
Abstract
PURPOSE:
To evaluate the diagnostic value of shear wave velocity (SWV) ratio for the differential diagnosis of benign and malignant breast lesions.
MATERIAL AND METHODS:
Our retrospective study included 151 breast lesions that were diagnosed by biopsy and surgical pathology. All of the breast lesions were detected by conventional ultrasound and Virtual Touch tissue quantification (VTQ) and mammography. The sonographic characteristics of the breast lesion, such as the internal echo, shape, margin, color flow, and calcification so on, were also observed. The SWV in lesions and surrounding parenchyma were measured and the SWV ratio between the lesion and surrounding parenchyma was calculated. Pathological results were used as a diagnosis standard to compare the value of SWV ratio, VTQ, and mammography in the diagnosis of benign and malignant breast lesions.
RESULTS:
The 151 breast lesions included 96 benign lesions and 55 malignant lesions. The cutoff value of VTQ in the diagnosis of benign and malignant breast lesions was 5.01 m/s, of SWV ratio was 2.43, and mammography was BI-RADS 4B. The sensitivity, specificity, accuracy and the area under the ROC curve (AUC) of the SWV ratio were 78.2%, 86.5%, 83.4%, and 0.83 respectively. While of SWV ratio with mammography was 86.4%, 89.4%, 88.3% and 0.87, respectively. The sensitivity, specificity, accuracy, and AUC of SWV ratio and SWV ratio with mammography were statistically higher than those of mammography, no statistically higher than VTQ and VTQ with mammography.
CONCLUSION:
The SWV ratio can improve the sensitivity without sacrificing diagnostic specificity in the process of breast cancer diagnostic, provide a better diagnostic performance, and avoid unnecessary biopsy or surgery.
Introduction
The incidence of breast cancer has continued to rise in China recently [1], moreover, patients with advanced-stage breast cancer have a poor prognosis [2], the 10-year survival rate of T3 breast cancer masses is less than 60%, while approximately 85% in patients with T1 breast cancer lesions (≤20 mm) [3]. Early detection and accurate diagnosis are crucial to improving the survival rates and quality of life of patients with breast cancer. Mammography is an important tool for the diagnosis of benign and malignant breast lesions, especially for breast lesions with micro-calcification, which may lead to a missed diagnosis for the breast ultrasound examinations. However, Chinese women tend to have dense breast tissue that X-rays cannot easily penetrate, and the masses may not be detectable by mammography [4, 5]. It has reported that the sensitivity and specificity of mammography is commonly reported to varies between 69 and 90% [6, 7]. Ultrasound (US) is thought to be the most important adjunct to mammography in the differential diagnosis of breast masses [8–10], and it has a specificity of 92.7–95.0% and a sensitivity of 68.0–91.2% in previous research [11]. Although the US is a useful tool in differentiating benign from malignant breast tumors, it can only provide morphologic information, such as size, shape, echo intensity, margin, boundary, calcification and blood flow, but not the functional information of the breast tumor, and may lead to a considerable number of false-positives [11].
Generally, the tissue stiffness of malignant breast tumors is higher than that of the benign tumors; thus, the information on stiffness can be used to differentiate benign from malignant breast tumors [12–14]. Ultrasound elastography which could provide additional functional information by reflecting tissue stiffness [15], has been used to assess abnormalities between benign and malignant lesions. Acoustic radiation force impulse (ARFI) imaging is a type of US elastography to measure tissue stiffness without external compression. It has two modes: Virtual Touch tissue imaging (VTI), Virtual Touch tissue quantification (VTQ) and Virtual touch tissue imaging quantification (VTIQ) [16]. The stiffer the tissue is, the darker the ROI becomes in VTI, and the greater shear velocity it will show in VTQ [16]. VTI qualitativly evaluated the tissue stiffness through by the acoustic impulses emitted by the probe, with the advantages of more reproducible and operator independent. While VTQ was quantitatively reflected the elasticity of tissue stiffness with several limitations: such as the fixed region of interest (ROI) (i.e., 6 mm×5 mm) and the limited SWS measurement range (i.e., 0.5–9.0 m/s) [17].
The aim of our study was to evaluate the diagnostic value of shear wave velocity (SWV) ratio for the differential diagnosis of benign and malignant breast lesions.
Materials and methods
Patients
This retrospective study was approved by our hospital’s Institutional Review Board (Approval No:2019-027), and the informed consent of participants was waiving. From July 2014 to July 2018, women with suspicious conventional US or mammography findings of breast masses were scheduled to undertake the US-guided biopsy, which was enrolled in the study. And before the biopsy, the diagnostic ultrasound examinations of the breast were undergone, including ARFI imaging with VTQ. The following inclusion criteria needed to be met: (1) the patient was older than 35 years, (2) the cystic areas of the breast tumor were less than 25%, to reduce the impact of ROI fixation (6*5 mm) on the accuracy of shear wave measurement in cystic solid nodules less than 10 mm, (3) the minimum diameter of the mass was larger than 6 mm, since the region of interest (ROI) is fixed (i.e., 6 mm×5 mm) [17], (4) the patient had never received any treatment for the tumor, (5) all patients need to obtain the results of ultrasound and molybdenum target examination and (6) pathological confirmation of the lesion was obtained by surgical or needle biopsy. For patients with multiple breast lesions, only the most suspicious breast lesions found by the conventional US or mammography were included. Details about this study program are listed in Fig. 1. Finally, a total of 151 consecutive women with 151 the most suspicious breast lesions were included in our study based on the criteria. The final diagnosis for all breast lesions was derived from the pathological results after core biopsy or surgery, and the interval time between ultrasound and core biopsy or surgery can not more than 3 months.

Details about this study program.
The Ultrasound(US) and ARFI imaging were performed by using the Siemens S2000US machine (Siemens Medical Solutions, Mountain View, CA, USA) equipped with the linear array transducer (9L4, Siemens), and the center frequency of it was 7.5 MHz (range, 4.0–9.0 MHz). All of the US examinations were independently carried out by two radiologists who had more than 5 years of experience in breast US examination and who had performed optimal ARFI imaging. The sonographic characteristics of the breast lesion, such as the internal echo, size, shape, margin, color flow, posterior acoustic effect, and calcification, were also recorded. ROI of VTQ was localized to the lesion and sufficient surrounding parenchyma avoiding the calcified or cystic areas as much as possible. Five valid SWV values were measured for each lesion, and the median value of these was recorded as a mean SWV. Mean SWV values obtained from each lesion and surrounding parenchyma, as well as the SWV ratio of lesion-to-surrounding parenchyma for each lesion, were recorded. For the lesions with heterogeneous components, the SWV value was outside the acceptable range of the VTQ system (0.5–9.0 m/s) and was displayed as “X.XX”; we recorded it as 0 m/s when the ROI was placed in the cystic portion while recorded it as 9.0 m/s in the solid portion. When the SWV value was given as “NA” by the software, “NA” was recorded as 10 m/s. All data were recorded and stored for further analysis.
Mammography
On mammography, mediolateral oblique (MLO) view and Craniocaudal (CC) view were conducted for all patients, performed using the molybdenum-rhodium target full-field digital MG (FFDM) system (Senographe DS, GE Medical Systems, Buc, France), following the imaging parameters: 40 kHz, 18–35 kV, and 1–100 mAs. A mediolateral view or spot view was performed if necessary. Observed and recorded the gland type, breast skin, nipple, lesion location, size, density, border, morphology, presence or absence of calcification, calcification type, and axillary lymph nodes, etc., by the same radiologist physician who is skilled in mammography. And classify the lesions according to the Breast Imaging Reporting and Data System (BI-RADS) guidelines issued by the American College of Radiology in 2003. We set BI-RADS-X≥4B as the diagnostic cutoff point in the differential diagnosis of breast lesions [18].
When mammography, US or VTQ was combined SWV ratio, the lesion was considered malignant as long as it met one of the above examination results is suspected to be malignant.
Statistical analysis
Statistical calculations were performed using SPSS 21.0 (IBM Corp, Armonk, NY, USA). The SWV values were expressed as the mean±standard deviation (SD). Continuous variables were compared between the mean velocity values of the benign and malignant groups by using the independent two-samples t-test. The diagnostic performance of mammography and the combination of the SWV ratio with mammography were evaluated using the receiver operating characteristic (ROC) curve analysis. The difference between the AUC of the three methods was compared by the Z test. The differences were considered statistically significant if the p-value was <0.05.
Results
151 female patients with151 breast lesions were included and all breast lesions confirmed by biopsy or surgical pathology. Of the 151 lesions, 96 (63.6%) were benign, and 55 (36.4%) were malignant. And most of the breast lesions were located in the outer upper quadrant of bilateral breasts. The maximum diameters of the lesions ranged from 6 mm to 40 mm; the mean±SD of benign breast lesions was 16.8±7.01 mm, while 19.7±9.91 mm in malignant breast lesions, there were no statistically significant differences between the malignant and benign lesions in age (t = 1.89, P = 0.061). The age of the patients with malignant breast lesions was 35–79 (49.75±9.62) years old, while those with benign breast lesions were 35–72 (45.81±8.15) years old, there were statistically significant differences between the malignant and benign lesions in age (t = 2.5, P = 0.014) Table 1.
Characteristic of patients or breast lesions
Characteristic of patients or breast lesions
On mammography, BI-RADS-X≥4B was considered as the diagnostic cutoff point in the differential diagnosis of breast lesions in our study. There were 143 breast lesions with BI-RADS-X < 4B (benign) and 63 with BI-RADS≥4B (malignant). The cutoff value of BI-RADS-X≥4B yielded a sensitivity of 54.5%, a specificity of 83.3% and an accuracy of 72.8%. The area under the ROC curve (AUC) of it was 0.69.
On US, BI-RADS-US ≥ 4A was considered as the diagnostic cutoff point in the differential diagnosis of breast lesions in our study, it yielded a sensitivity of 74.5%, a specificity of 76.0% and an accuracy of 75.5%. The area under the ROC curve (AUC) of it was 0.75.
The SWV of malignant lesions ranged from 2.45 to 9.0 m/s, and the mean±SD was 7.38±1.79 m/s, while benign lesions ranged from 1.09 to 7.35 m/s, and the mean±SD was 3.85±2.15 m/s. The cutoff value of VTQ in the lesion of 5.01m/s yielded a sensitivity of 76.4%, a specificity of 85.4% an accuracy of 82.1% and AUC of 0.81. And it has a sensitivity of 76.5%, a specificity of 75.0% and an accuracy of 75.6% in the largest diameter <10 mm (41 lesions), 88.8%, 81.5%, 84.4%, respectively in 10–20 mm (45 lesions), while 95.8%, 87.5%, 92.7%, respectively in the largest diameter >20 mm (55 lesions).
The SWV of the surrounding parenchyma in malignant lesions ranged from 0.81 to 8.9 m/s, and the mean±SD was 2.58±1.49 m/s, while in the benign lesions, the range was from 0.88 to 8.9 m/s, and the mean±SD was 2.66±1.82 m/s. The SWV ratio of the lesion-to-surrounding parenchyma of malignant lesions ranged from 1.66 to 8.69, and the mean±SD was 4.89±1.93, while in the benign lesions the ratio ranged from 0.28 to 5.7, and the mean±SD was 1.82±0.63, there were statistically significant differences between the malignant and benign lesions in SWV and SWV ratio (P < 0.05). The cutoff value of the SWV ratio of 2.43 yielded a sensitivity of 78.2%, a specificity of 86.5%, an accuracy of 83.4% and AUC of 0.83 Fig. 2.
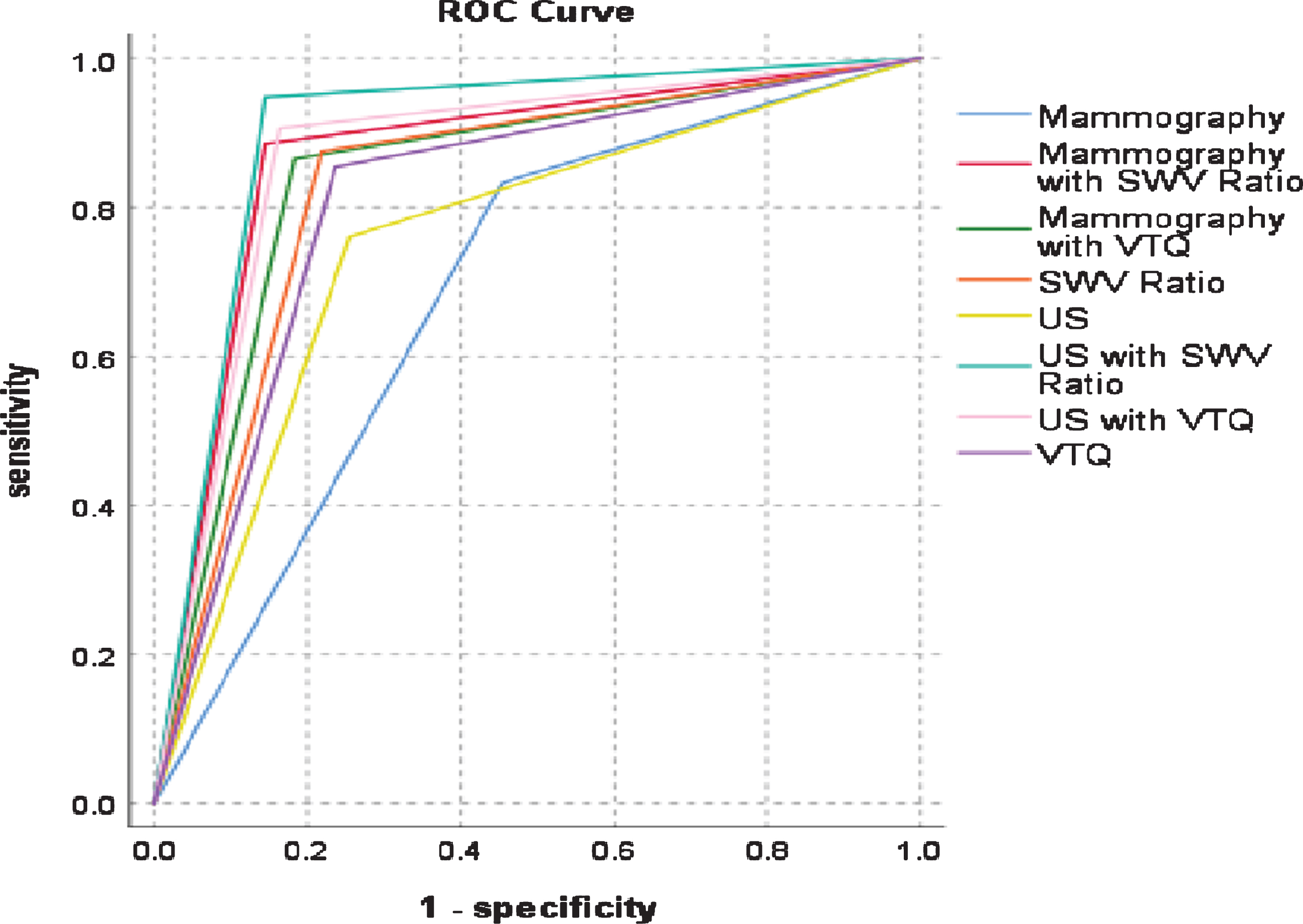
ROC of Mammography, US, VTQ, SWV Ratio and their Combined used.
The sensitivity, specificity, accuracy, and AUC of mammography with VTQ were 81.8%, 86.4%, 84.7% and 0.84, respectively. And of mammography with SWV ratio was 85.5%, 88.5%, 87.4% and 0.87, respectively. The sensitivity, specificity, accuracy, and AUC of US with VTQ were 83.6%, 90.0%, 86.7% and 0.87, respectively. While of US with SWV ratio was 85.5%, 94.8%, 91.0% and 0.90, respectively, Table 2. The sensitivity, specificity, accuracy, and AUC of VTQ and VTQ with mammography were significantly higher than those of mammography (P < 0.05). And the sensitivity, specificity, accuracy, and AUC of the SWV ratio were significantly higher than those of mammography (P < 0.05), while higher than VTQ with no statistically significant differences (P > 0.05). And the sensitivity, specificity, accuracy, and AUC of the SWV ratio with mammography were significantly higher than those of mammography (P < 0.05), while higher than VTQ and VTQ with mammography with no statistically significant differences (P > 0.05).
Diagnostic performances of mammography, US, VTQ, SWV ratio, mammography with VTQ, mammography with SWV ratio, US with VTQ, US with SWV ratio
The occurrence of breast cancer had a tendency toward young, which brings great physical and mental pain to females. Mammography has the characteristics of low X-ray tube voltage, low energy, long wavelength, weak penetrability, etc, particularly suitable for the diagnosis of early breast cancer without mass or only with clustered microcalcifications, such as ductal carcinoma in situ. However, Chinese women tend to have dense breast tissue that X-rays cannot easily penetrate, which may lead about 5% to 15% of breast cancers not to be detectable by mammography, especially in breast cancers with the characteristics of small lesions, near chest wall lesions, and multifocal lesions [19–21]. It is controversial in the diagnostic application of mammography in the differential diagnosis of breast lesions of Chinese. The sensitivity of mammography was 55.4% in our study, significantly lower than that of VTQ, SWV ratio and the combined use of them, which is consistent with the SHao SH et al. study [22]. But the diagnostic performance of it was lower than the Pan J et al. study [23], it may be affected by the density of breast tissue and the experience of the radiodiagnostic [24, 25].
The conventional US has a higher sensitivity in the differential diagnosis of breast lesions, but its specificity is low according to the US BI-RADS criteria, especially in dealing with BI-RADS of category 4 breast lesions, where the risk of malignancy ranges from 2% to 94% [26–28]. In our study, US with the cutoff value of BI-RADS-US 4A exhibited better sensitivity (74.5%), specificity (76.0%), accuracy (75.5%) and AUC of it was 0.75, which is consistent with previous studies [25, 29]. Elastography, a non-invasive and reliable method, as a complement to the conventional US, has shown promise in differentiating low-risk lesion [29, 30]. A newly developed elastic imaging technique named ARFI, it including VTI, VTQ and VTIQ. Li et al. [17]. set VTI score ≥4 as the cut-off value, the sensitivity, specificity, accuracy and AUC of VTI were 83.0%, 76.8%, 79.3% and 0.81, respectively. VTQ with the cutoff value of 5.01 exhibited better sensitivity (76.4%), specificity (85.4%), accuracy (82.1%) and AUC of it was 0.81 in differentiating 151 lesions in our study, which is consistent with previous studies [29, 32]. The diagnostic performance of mammography with VTQ has a better sensitivity (81.8%), specificity (86.4%), accuracy (84.7%) and AUC(0.84) than mammography. When the VTQ was combined with US, it also improved the sensitivity (83.6%), specificity (90.0%), accuracy (86.7%) and AUC(0.87), and the previous studies have the similar results [32, 33]. Li et al. reported that the combination of VTI with VTIQ could yielded sensitivity, specificity and accuracy of 95.7%, 66.7% and 78.4%, respectively [17], which is consistent with Han J et al. study [34].
Yao et al. pointed out that the tumor margins and the distribution of blood flow in the tumor can affect the SWV measurement [35]. Our study shows that the SWV of the surrounding parenchyma in malignant lesions was 2.58±1.49 m/s (mean±SD), while in the benign lesions, was 2.66±1.82 m/s (mean±SD). The SWV ratio of the lesion-to-surrounding parenchyma of malignant lesions was 4.89±1.93, while in the benign lesions the ratio was 1.82±0.63, there were statistically significant differences between the malignant and benign lesions in SWV and SWV ratio of the surrounding parenchyma (P < 0.05). The cutoff value of the SWV ratio of 2.43 yielded a sensitivity of 78.2%, a specificity of 86.5%, an accuracy of 83.4% and AUC of 0.83, which were statistically significantly higher than those of mammography, while VTQ with no statistically significant differences Fig. 3. The sensitivity, specificity, accuracy, and AUC of the SWV ratio with mammography were 85.5%, 88.5%, 87.4% and 0.87, respectively. The diagnostic performance of the SWV ratio with mammography was statistically significantly higher than those of mammography, while no statistically significantly higher than the diagnostic performance of VTQ, VTQ with mammography and SWV ratio.

A 64-year-old female with breast lesion was histopathologically confirmed to be invasive ductal carcinoma. The SWV in lesion is X.XX m/s (X.XX was recorded as 9.0 m/s corresponding to the solid portion) (A) and 2.45 m/s in surrounding parenchyma (B) at VTQ.
Compared to the results of different diagnostic methods in our study, we found that the single and combination use of the SWV ratio can improve sensitivity without sacrificing diagnostic specificity in the process of breast cancer diagnostic. It illustrates that the SWV ratio has an important role in the differential diagnosis of breast lesions, it was helpful to improve the differential diagnosis performance of breast lesions.
Our study has several limitations. First, the SWV values measured were limited by the the fixed region of interest (ROI) (i.e., 6 mm×5 mm) and the limited SWS measurement range (i.e., 0.5–9.0 m/s); if the SWV values of a breast lesion exceeded the upper limit or the largest diameter <6 mm, the SWV values measured was affected. Second, the SWV measurement is affected by the respiratory movements and cardiac motion of the patient, which may affect the VTQ values in our study. Third, the pathological types of breast lesions in this study were limited, many pathological types of breast malignancies were not represented in our sample; further, the sample size is limited in this study, therefore, more studies are necessary.
In conclusion, our clinical experience is that the SWV ratio can improve the sensitivity without sacrificing diagnostic specificity in the process of breast cancer diagnostic and avoid unnecessary biopsy or surgery.
Footnotes
Acknowledgments
The study was supported in part by Grant PW2014D-7 from Shanghai Pudong District Municipal Commission of Health and Family Planning, Shanghai, China.