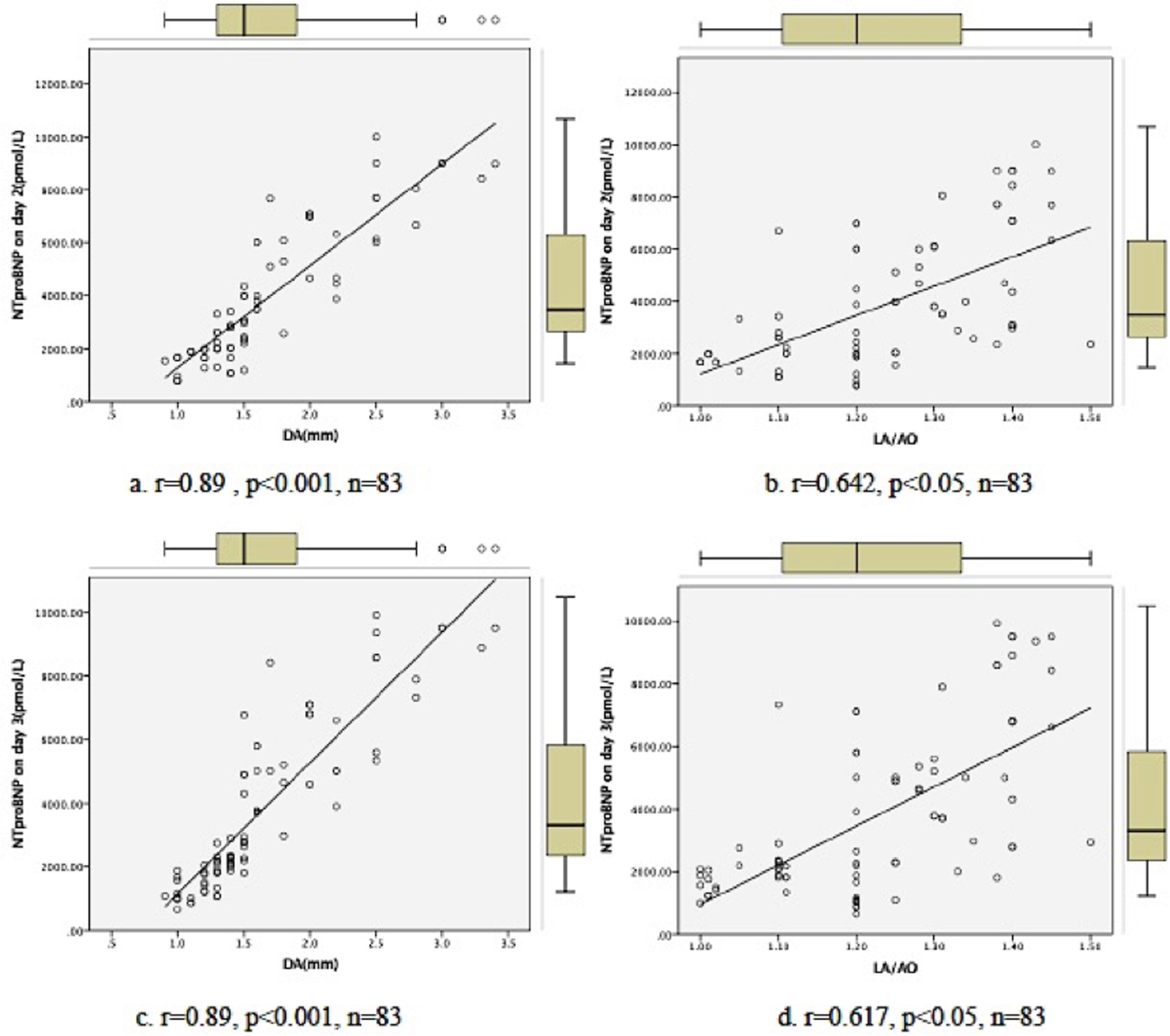
Correlation of plasma NTproBNP levels at day 2 (a-b) and day 3 (c-d) of life. Data are presented as scatter plots. Spearman’s rank order correlation coefficients (r) and level of significance (P) are given.
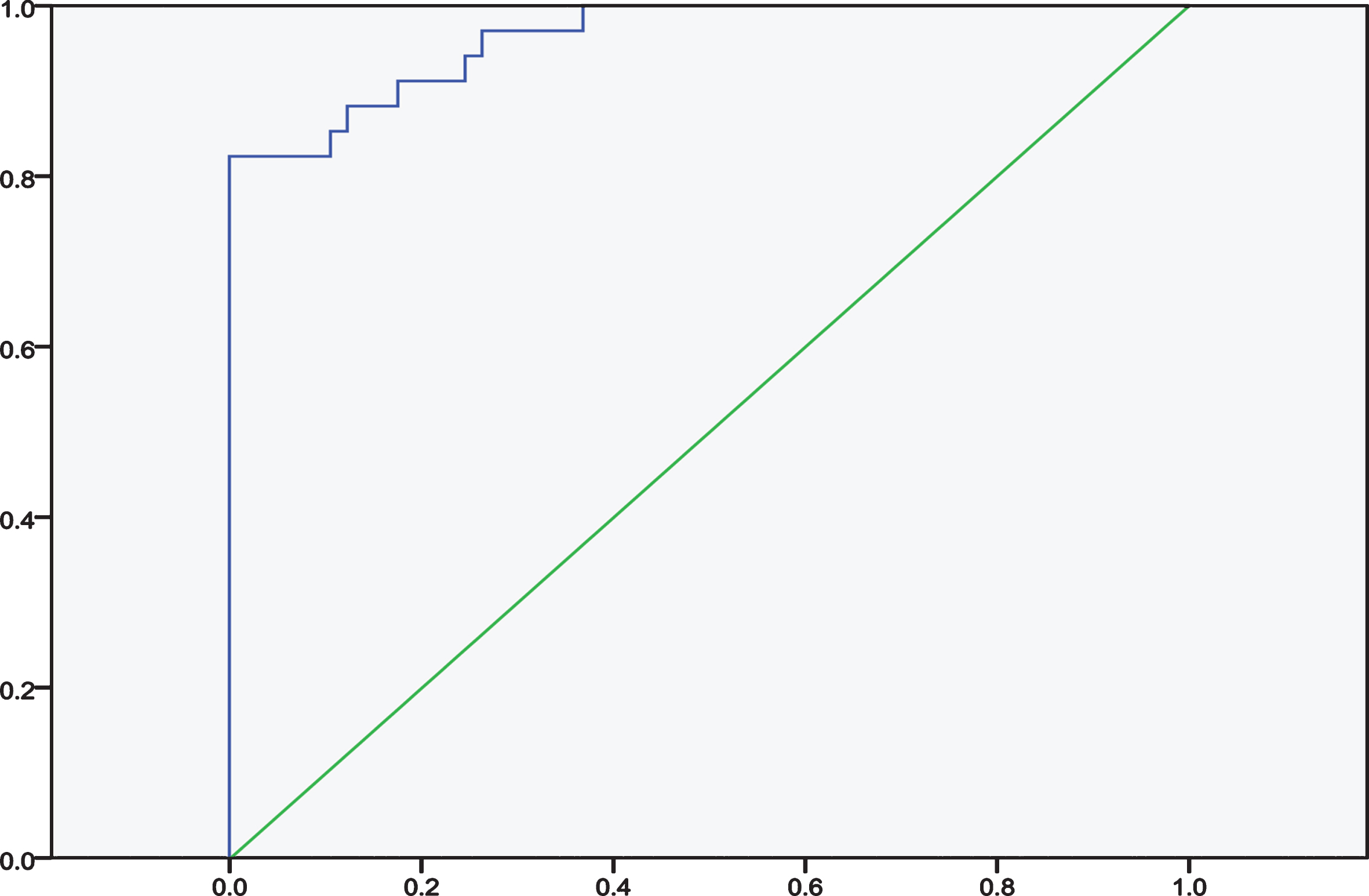
ROC. Using the receiver operating characteristic curve (ROC), NT-proBNP level was a good predictor of an HsPDA with the area under the curve of 0.962 (95% IC: 0.928 0.997, P = 0.000). Using a cut-off value of 1742 pmol/L was associated with a 100% sensitivity and 63.2% specificity of accurately diagnosing an HsPDA. Meanwhile, the optimal cut-off value was 2779 pmol/L associated with a 91.2% sensitivity and 82.5% specificity.
In the present prospective study, results suggested that for infants with hsPDA, there was significant shunting of blood from the systemic circuit to the pulmonary circuit, resulting in increased pulmonary blood flow and the subsequent increased pressure overload and myocardial wall stress, as well as cardiac pressure (reflected by high pulmonary pressure). The changes in pressure were mainly decided by the volume of the shunt. Hence, there was a significant difference in NTproBNP value between the hsPDA group and asPDA group, indicating that NTproBNP level had a patent role in diagnosing hsPDA in infant with PDA.
As revealed in the successive monitoring of plasma NTproBNP concentration, the values in infants without hsPDA remained at a relatively stable and lower level in the first three days of life, which was similar to a plateau. For infants with hsPDA, these values rapidly and significantly increased within 24–48 hours of life, and remained high on within 48–72 hours of life. The peak levels presented on day two (24–48 hours of life), which is in accordance with the studies conducted by Alenazi [14] and Ramakrishnan [15], in which NTproBNP remained at a high level even on day seven. In general, in healthy preterm infants without hsPDA, the levels of NTpBNP would surge at birth, maintain a plateau on days 3–4, and rapidly decline within a week. Then, this would be followed by a steady fall to a stable level, reaching a constant level in infancy [14–16]. Since the preterm infants appears to have unstable hemodynamic changes in the first few days after birth, and it was assumed that these various influences would induce the DA to open or reopen, such as resuscitation, PS therapy and fluid therapy, with not a sole, but a comprehensive influence. Proper management would probably induce the DA to close or partly close by day three.
To date, studies of NTproBNP for the early prediction of hsPDA continue to have varying cutoff values and testing times (day two or three) [9, 14–18]. In order to discriminate whether the NTproBNP level on day two or three would be better, both values of these two days were taken into consideration. As a result, the NTproBNP level in the hsPDA group was significant higher than that in the control group, both on day two and day three. Preterm infants with NTproBNP levels exceeding 3,689.0 pmol/L on day two of life, and levels exceeding 2,331.5 pmol/L on day three of life were very likely to be diagnosed with hsPDA. Some recent studies were summarized with the present study in Table 4. All of these had the same assay (Roche Elecsys system) and a relatively similar GA. Furthermore, the thresholds widely varied from 1,203 pmol/L [16] to 7,252 pmol/L [14] on day two of life. The possible reasons would be that the conditions of these infants were more unstable and in need of various clinical management within the first 48 hours after birth, leading to more influences on circulation. However, on day three (48–72 hours), these findings appeared to be similar to that observed in the present study, to a certain extent. The scatter plot revealed a relatively concentrate trend, ranging from 1345.3 pmol/L [9] to 3196.8 pmol/L [18]. These variations may be due to the different populations (including races, GA, and BW) studied, the severity of illness, and the definition of hsPDA across these studies.
Cut-off values of plasma NTproBNP concentration in diagnosis of hsPDA in preterm infants in different studys
Cut-off values of plasma NTproBNP concentration in diagnosis of hsPDA in preterm infants in different studys
*The diamond stand for cutoff value of this study; the square stand for cutoff value of other studies; the vertical line stand for the mean value of these studys.
Moreover, the logistic regressive analysis revealed that NTproBNP level was an independent predictor for hsPDA, both on day one and day two. The NTproBNP level on day three was a dependent risk factor of hsPDA. Hence, it appears that day three of life (48–72 hours) would be the optimal testing time.
Traditional echocardiographic parameters, such as DA size and the LA:AO ratio, were used as the gold standard for determining hsPDA [14, 19]. In the present study, the same results were demonstrated, in which NTproBNP significantly correlated with the echo parameters of the DA size and LA/AO ratio, both on day two and day three of life (P < 0.05). However, when only infants with hsPDA were taken into consideration, no significant correlation between NTproBNP and the LA/AO ratio was found (P > 0.05). This was consistent with the study conducted by Harling S et al., which revealed that ductal diameter was the most accurate echocardiographic marker for predicting a significant shunt. In the preterms observed in studies conducted by Martinovicie et al. [21] and Buddhe et al. [22], there was a relatively stronger correlation between plasma NTproBNP level and DA size, when compared to the LA/AO ratio. Furthermore, the study conducted by König K et al. [23] also revealed that NTproBNP was only significantly correlated with PDA size in very preterm infants.
To date, the present prospective study and other studies have shown that early plasma NTproBNP levels in preterm infants can be used to predict the presence of hsPDA, and correlated this with the degree of ductal shunting through significant positive correlations with the DA size and LA/OA ratio. Plasma NTproBNP, which lacks the influence of antenatal and postnatal factors on these levels (gender, chorioamnionitis, steroids, delivery, and inotrope use) [9], has been proven to be a useful tool for predicting hsPDA and guiding the target treatment in the early stage [24, 25]. Concerning the more variable levels in the first 48 hours after birth, and acting as a dependent risk factor of hsPDA on day three (48–72 hours), it is recommended that the proper time to screen for hsPDA is 48–72 hours after birth.
The limitations of the present study were as follows. The study had a small sample size. In addition, there were few confounding factors that could influence the validity of the NTproBNP levels, such as increased pulmonary vascular resistance, concomitant renal impairment, hydration status and sepsis. And while BNP is positively associated with left to right shunt, currently there is no clear evidence that BNP can be used to determine treatment decisions. We also did not specifically statedthe treatment decisions regarding active ductal closure interventions, as we did not directly address whether there is a high predictive value of this test to identify infants who would benefit from intervention. In addition, Kulkarni MAA indicated that that BNP or NT-proBNP assays should be locally validated for specific patient population and outcomes, so we still need to validate the cutoff value detected in our local population, since the data may not reach the same value in other centers, so that our findings can be used as a reference for other medical centers.
The biomarker of plasma NTproBNP levels during the early neonatal period is significantly correlated to the PDA shunt magnitude. This can be applied as a useful tool to screen and assess hsPDA in premature infants, which is cost effective, easily available, and can supplement the information obtained from functional echocardiography, aiding in the management of hsPDA. NTproBNP levels of > 3,689.0 pmol/L on postnatal day two or > 2,331.5 pmol/L on postnatal day three indicate the high possibility of hsPDA in VLBWIs, with high sensitivity and specificity. However, the investigators proposes day three of life (48–72 hours) as the optimal testing time.