
Abstract
BACKGROUND:
Renal ischemia-reperfusion (I/R) injury often occurs in various clinical events, and its incidence and mortality have been increasing.
OBJECTIVE:
To investigate the value of contrast enhanced ultrasonography (CEUS) in the monitoring of dexamethasone in the improvement of renal I/R injury in rats.
METHODS:
Eighteen healthy male Sprague-Dawley rats were randomly divided into sham-operated, I/R, and I/R surgery plus dexamethasone treatment (Dexa) groups. In the I/R group 45-minute renal ischemia with 24 h reperfusion period was monitored. Time-intensity curve (TIC)-derived parameters, which included peak value, time to peak (TP), area under the curve (AUC), and mean transit time (MTT) were compared to the blood creatinine, urea, Caspase-1, and NLRP3 levels.
RESULTS:
The I/R group showed an increased peak value, prolonged TP and MTT, and greater AUC (P < 0.05). The Dexa group showed shorter TP and MTT, and smaller AUC (P < 0.05). Results show that the associations between (i) TP, AUC, and MTT and (ii) creatinine, urea, Caspase-1, and NLRP3 levels were significant (P < 0.05).
CONCLUSION:
Dexamethasone can alleviate renal I/R injury in rats, which may be related to the inhibition of NLRP3 and caspase-1. CEUS can quantitatively measure this change, in which the changes in TP, AUC and MMT values have considerable reference values.
Introduction
Renal ischemia-reperfusion (I/R) injury occurs when blood supply is restored after a period of ischemia. It results in renal tissue damage, which could be irreversible. I/R injury is mainly induced by perioperative procedures for kidney transplantation, cardiovascular surgery, aortic repair, etc. [1, 2]. The pathogenesis of renal I/R injury is complex, and it is a multi-factor, cascading, and complex pathological process. Studies have found that renal I/R injury is related to the pathogenesis of inflammatory response, apoptosis, autophagy, oxidative stress, pyroptosis, and micro-rheological parameters, etc. among which the inflammatory response mechanism plays an important role in the occurrence and development of renal I/R injury [3–5]. Renal I/R-induced acute kidney injury is an important cause of morbidity. There are many ways (pharmacological, physical, surgical preconditioning, and various ischemic preconditioning techniques) to protect kidneys from I/R injury, but it is not clear which method is best [6]. Therefore, it is necessary to explore effective diagnostic and therapeutic methods.
Contrast enhanced ultrasonography (CEUS) is a quantitative imaging technique in which highly echogenic microbubbles are utilized as contrast agent to improve the contrast and increase the sensitivity and specificity for blood flow measurement [7]. The size of microbubbles is comparable to that of red blood cells. After intravenous injection, microbubbles distribute throughout the body through the blood circulation. Using microbubbles for signal enhancement, measuring the ultrasound echo signal over time at the same location, a time-intensity curve (TIC) can be drawn (with time on the horizontal axis and signal intensity on the vertical axis). Then, a log-normal curve is fitted to the data, which is used to calculate parameters such as peak value, time to peak (TP), area under the curve (AUC), mean transit time (MTT), and wash-in and wash-out in the region of interest (ROI). These parameters could quantitatively reflect the blood flow characteristics of the organ, and have been used widely for the evaluation of acute pyelonephritis [8], diffuse proliferative nephritis [9], renal mass [10], renal cortical blood perfusion, and renal transplantation [11]. Researchers have demonstrated good correlation between TIC-derived parameters and renal blood perfusion [12].
Dexamethasone is a synthetic corticosteroid that is widely used in clinical settings for its anti-inflammation, immuno suppression, and anti-rheumatoid properties. Studies have demonstrated that dexamethasone can effectively alleviate I/R-induced kidney injury [13–15]. The NACHT, LRR, and PYD domains containing protein 3 (NLRP3) inflammasome is a cytoplasmic macromolecular complex. The NLRP3 inflammasome acts as an intracellular sensor that detects a broad range of microbial motifs and endogenous danger signals (e.g., I/R) and orchestrates inflammatory and innate immune responses. Activation of the NLRP3 inflammasome triggers activation of Caspase-1, which is required for processing and release of active proinflammatory cytokines, such as IL-1β and IL-18, and subsequent local inflammation [16, 17]. The vascular inflammatory reaction also plays important roles in renal I/R injury. Renal ischemia induces an inflammatory cytokine signaling cascade, and inhibition of the inflammatory response could effectively alleviate renal I/R injury [18–20].
In this study, we aimed to investigate the renal cortical blood flow changes before and after dexamethasone treatment in I/R injury in rats using CEUS, to analyze the association between TIC-derived parameters and renal biochemical parameters, and to investigate whether dexamethasone protects the kidney from I/R injury via inhibiting NLRP3 and Caspase-1 expression.
Materials and methods
Animals and groups
Eighteen healthy adult male Sprague-Dawley rats (200–250 g) were purchased from the Laboratory Animal Center of Southwest Medical University. Animals were accommodated for one week before the surgical procedure with water and food ad libitum. The rats were randomly allocated to one of the following groups: the sham group (n = 6); the I/R group (n = 6); and the I/R surgery plus dexamethasone treatment (Dexa) group (n = 6). Rats in the Dexa group received dexamethasone (5 mg/mL, dose: 4 mg/kg, intraperitoneal injection) 1 hour before the onset of ischemia. Sham and I/R rats received an equal volume of 0.9% saline (intraperitoneal injection) 1 hour before the onset of ischemia.
Rat renal I/R injury model
All rats were anesthetized with intraperitoneal injection of 10% chloral hydrate (100 mg/mL, dose: 2 mL/kg) and 0.2% ropivacaine hydrochloride was administered subcutaneously for pain control. The position of the rat kidneys was determined using pre-operative two-dimensional ultrasonography. Preparation of the kidney area for surgery included hair removal and iodophor disinfection. Rats were placed in the prone position. A midline incision was made and tissue was separated layer by layer. The ureter was separated, right nephrectomy was performed after ligation of the right renal pedicle with a 2.0 mm suture, and the left renal pedicle was clamped for 45 min with a nontraumatic vascular clip. The ischemic status was determined by visual inspection of the color of the left kidney. After the color of the entire left kidney changed from bright red to dark red, the clamp was kept for 45 min. It was released to allow blood flow, which was indicated by the return to their original bright red color. The abdomen was closed in layers. The sham surgery consisted of right nephrectomy and isolation of the left renal pedicle, except that clamps were not applied. After surgery, animals had water and food ad libitum.
All animal experiments were carried out in accordance with Institutional Animal Care and Use Committee guidelines. All surgical procedures were performed under anesthesia, and reasonable efforts were made to minimize animal suffering.
Contrast enhanced ultrasound imaging
At 24 h after surgery, rats were anesthetized and secured. An ACUSON S3000 ultrasound imaging system equipped with 9L4 Multi-d Transducer was used. The probe was oriented and fixed at the maximum coronal cross-section of the left kidney. Imaging was initiated. The ultrasound imaging parameters were set as: frequency 4.0 MHz, depth 4 cm, and mechanical index (MI) 0.1. SonoVue® (manufactured by Bracco Imaging and distributed by Bracco Sine Shanghai, China) was used as contrast agent. In accordance with the manufacturer’s instructions, 5 mL saline, which contained 25 mg of freeze-dried SonoVue powder, which is equivalent to 59 mg sulfur hexafluoride, was injected into the ampule. Microbubble suspension was made by shaking the ampule vigorously. Then the contrast agent was bolus injected via the tail vein (dosage 0.4 mg/kg), followed by 0.2 mL saline flush. While the contrast agent was injected, the images were collected simultaneously, and images were recorded continuously for 3 min. Auto-tracking contrast quantification software (Siemens) was used for TIC analysis. In brief, a circular ROI with an area of 0.05 mm2 was placed within the cortex at the maximum coronal section. The TIC was drawn, and the following parameters were derived: peak value, TP, AUC, and MTT. The analysis was repeated three times.
Renal function assessment
After CEUS, the 2.0 mL blood was extracted from the caudal caval vein after anaesthesia and centrifuged at 3000 rpm at room temperature for 10 min. The supernatant was collected and submitted to the Clinical Laboratory of the Affiliated Hospital of Southwest Medical University for the measurement of serum creatinine and urea levels.
Histologic evaluation
After blood extraction, the rats were euthanized. Half of the kidney was fixed in 10% neutral buffered formalin solution, paraffin-embedded, sectioned, and stained with hematoxylin and eosin (HE). The HE staining results were evaluated by the Department of Pathology of Southwest Medical University.
Immunohistochemistry
Immunohistochemistry was performed to measure the renal expression levels of Caspase-1. Formalin-fixed rat kidney was dehydrated and embedded using an automatic histology processer. After sectioning and wax removal, the slides were immersed in the staining chamber, washed three times with PBS, blocked with goat serum at room temperature for 20 min, incubated with polyclonal rabbit anti-Caspase-1 (1 : 50) at 4°C overnight, and incubated with biotinylated goat anti-rabbit secondary antibody (SP-9001, ZSGB-BIO, Beijing) at 37°C for 30 min. The sections were washed three times with PBS for 5 min and the signal was generated using a DAB IHC staining kit. In brief, the reagents were mixed as instructed and added to the sections. The color was allowed to develop at room temperature until the desired intensity, which typically took about 2 min. Then, the slides were washed with distilled water, counterstained with hematoxylin, dehydrated, cleared, and finally sealed using neutral balsam mount medium. The stained slides were first observed under 100×magnification to pick three optimal fields, which were further examined under 400×magnification for quantitative analysis. The integrated optical density, area, and mean density of each selected field were analyzed using Image-Pro Plus 6.0 software. Then the average values of three fields were calculated and used to represent the values of the whole slide.
Real-time quantitative polymerase chain reaction (PCR)
Real-time quantitative PCR was used to measure the NLRP3 mRNA levels. Total RNA was extracted from renal tissue using TRIzol according to the manufacturer’s instructions (Invitrogen, USA). cDNA was synthesized using PrimeScript RT reagent Kit (Solarbio Bioscience & Technology Co., Ltd., Dalian, China). PCR reactions were conducted using a Real-time PCR system (Thermo fisher Scientific Inc., USA). The primers are listed in Table 1. The PCR conditions were as follows: pre-denaturation at 95°C for 30 s, followed by 40 cycles of 95°C for 5 s; 55°C for 30 s, and 72°C for 30 s. β-Actin was used as internal reference. The relative expression levels were calculated using the 2–ΔΔCT method.
Primers used in PCR
Primers used in PCR
NLRP3: NACHT: LRR: and PYD domains containing protein 3; PCR: polymerase chain reaction.
SPSS v. 20.0 was used for data analysis. Numerical data are presented as mean±SD. The comparison between groups was performed using ANOVA. The Spearman correlation coefficient was used to describe the association between different parameters. A P value less than 0.05 was considered to indicate a statistically significant difference.
Results
Dexamethasone alleviates renal I/R injury
The creatinine and urea levels in the I/R group were 69.33±12.02μM and 29.11±6.08 mM, i.e., a threefold and fourfold increase compared to the sham group, respectively. The results indicated impaired renal function after I/R injury (P < 0.05). The creatinine and urea levels of the Dexa group were 41.10±7.83μM and 14.18±1.28 mM, respectively, which were significantly lower than those of the I/R group. These results suggest that dexamethasone treatment prevents impairment of real function (Fig. 1A, B).
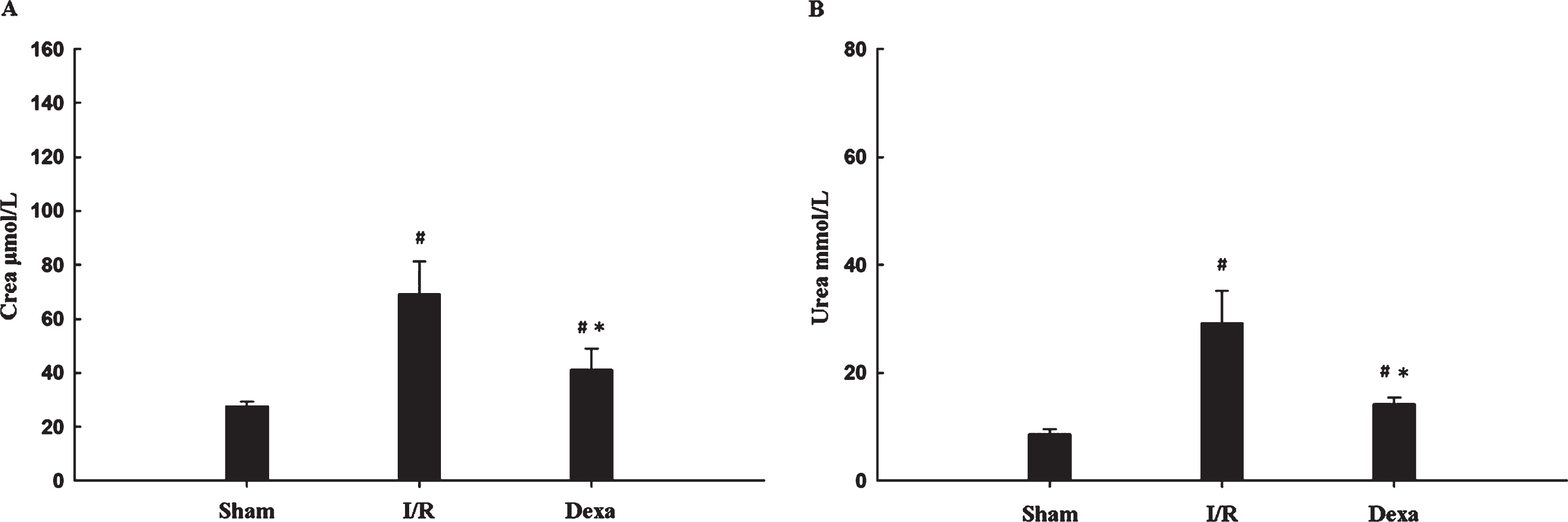
Blood creatinine and urea levels in the three groups of rats. (A) Blood creatinine levels. (B) Blood urea levels. The Dexa group had significantly lower blood creatinine and urea levels than the I/R group. #P < 0.05 compared with the sham group; *P < 0.05 compared with the I/R group. Dexa: dexamethasone treatment; I/R: ischemia-reperfusion.
To further validate the above results, we examined the histopathology of renal tissue sections. Compared with the sham group (Fig. 2A), the I/R group showed evident renal injury at 24 hours after I/R, with the histopathological changes including tubular dilatation, tubular cell swelling, cellular vacuolization, loss of tubular brush border, medullary congestion, edema, and inflammatory cell infiltration (Fig. 2B). In contrast, the Dexa group showed slight congestion, slight edema of tubular cells, and slight interstitial edema (Fig. 2C). These results demonstrate that dexamethasone treatment reduces I/R-induced renal injury.
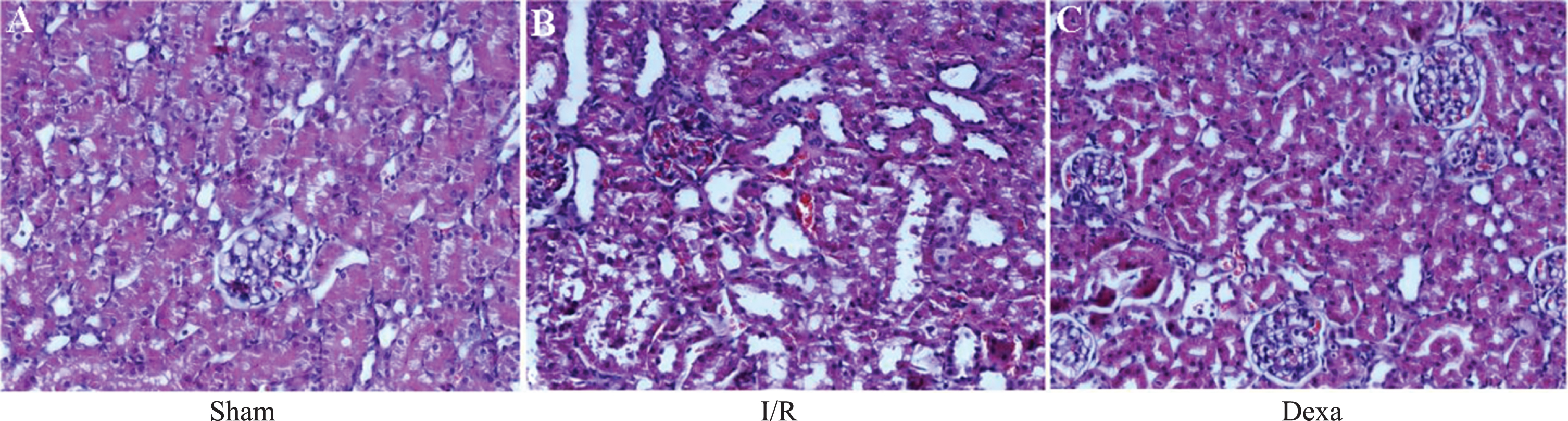
Histopathological examination of kidneys of the three groups of rats (magnification×200). (A) Sham group. (B) I/R group. (C) Dexa group. Dexa: dexamethasone treatment; I/R: ischemia-reperfusion.
To investigate the mechanisms underlying the protective effects of dexamethasone against renal I/R injury, we performed real-time PCR to evaluate the NLRP3 mRNA levels. The 2–ΔΔCt method was used to evaluate the relative quantification results, and β-actin was used to normalize the results. The results show that the NLRP3 mRNA levels were significantly higher in the I/R group than in the sham group (P < 0.05). In the Dexa group, NLRP3 mRNA levels were significantly lower than in the I/R group (P < 0.05). These results demonstrate that renal NLRP3 mRNA levels were enhanced upon I/R injury, and dexamethasone treatment markedly reduced I/R-induced enhancement of renal NLRP3 mRNA expression (Table 2).
Comparison of the biochemical variables between groups (mean±SD)
Comparison of the biochemical variables between groups (mean±SD)
#P < 0.05 compared with the sham group; *P < 0.05 compared with the I/R group. Dexa: dexamethasone treatment; I/R: ischemia-reperfusion; NLRP3: NACHT, LRR, and PYD domains containing protein 3; PCR: polymerase chain reaction; SD: standard deviation.
To investigate whether I/R-induced activation of the NLRP3 inflammasome could further activate Caspase-1, immunohistochemistry was carried out to measure Caspase-1 expression levels in the kidney. Negative cells were stained blue, and the substrate was stained white (Fig. 3A); positive cells were stained yellow or yellowish brown, and the anti-Caspase-1 reaction product was mainly located in the cytosol (Fig. 3B). The renal Caspase-1 protein levels in the I/R group were significantly higher than in the sham group (P < 0.05), and in the Dexa group they were significantly reduced compared with the I/R group (P < 0.05) (Table 2). These results indicate that I/R-induced activation of the NLRP3 inflammasome upregulates renal Caspase-1 expression in the kidney. Dexamethasone treatment inhibits the upregulation of Caspase-1 and therefore alleviates renal I/R injury.
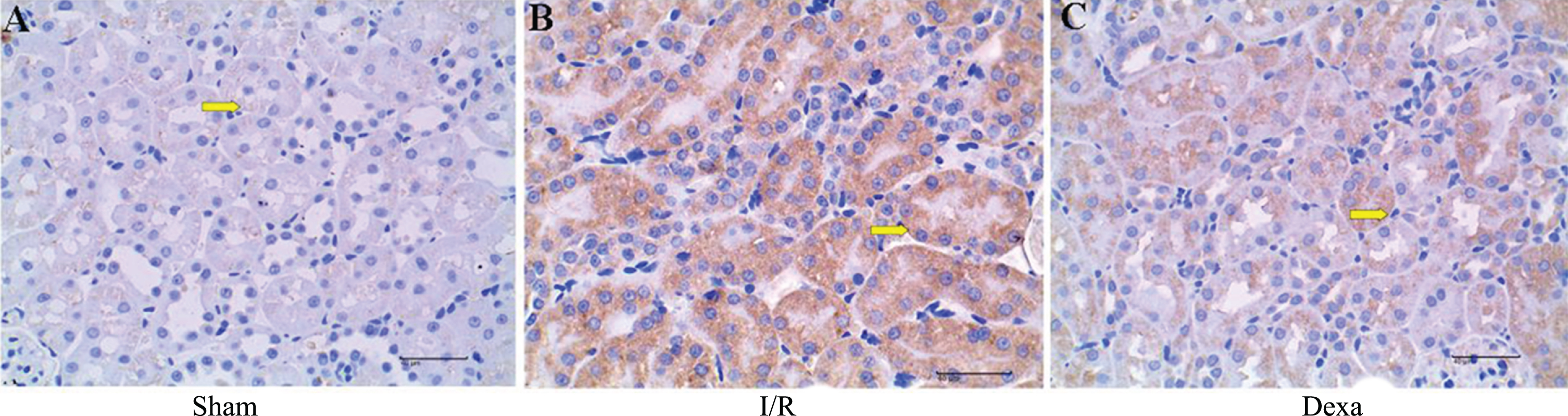
Histological sections of kidneys in three groups were stained with anti-Caspase-1 antibody (magnification×400). (A) Sham group. (B) I/R group. (C) Dexa group. Negative cells were stained blue, with white substrate. Positive cells were stained yellow or brownish-yellow. Dexa: dexamethasone treatment; I/R: ischemia-reperfusion.
After intravenous bolus injection of contrast agent via the tail vein, the renal arteries (renal arteries, segmental arteries, renal interlobar arteries, and renal arcuate arteries), cortex, and pyramid were clearly displayed in sequence, which has been described as “fireball-like” signal enhancement. The signal intensity peaked rapidly, and then gradually decreased to baseline in the medulla, cortex, and renal artery in sequence. The TICs of the ROIs were analyzed. As shown in Fig. 4A, the TIC of renal cortical perfusion in the sham group showed an obvious steep ascending slope, a peak, and a descending slope. In the I/R group, renal function was impaired, and the renal hemodynamics were altered. As a result, the TIC in the I/R group showed flatter ascending and descending slopes compared with the sham TIC (Fig. 4B). However, dexamethasone pre-treatment improved renal hemodynamics. As shown in Fig. 4C, the ascending and descending slopes in the TIC of the Dexa group were steeper than those of the I/R group, but still not as steep as those of the sham group.
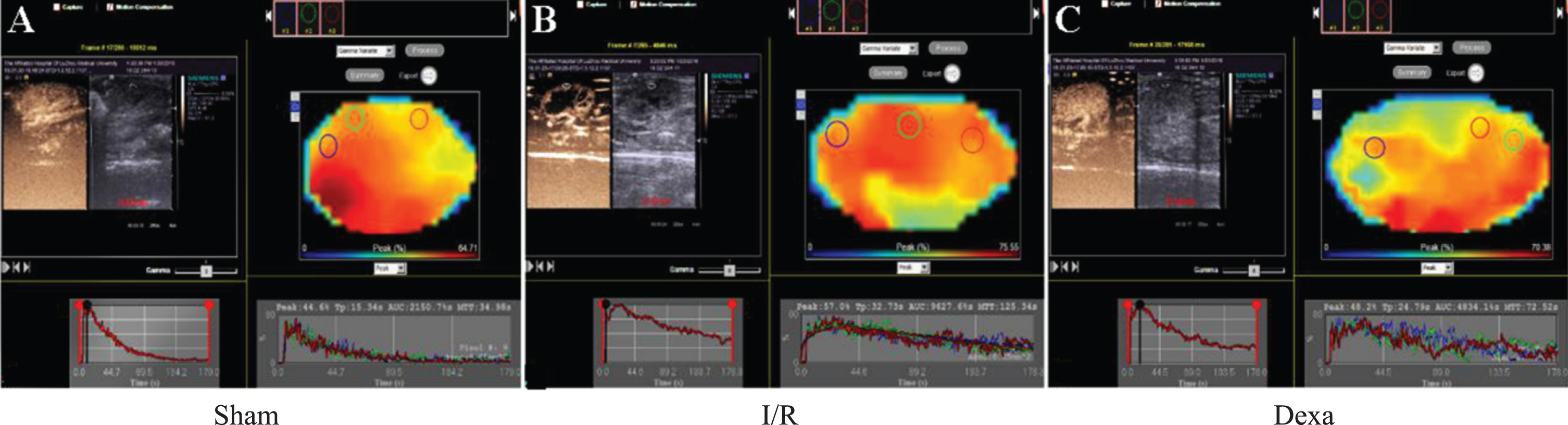
Contrast enhanced ultrasound imaging and TIC analysis of the three groups of rats. (A) The sham group showed normal renal cortical blood flow, and its TIC had steep ascending and descending slopes. (B) The I/R group showed impaired renal cortical blood flow, and its TIC had flatter ascending and descending slopes. (C) The Dexa group showed improved renal cortical blood flow and steeper ascending and descending slopes compared with the I/R group. Dexa: dexamethasone treatment; I/R: ischemia-reperfusion, TIC: time-intensity curve.
One-way ANOVA was used to compare the differences in peak value, TP, AUC, and MTT between groups. The results show that peak values did not differ significantly between the I/R and Dexa groups (P > 0.05). However, TP, AUC, and MTT values were significantly different between the sham, I/R, and Dexa groups (P < 0.05) (Table 3). These results suggest that the peak value of the TIC does not accurately reflect the changes in renal cortical perfusion.
Comparison of TIC-derived variables between groups (mean±SD)
Comparison of TIC-derived variables between groups (mean±SD)
#P < 0.05 compared with the sham group; *P < 0.05 compared with the I/R group. AUC: area under the curve; Dexa: dexamethasone treatment; I/R: ischemia-reperfusion; MTT: mean transit time; SD: standard deviation; TIC: time-intensity curve; TP: time to peak.
To evaluate the potential application and significance of TIC analysis of blood flow in the renal cortex after contrast enhanced ultrasound imaging, the Spearman correlation coefficient was used to describe the association between all parameters. Our analysis results show that the Spearman correlation coefficients between creatinine levels, urea levels, and the peak value were of statistical significance (P < 0.05), while the Spearman correlation coefficients between NLRP-3, Caspase-1, and the peak value were not significant (P > 0.05). The renal panel parameters, i.e., Caspase-1 protein levels, NLRP3 mRNA levels, creatinine levels, and urea levels, were significantly associated with TP, AUC, and MTT values (P < 0.05) (Table 4). The results show that the changes in AUC, TP, and MTT values are valuable parameters for the evaluation of blood perfusion status before and after renal I/R injury.
Correlation between biochemical and cortical TIC-derived variables
Correlation between biochemical and cortical TIC-derived variables
*P < 0.05; **P < 0.01; ***P < 0.001. AUC: area under the curve; MTT: mean transit time; NLRP3: NACHT, LRR, and PYD domains containing protein 3; TIC: time-intensity curve; TP: time to peak.
Our experiments demonstrate that dexamethasone attenuates kidney injury in an I/R rat model. Upon I/R, dexamethasone reduced blood creatinine and urea levels and mitigated renal histopathological damage. The TIC derived from CEUS of the renal cortex exhibited consistent changes. In addition, dexamethasone treatment reduced the expression levels of NLRP3 and Caspase-1 in renal tissues, suggesting that it protects the kidney from I/R injury via inhibiting the expression of the NLRP3 inflammasome possibly, which has not been shown before. Another innovation of this study is that we investigated the mechanisms underlying renal I/R injury while using CEUS as a monitoring technique.
SonoVue is an ultrasound contrast agent that contains sulfur hexafluoride lipid microspheres. It is a purely intravascular agent, distributes throughout the whole body, is not affected by the glomerular filtration rate and tubular reabsorption, has no contrast interstitial or urinary extravasation, and is excreted only through the lungs without any renal toxicity [21]. Studies have shown that blood perfusion is closely associated with the initiation, development, and prognosis of many renal diseases. Due to the fact that cortical blood flow comprises ∼90% of the total renal blood flow, we analyzed blood perfusion of the entire kidney using the renal cortex as ROI [22]. Contrast enhanced renal perfusion images of the ROI were converted into a TIC. Hemodynamic parameters, i.e., peak value, TP, MTT, and AUC, were derived from the TIC using regression with the gamma model. Using these parameters, the blood flow in capillaries, tissue, and whole organ can be measured quantitatively in real-time. Studies have shown that CEUS could quantitatively measure the changes in renal blood flow during the different stages of I/R injury or after treatment [23, 24].
In this study, rat renal I/R models were created as per previously published articles [6, 25]. Through many preliminary experiments, we found that this method to be the most effective. Renal hemodynamics were significantly changed at 24 h after I/R injury. The peak value was highest in the Dexa group, followed by the I/R group; it was lowest in the sham group. However, the peak value did not differ significantly between the I/R and Dexa groups, and the association coefficient between peak value and renal panel parameters was not significant (P > 0.05). These results are consistent with a study by Li et al. [26], who investigated the association between renal cortical TIC parameters and intracellular adhesion molecule-1 (ICAM-1) expression in a rabbit I/R model. It was found that the peak value is not a quantitative indicator for renal cortical blood flow because it only reflects the transient, not the cumulative, maximum signal intensity within the ROI. At 24 h after renal I/R surgery, the TP and MMT were prolonged and the AUC was increased. TP was defined as the interval from the moment when the contrast agent first enters the cortex to the moment when signal intensity in the cortex reached its peak. MTT was defined as the interval from the moment when the contrast agent first entered the cortex to the moment when the peak intensity fell to half. These parameters reflect the wash-in and wash-out rates of the contrast agent. Ischemia and hypoxia trigger vasoconstriction, endothelial cell responses, infiltration of various inflammatory cytokines, flow impairment, and the formation of thrombi in the microcirculation, which eventually lead to reduced blood flow in the renal cortex [27]. Such changes could be detected by CEUS and manifested as reduced wash-in and wash-out rates of contrast agent, i.e., prolonged MTT and TP on the TIC. The AUC is a measure of the total cumulative volume in a certain time period in the ROI. Upon I/R injury, the permeability of endothelium increases. The inflammation mediators facilitate the homing and adherence of inflammatory cells to the injured blood vessel endothelium. Microbubbles can be phagocytosed by activated inflammatory cells and still maintain their acoustic characteristics. Therefore, the ultrasound signal may intensify at the sites of inflammation, leading to a larger AUC [28]. TIC analysis showed that after dexamethasone treatment, MTT and TP were shorter, and the AUC was smaller. This might be a result of the fact that exogenous dexamethasone inhibits the expression of NLRP3 and Caspase-1, inhibits the release of inflammation mediators and infiltration of inflammatory cells, reduces microcirculatory resistance, and improves perfusion of the renal cortex. These effects manifested as increased contrast agent wash-in and wash-out rates and shortened TP and MTT on the TIC. Inhibition of inflammation also led to reduced phagocytosis of microbubbles by inflammatory cells, and consequently less accumulation of microbubbles with a certain time period, which manifested as a reduced AUC of the TIC.
Dexamethasone is a commonly used corticosteroid. Studies have demonstrated that dexamethasone alleviates I/R injury in many organs, including the brain, heart, kidneys, lungs, and intestines, and tourniquet-induced acute hind limb I/R injury in mice [29–33]. Dexamethasone protects tissue from I/R injury via several mechanisms. (1) Glucocorticoid receptor (GR) is expressed in almost every cell in the body, including lung, liver, and kidney cells. When glucocorticoids bind to GR, the receptor-glucocorticoid complex enters the nucleus, where it binds to an array of DNA sequences, regulating transcription of a range of target genes, and consequently inducing or downregulating the synthesis of target proteins, thereby exerting pharmacological effects [34]. (2) Dexamethasone decreases membrane fluidity, reduces the production and release of inflammatory cytokines and mediators, and eventually alleviates local inflammation. (3) Dexamethasone inhibits the adhesion of neutrophils to endothelium, reduces the obstruction of microvessels by neutrophils and thrombi, and therefore improves micro-circulation and prevents the no-reflow phenomenon observed in I/R injury [35]. (4) Upon renal I/R injury, the expression levels of eNOS decrease, while those of iNOS increase. The disturbed eNOS/iNOS ratio leads to dysregulation of NO levels in tissue and hence causes renal damage. Dexamethasone alleviates renal damage by upregulating the eNOS/iNOS ratio [15]. Inflammasomes are cytosolic multiprotein oligomers. The NLRP3 inflammasome is one of the best characterized inflammasomes and is currently a popular research topic. One of the characteristics of NLRP3 inflammasome-dependent responses is the requirement of an initial priming stimulus by a pathogen-associated molecular pattern (PAMP) or damage-associated molecular pattern (DAMP). The NLRP3 inflammasome consists of NLRP3, apoptosis-associated speck-like protein containing CARD (ASC), and Caspase-1. The NLRP3 inflammasome plays central roles in the triggering of inflammatory responses, while inhibition of the NLRP3 inflammasome or NLRP3 expression can effectively attenuate renal I/R injury [5, 36]. Therefore, research focusing on the NLRP3 inflammasome could aid in the development of novel treatment approaches for the management of renal I/R injury.
Conclusions
In summary, CEUS combined with TIC analysis is of high application value in the detection and evaluation of drug effects on renal I/R injury. Among TIC-derived parameters, TP, MTT, and AUC have significant value. Dexamethasone protects the kidney from I/R injury by inhibiting NLRP3 and Caspase-1 expression possibly. Further studies of the NLRP3 inflammasome could lead to novel treatment strategies for renal I/R injury. However, the pathologic mechanisms underlying renal I/R injury are complicated. The tolerance of the rat kidney may be different from that of the human kidney. When the basic experimental results are fully applied to the clinical settings, they may also be influenced by a variety of clinical factors [37]. For these reasons, more comprehensive preclinical and clinical research is needed to elucidate the mechanisms underlying renal I/R injury and to provide information to improve clinical management. CEUS is a sensitive, feasible, and noninvasive technique, and offers great research and application potential.
Footnotes
Acknowledgments
This work was supported by the Education Department of Sichuan.