
Abstract
BACKGROUND:
Platelet activation is associated with abdominal obesity and exercise training is an important modulator of body weight.
OBJECTIVE:
We investigated the effects of two high intensity interval exercise (HIIE) protocols of different intensity and duration on platelet indices and platelet aggregation in overweight men.
METHODS:
Ten overweight men performed 6 intervals of 30s exercise at 110% of peak power output (PPO) interspersed by 3 : 30 min active recovery (1/7 protocol) at 40% of PPO and 6 intervals of 2 min exercise at 85% of PPO interspersed by 2 min active recovery (1/1 protocol) at 30% of PPO in two separate sessions. Platelet indices and platelet aggregation were measured before and immediately after both HIIEs.
RESULTS:
Platelet indices increased significantly following HIIE (P < 0.05), though, significant differences between the two protocols were only detected for platelet count, which was markedly increased following 1/1 protocol. Platelet aggregation increased significantly (P < 0.05) in response to the two HIIE protocols, with no significant difference being observed between the two protocols (P > 0.05).
CONCLUSIONS:
It is concluded that HIIE leads to transient increases in markers of thrombus formation and that work to rest ratio is an important factor when investigating the changes in thrombocytosis following HIIE.
Introduction
Platelet hyper-activation and impaired platelet function participate to the pathogenesis and progression of cardiovascular disease [1, 2]. Platelet activation and aggregation can lead to thrombosis and are influenced by physiological stresses including high shear stress and inflammation [3, 4].
There is a consensus that acute exercise can significantly affect platelet function parameters [5–8] with exercise intensity being a strong modulator [9, 10]. It is believed that high-intensity exercise can increase catecholamine release, promote spleen contraction, inhibit nitric oxide (NO) and promote secretion of p-selectin, which, all result in platelet aggregation and thrombosis [5, 12]. Furthermore, moderate to vigorous exercises have been shown to cause a rise in several indices of platelet activity such as beta-thromboglubin, platelet factor 4 and thromboxane A2 [13]. Ikarugi et al. [12] have shown that thrombotic risk increases only after high-intensity exercise, but not with low-intensity exercise [12, 14]. In addition, there is a potential risk of complex events such as myocardial infarction (MI) not only during strenuous exercise [5–7], but also during the recovery period following exercise [15]. Platelet dysfunction may play an important role in MI during and after high-intensity exercise [16].
High intensity interval training (HIIT) has recently been introduced and prescribed for different populations including athletes, healthy individuals and patients to improve performance, and to prevent and treat many different diseases including cardiovascular disease [17–19]. Although acute high intensity exercise may increase the risk of an adverse cardiac event, HIIT could be useful amongst different patient populations [19, 20]. Recently, Miron et al. [10] have suggested that high intensity interval exercise (HIIE) may increase platelet aggregation even in trained individuals. Some of the exercise variables (i.e. intensity and duration) that form the structure of interval exercise program may be important factors to minimize the exercise risk whilst maximize the benefits. Based on a review [21] there are different key factors that may be manipulated when designing HIIE protocols, such as the intensity and duration of work and recovery, and the work to rest ratio. The work to rest ratio during this type of exercise has recently been confirmed as an important factor when designing HIIT or investigating the risk of HIIE [22]. In our previous study [23], we found that the risk for exercise-induced thrombosis was higher during HIIE compared to moderate continuous exercise (MCE) in patients with recent revascularization. However, it was unclear whether this was caused by the higher work to rest ratio in the HIIE or due to other exercise variables such as intensity.
Overweight people have an increased risk for coronary heart disease [24] and an association between android obesity and platelet dysfunction has been reported [25]. Physical activity programs are recommended in overweight people and improvements in cardiorespiratory fitness and body composition have been reported following high intensity interval training in this population [26]. Since exercise duration, volume and intensity are exercise variables that might promote thrombocytosis and platelet activation in overweight persons, there is a need to determine the type of HIIE protocol that would stimulate thrombocytosis and platelet aggregation less.
To our knowledge no previous study has investigated the effects of different HIIE protocols on platelet indices and function in overweight individuals. Since different HIIE protocols might induce different physiological stresses and responses [22], we hypothesized that HIIE with a higher work/rest ratio (1/1) but lower intensity would induces higher platelet responses and potential thrombogenesis than HIIE with a lower work/rest ratio (1/7) but higher intensity.
Materials and methods
Subjects
The study participants consisted of twelve overweight men (Mean±SD: age, 24.8±1.39 yrs; BMI, 27.4±1.43 kg/m2) who were non-smokers, not taking “platelet - active” medications, had no history or diagnosed signs of cardiovascular diseases, and did not participate in regular exercise. The university research and ethics committee approved the exercise protocol and laboratory procedures (approval no. SBU.ICBS.95.1004). This study was conducted in accordance with the Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Subjects. Prior to the experiments, all participants were fully informed about the aims and procedures of the study and a written consent was obtained.
Experimental design
Participants came to the laboratory on three separate occasions each separated by one week. The first session was designed to familiarize the participants with laboratory equipment, testing protocols and measurements of height (Seca, UK), body mass (Seca, UK), BMI (weight divided by height squared) and peak power output (PPO). At the second and third sessions all participants performed two different HIIEs in random order. They were asked to avoid any vigorous exercise for at least 48 h before the experiments.
Determination of peak power output
After a proper fitting of the ergometer (Monark ergomedic, E839, USA) for each participant, a 3 min warm-up was performed at 50 watts (W). Immediately after the warm-up, work rate was increased by 40 W every 2 min until volitional exhaustion. During the tests subjects cycled at a rate of 90 rpm. The test was terminated when subjects were no longer able to keep the pedaling rate of 90 rpm, heart rate was close to age predicated maximal values, or a rating of perceived exertion (RPE) of 20 was reached. Wmax was calculated according to the equation presented by Kuipers et al. [27]. After exhaustion, the test continued for 3 min at a low work rate (30 W) as a cool down. Heart rate was regularly measured and monitored throughout the test.
HIIE protocols
After an eight-hour overnight fasting, all participants arrived to the laboratory between 08 : 00–09 : 00. Upon their arrival, participants were asked to rest in a seated position for 20 min during which heart rate and blood pressure were measured and a blood sample was taken. Thereafter, participants were asked to complete a warm-up at 40 W for 3 min, which was followed by an HIIE protocol. All participants performed two different HIIE protocols on two different occasions as described previously. The first protocol consisted of 6 intervals of 30 s work at 110% of PPO interspersed by 3 : 30 min of active recovery at 40% of PPO (protocol with work to rest ratio of 1/7, HIIE1/7). The second session involved 6 intervals of 2 min work at 85% of PPO interspersed by 2 min active recovery at 30% of PPO (protocol with work to rest ratio of 1/1, HIIE1/1). The second blood sample was taken immediately after exercise in seated position. All sessions were supervised by an exercise physiologist and environmental conditions including ambient temperature (25±2%), humidity (34±2%) and time of the day (08 : 00–09 : 00) were constant for both HIIE sessions.
Blood sampling and laboratory methods
Blood samples (6 ml) were taken from an antecubital vein, before and immediately after exercise. They were collected in tubes containing either Ethylenediaminetetra-acetic acid (EDTA, BD Vacutainer 7.2 mg K2EDTA, 4.0 mL, Becton Dickinson & Company, Plymouth, UK) or sodium citrate (Coagulation Sodium Citrate 3.2%, Greiner Bio-One GmbH, Frickenhausen, Germany). The whole blood anti-coagulated with EDTA was used to measure platelet indices including platelet count (PLT), plateletcrit (PCT), mean platelet volume (MPV) and platelet distribution width (PDW) by using a blood cell counter (XP-300, Sysmex, US). The tube contained sodium citrate was used to measure platelet aggregation [28]. For platelet aggregation tests, platelet-rich plasma (PRP) was obtained after centrifugation at 900 g for 8 min at room temperature and platelet-poor plasma (PPP) was prepared after centrifugation at 3000 g for 15 min at room temperature. The number of platelets in the PRP sample were counted, and if the number of platelets exceeded 275×103, samples were normalized through PPP [29, 30]. PRP was used to measure platelet aggregation using a four-channel platelet aggregometer (APACT 4004, Ahrensburg, Germany). Platelet aggregation was initiated with the addition of ADP (5 mM).
Statistical analyses
All data were analyzed by using a statistical package for social sciences (SPSS) version 22. Data were assessed for normality using the Shapiro-Wilk test. Repeated measures of ANOVA (2 protocols×2 times) were employed to compare the responses of all variables to both protocols. The significant value was set at P < 0.05. All data are presented as mean±SD.
Results
Platelet count increased significantly (F1,8 = 55.55, P = 0.001) in response to both HIIE trials (Fig. 1A & 1B). The increase in platelet count was higher during the HIIE1/1 than during the HIIE1/7 protocol (+21.1% vs + 10.3%, respectively; F1,8 = 5.76, P = 0.04). The other platelet’s indices including PCT (F1,9 = 25.7, P = 0.0.001), MPV (F1,9 = 14.3, P = 0.004), and PDW (F1,9 = 16.8, P = 0.003) increased following the two HIIE protocols (Table 1), but no significant difference was observed between the two trials (P > 0.05). Platelet aggregation induced by ADP increased significantly (F1,7 = 20.1, P = 0.003) from 70.7±7.9 to 80.9±5.6 and from 72.0±7.6 to 78.9±7.3, following HIIE1/1 and HIIE1/7, respectively (Fig. 2A & 2B); but we found no significant difference between the two HIIE protocols.

Mean (±SD) values of PLT before and immediately after HIIE1/1 (A) and HIIE1/7 (B). *indicates a significant (P < 0.05) effect of HIIE.
Mean values (±SD) of platelet indices before (Pre) and after (post) both HIIE protocols
*Indicates significant exercise effect. PCT, plateletcrit; MPV, mean platelet volume and PDW, platelet distribution width.
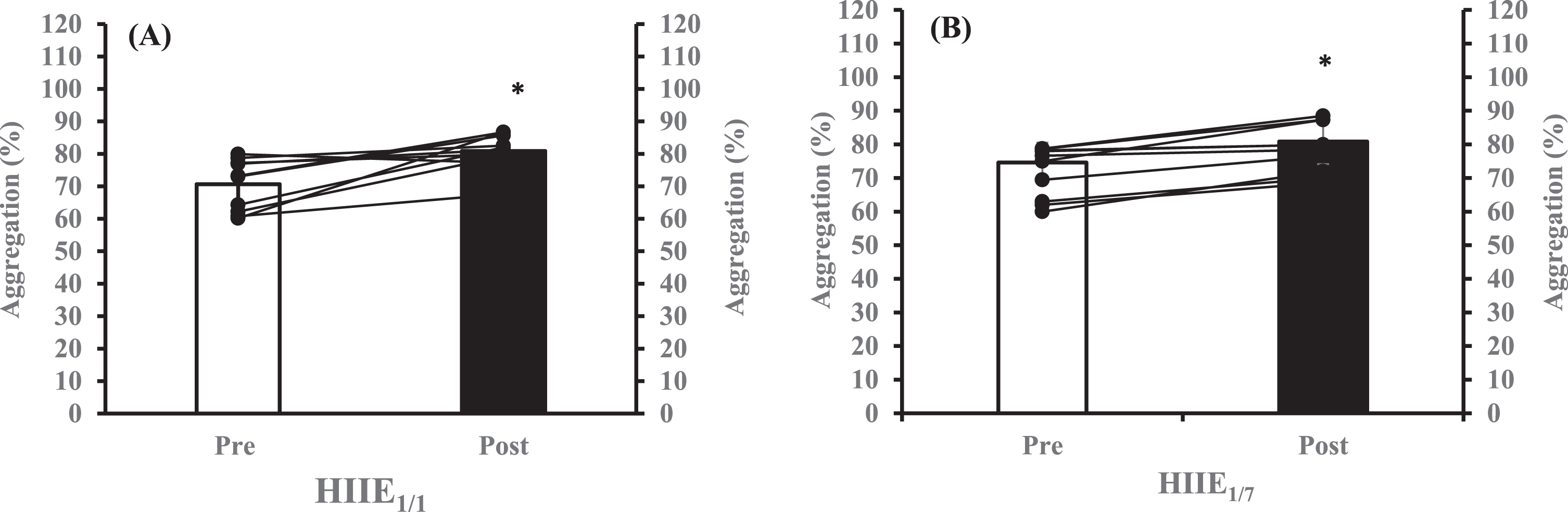
Mean (±SD) values of platelet aggregation before and immediately after HIIE1/1 (A) and HIIE1/7 (B). *indicates a significant (P < 0.05) effect of HIIE.
The main findings of the present study were that all platelet indices and platelet aggregation increased following HIIE and the magnitude of changes in PLT count was dependent on the work to rest ratio.
In the present study, regardless of the type of exercise protocol, HIIE increased platelet count by nearly 30%. Although few studies have reported no changes in PLT after exercise [31, 32], the majority of studies have shown an increase in PLT immediately after different exercise protocols [1, 33]. Meanwhile, Ahmadizad et al. found that a single session of HIIE increases PLT more than continuous exercise [23]. One of the main mechanisms responsible for exercise-induced thrombocytosis (platelet increase) is exercise-induced increases in sympathetic nervous system activity mediated by increased circulating catecholamine concentrations, which induce spleen contraction and as a result platelet secretion [16]. Therefore, the majority of the thrombocytosis could be related to the release of young platelets from spleen rather than fragmentation of megakaryocytes. In addition, it has been shown that catecholamine responses to exercise are intensity related [34, 35]. However, in the present study PLT increased more in response to HIIE1/1 (i.e., lowest intensity) than during HIIE1/7 (i.e., highest intensity). This finding could be explained by the fact that 1) the intensity for HIIE1/1 (85% of PPO) can still be considered high, and 2) the ratio of work to rest for HIIE1/1 is higher than the HIIE1/7, which might lead to more physiological stress and as a result more catecholamine production. In accordance to PLT and in line with previous studies [36, 37], plateletcrit rose by 18–21% following both HIIE trials, though, these increases were not different between the two HIIE protocols.
MPV and PDW were increased after the two exercise trials by 3–6% and 5.5–8.5%, respectively. The increases in MPV following HIIE demonstrate that the increases in PLT reported in our study might be related either to exercise-induced fresh release of large platelets from spleen or exercise-induced increases in the volume of circulating platelets. Moreover, MPV is considered as platelets activity index [38] and its increase in patients with coronary artery disease (CAD) is associated with higher incidence of myocardial infarction [39]. In our study, although non-significant the magnitude of MPV increase following HIIE1/1 (+6%) was twice the one observed after HIIE1/7 (+3%). This larger increase could be severe enough to put the individuals at greater risk for cardiovascular events, because it is higher than the within-subject variation (4.3%) reported for this variable [40], and the values (10.93±0.9 fL) reached the high-risk level (9.5 fL) reported by others [41].
Platelet aggregation rose in response to both HIIE protocols (8.5 and 18.5% for HIIE1/7 and HIIE1/1, respectively). There is a consensus in the literature regarding the vigorous exercise-induced increases in platelet aggregation [3, 10]. The increases in platelet aggregation found in our study could be justified by the intensity of the two HIIE protocols, which both were high (85 and 110% of PPO). These findings confirm those of Wang (2004) and Hilberg et al. (2008) who reported platelet aggregation increases following exercise in an intensity related manner [29, 42]. The exercise-induced increases in platelet aggregation are multifactorial, and could be explained by different mechanisms including the increases in blood flow related shear stress with intense exercise [29], epinephrine concentrations that stimulate the release of vWF from endothelial cells [43], and activation of platelet α2-adrenergic receptors [44], that all lead to enhanced shear-induced platelet aggregation. Furthermore, increased platelet aggregation might be potentiated by the changes in PLT and MPV values, because there is a positive correlation between MPV and platelet aggregation. In addition, our findings support studies that demonstrate increased platelet reactivity with aerobic interval exercise [45] and increased platelet function following an HIIE protocol [23].
The current study has practical implications regarding the prescription of high intensity interval training in overweight individuals, especially when designed for prevention and treatments of cardiovascular disorders. The results indicate that HIIE protocol with higher intensity and longer rest periods (1/7) is a safer protocol than the HIIE with lower intensity and shorter rest periods (1/1), because the thrombocytosis (increases in platelet count) was higher following the HIIE with the higher work to rest ratio (1/1), which might be the result of higher physiological stress. Therefore, it is suggested that practitioners consider the work to rest ratio as an important exercise variable when prescribing HIIE.
In conclusion, we showed that 1) high intensity interval exercise leads to transient increases in thrombocytosis and markers of thrombus formation (platelet aggregation), and 2) the intensity of exercise is not the only important exercise variable when considering the responses of thrombocytosis to HIIE. The physiological stress characterized by the aggregate effects of intensity, duration and work to rest ratio should be considered to justify the changes in thrombocytosis, but not the changes in platelet aggregation.
Footnotes
Acknowledgments
The authors wish to thank volunteers for their enthusiastic participation in this study and to thank Dr. Mark Rakobowchuk for proofreading the manuscript.