
Abstract
BACKGROUND:
Dehydration occurs frequently in older patients and constitutes a significant clinical problem.
OBJECTIVE:
This proof-of-concept study examines whether 1) sublingual measurement in dehydrated old patients is feasible, 2) frailty and incompliance in old, awake patients affects video-quality, 3) dehydration impacts microcirculation
METHODS:
This prospective observational study included clinically dehydrated patients aged ≥65 years immediately after admission. Dehydration was assessed clinically. A sidestream dark field camera (SDF) was used for measurement. Video-quality was evaluated with MIQS (microcirculation image quality score). Both AVA 4.3C- and AVA POEM-software analyzed the videos. Seventeen patients ≥65 years not showing dehydration served as control.
RESULTS:
Thirteen patients (8 female) were included. The average age was 83±8 years. The mini-mental test was 17±15 points, the Clinical Frailty Scale 4±3, the Barthel-Index 59±39. None of these parameters correlated with MIQS (3.4±4.2 SD (“acceptable”)). Dehydrated patients had a slightly impaired microcirculation, with a significantly lower percentage of perfused small vessels compared to control (83.1±7.7% versus 88.0±6.0%, P < 0.05). After rehydration, there was acute improvement in the microcirculation.
CONCLUSIONS:
Sublingual microcirculatory SDF-measurement is both, safe and valid for dehydrated old patients - regardless of frailty, age or cognitive performance. Dehydration leads to an impaired microcirculation.
Introduction
The world population older than 60 years will approximately increase from 12 % in 2013 up to 21 % in 2050 [1]. Dehydration affects one-third of these older adults causing electrolyte imbalances and is associated with adverse outcomes [2–4]. The problem might be aggravated by a rising occurrence of heatwaves due to climate change. Thus, the incidence of dehydration in older people is likely to increase possibly resulting in higher mortality rates [5]. There is a variety of reasonable explanations for the increased incidence of dehydration with a growing subject age. Thus, aging contributes to changes in the total body water, a decreased thirst perception [6], a decreased renal concentrating ability with reduced effectiveness of vasopressin [7]. In consequence, dehydration contributes to several end-organ damage syndromes such as delirium, acute kidney injury or cardiac arrhythmia [8]. In healthy adults, dehydration impairs sublingual microcirculation [9]. Dehydration alters the function both of blood and tissue cells [10, 11].
There is growing evidence that an exaggerated fluid balance negatively affects outcomes comparable to hypovolemia (e.g., in septic patients [12]). The correct identification of patients requiring fluids on the one hand and the avoidance of iatrogenic hypervolemia is a persisting challenge in clinical management [13]. Since sublingual intravital sidestream darkfield microscopy (SDF) has been introduced in clinical practice, microcirculation has become a directly detectable physiological compartment reliably reflecting organ perfusion [14–17]. The method is non-invasive and enables one to quantify both, blood flow and vessel density with a diameter of less than 100μm, and in particular, of those being smaller than 20μm (mostly capillaries). These vessels are of key importance for tissue oxygen supply [18, 19]. Contrary to serum lactate as a late marker of impaired tissue oxygenation, sublingual microcirculation might earlier detect impaired tissue perfusion [20, 21]. The last generation of microcirculation assessment tools are easy to use hand-held devices providing microcirculatory parameters, which can be directly used for clinical interpretation. Therefore, with the introduction of hand-held devices, it is possible to monitor microcirculation at the bedside. These observations are not only of scientific interest but might also impact clinical decision making. Thus, measuring sublingual microcirculation can be used to identify high-risk patients in both, in septic and cardiogenic shock [22, 23], chronic heart failure [24], in coronary artery disease [25] and to predict outcome after cardiac arrest [26–29]. However, until now, there is lacking evidence about the efficacy of therapeutic interventions on microcirculation [30, 31] and the majority of investigations were performed in intensive care patients or healthy volunteers.
We hypothesize that microcirculatory impairment caused by dehydration is measurable even in a cohort of older patients with sufficient video-quality. Furthermore, it is hypothesized that fluid resuscitation results in improved microcirculatory values.
This study assesses the feasibility and clinical value of sublingual microcirculation measurement in dehydrated elderly patients.
Methods
Ethics
A cohort of patients and volunteers was analyzed prospectively. The study was approved by the German Ethics Committee of the Medical Faculty of the University Hospital Duesseldorf, Germany (Date of approval: April 22th, 2016; (Study No.: 5447R; Registry No.: 2016024919). Since we aimed to perform a proof-of-concept study, no sample size calculation was mandatory. The study was conducted at the University Hospital of Duesseldorf. Recruitment began in June and ended in October 2019.
Data recording
Medical history, clinical data, and standard laboratory parameters have been documented. Mortality data were collected by review of medical records in the in-hospital patient data management system (COPRA System GmbH, Berlin, Germany) and/or by patient contact. Patient’s data were collected prospectively in the patient data management system. All patient’s data were anonymized.
Inclusion criteria
For inclusion in the study, the following criteria had to be fulfilled: 1) 65 years old or older, 2) diagnosed with dehydration according to the clinical impression of the treating physician, 3) informed consent, 4) the sublingual mucosa had to be accessible. The clinical diagnosis of dehydration was made by the primary treating physicians, who were not part of the study team. Typical clinical signs were standing skin folds, dried mucous membranes, and a visually reduced, highly concentrated urine. Patients who underwent cardiopulmonary resuscitation where excluded from the study. Additionally, seventeen non-dehydrated patients, who were 65 years or older received SDF-measurement.
Quality control
Before analysis, all videos were rated according to the microcirculation image quality score [32] into three categories: “good”, “acceptable”, and “non-acceptable”. In brief, six different criteria were evaluated: Illumination, duration, focus, content, stability, and pressure. A video without significant impairment in all criteria received zero points. Mild impairment resulted in 1 point for each impaired criterion. Severe impairment in one criterion was defined to be rated with 10 points, which results in the category “non-acceptable”.
SDF-measurement and automatic video-analysis
The microcirculation was assessed by the implementation of the sidestream darkfield microscope (MicroScan® device, Microvision Medical, Amsterdam, The Netherlands) as described before [33]. A highly sensitive camera digitally recording the sublingual capillary network at the tip of the device. Videos were acquired in different regions under the tongue. Depending on the patient’s collaboration, at least four videos were taken per area. For video analysis, a suitable tablet computer was used (Microsoft Surface Pro 4, (Redmond, Washington, USA)). The software-based video-analysis can be carried out in real-time or offline at later time points using saved video files. After the acquisition of the videos, a validated automatic algorithm-software (AVA, Version 4.3 C) performed the analysis. Microvascular values provide information about both, convexity and diffusion capacities [34]: Total vessel density (TVD, total number of vessel crossings) and the number of crossing (NC, number of vessels intersections the lines in a grid of 3 equidistant horizontal and vertical lines) give information about diffusion and reflect the vascular density. The percentage of perfused vessels (PPV) offers information both about convexity and perfusion [35]. PPV was calculated after measuring the proportion of perfused vessels (PPV = 100 * (Total number of perfused vessels/total number of vessels). Both vessel density and perfusion can be combined for perfused vessel density (PVD = total length of perfused vessels divided by the analyzed area) and perfused number of crossings (PNC = number of vessel crossings with continuous flow). The values for all vessels can be considered as a quality check to exclude for example pressure artefacts [36]. Vessels with diameters less than 20 mm usually correspond to capillaries that are primarily responsible for the microcirculation. The small vessel values are marked by the prefix “s” (e.g. sPPV = PPV of small vessels). This algorithm is in line with the second consensus on the assessment of sublingual microcirculation in critically ill patients (European Society of Intensive Care Medicine) [37].
POEM-Score
Recently, Naumann et al. developed and validated a point-of-care-tool for the manual assessment of microcirculation [38]. This score (POEM-Score, point of care microcirculation) bases on the composite assessment of flow and heterogeneity and results in an ordinal scale from 1 (worst) to 5 (best).
Cognitive impairment, nursing status, and frailty
The cognitive and nursing status of the patients before hospital admission was assessed using different scores. The standardized Mini-Mental-Test [39] is a screening tool for cognitive impairment. The test was performed directly before SDF-measurement. The best possible result is 30 points, the worst 0 points. Test results up to 24 points can be considered normal [40]. Nursing status was estimated by the Barthel-Index [41] ranging from 100 points (“normal and autonomous”) to 0 points (“completely depending on nursing”). Frailty is a syndrome that includes an age-associated loss of physical and cognitive reserves, as well as reduced compensatory mechanisms to stress with an augmented susceptibility to many adverse clinical outcomes [42]. The Clinical Frailty Scale (CFS) is a simple model visually describing patients physical conditions with nine classes from very fit (class 1) to terminally ill (class 9). CFS is most widely used in intensive care [43] and is independently associated with higher hospital mortality, long-term mortality and morbidity [44–46]. Barthel-Index and CFS were referred to the situation four weeks before hospital admission, Mini-Mental-Test on the day of admission.
Follow-up
For follow up, clinical data were taken from medical records in the in-hospital patient data management system and/or by patient contact. In detail, the length of stay and in-hospital-mortality was assessed.
Statistics
Analyses were performed with Microsoft® Excel 2010 for Windows, the IBM Statistical Package for the Social Sciences (SPSS) 23.0 for Windows and Graph Pad Prism (Graph Pad Prism Software, Version 5, Graph Pad Software, San Diego, California, USA). The data were checked for normal distribution by the Shapiro-Wilk test. Normally distributed data are given in mean±standard deviation, non-normally distributed data are shown as median with inter-quartile-range. Categorical data are expressed as numbers (percentage). In this regard, the statistical tests applied were the Mann Whitney test and the t-test, respectively. For paired groups and non-normally distributed data, the Wilcoxon signed-rank test was used. A 2-tailed p-value <0.05 was considered statistically significant. For correlation analysis, Spearman-Rho was used for ordinal and Pearson for metric values.
Results
Patients’ characteristics
Thirteen patients (8 female, mean age of 83 years±5.5 years, minimum 66, maximum 96) who were admitted to the Emergency Department or Chest Pain Unit of the University Hospital of Duesseldorf between June 2019 and October 2019 were eligible for the study (see Fig. 1). The initial lactate was 1.5±0.5 mmol/L. Vital parameters were inconspicuous (Table 1). The most frequent comorbidities were preexisting chronic kidney disease (30.8%), Diabetes mellitus (23.1%), chronic heart failure (15.4%), active smoking (15.4%) and chronic obstructive pulmonary disease (7%).

Study Flow Diagram for patient inclusion. Patients who were 65 years or older and who had a clear diagnose of dehydration according to the clinical impression of the treating physician were eligible for enrollment in the study. Patients without an accessible sublingual mucosa or lacking informed consent were excluded.
Patients’ characteristics (Mean±SD for normally distributed values, Median with Interquartilrange for not normal distributed values), (n = 13)
Dehydration can influence sodium-hemostasis, osmolality and kidney function. Osmolality was calculated as follows: 2×Sodium (mmol/l) + Glucose (mmol/l) + Urea (mmol/l). In this cohort, there were no significant pathological values (Table 2).
Laboratory values of dehydrated patients (n = 13)
The results regarding the cognitive impairment, nursing, and frailty in the investigated cohort were heterogeneous: Mini-Mental-Test results had a mean value of 15 points (±13) and ranged between a maximum of 30 and a minimum of 0 points. Results for the Barthel-Index were similar, having a mean of 53 points (±40 points, minimum 0, maximum 90). Finally, the mean clinical frailty scale was 5 (±3 minimum 1, maximum 8, Fig. 2).
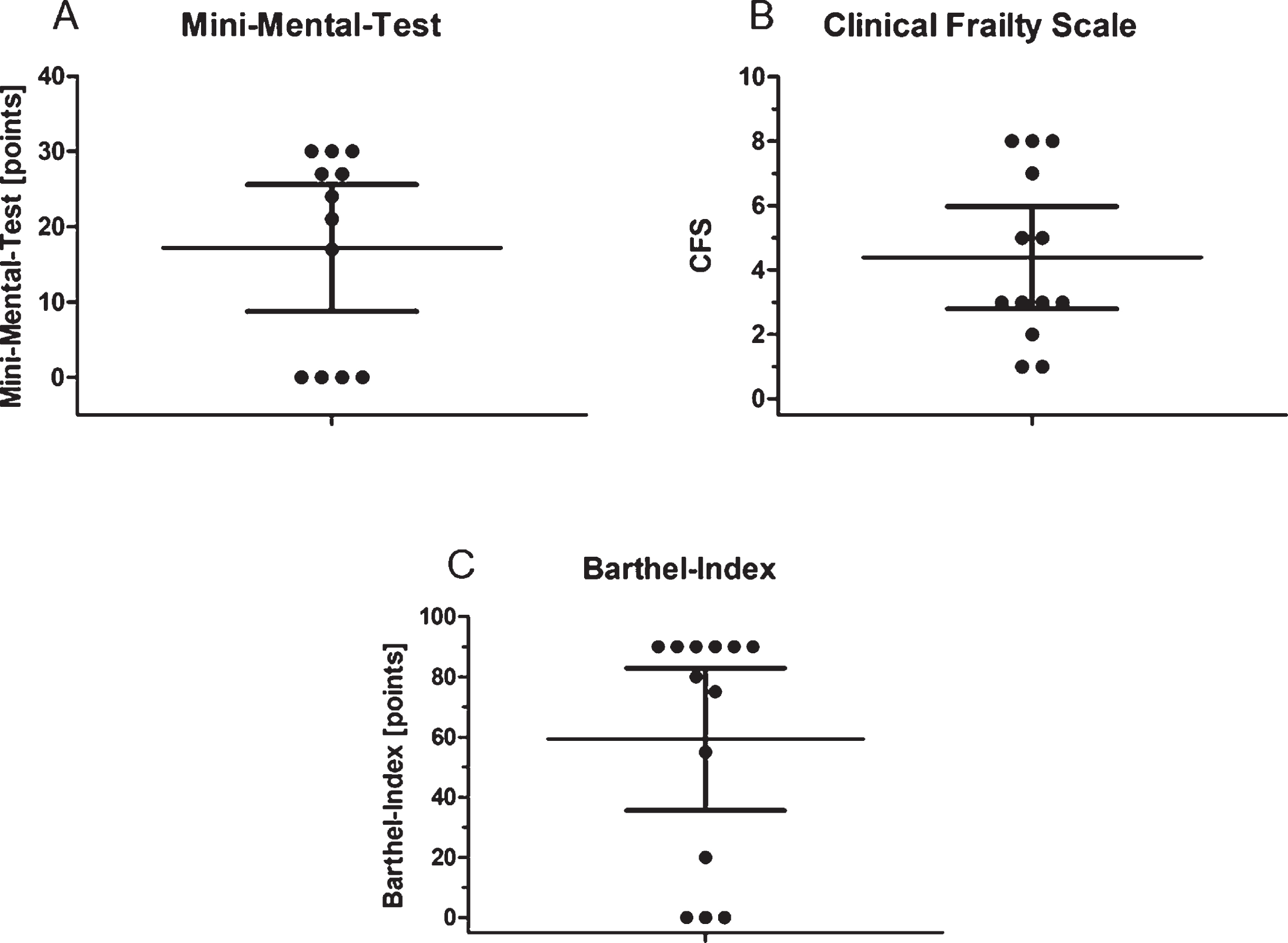
Cognitive function, nursing status and frailty. Mean with 95% -CI. (A) Mini-Mental-Test. (B) Clinical frailty scale. (C) Barthel-Index. A point represents the mean value of each patient for each time point. The horizontal line through the center of each group represents the mean with 95% -CI (horizontal bar of the top and the bottom of each group).
On average, it took 02 : 24±01 : 08 minutes for the SDF camera and software to be ready for use, when the camera was connected and the tablet was on “standby”. 04 : 26±02 : 23 minutes (Minimum 1 minute, Maximum 10 minutes) were necessary for the recording of a sufficient amount of acceptable video quality, and 04 : 08±00 : 22 minutes (Minimum 03 : 51 minutes, Maximum 05 : 00 minutes) for software to automatically evaluate a video. On average, 9±4 videos (Minimum 2, Maximum 10) were recorded per patient. Only in one patient, it was impossible to capture at least four videos. No complications regarding the microscope or the sublingual measurement had been reported.
The impact of cognitive impairment on quality scores and sublingual microcirculation
No correlation between the quality score and different assessment scores for cognitive impairment could be observed. In particular, a low Mini-Mental-Score did not affect MIQS. With the exception of sPPV, none of the microcirculatory parameters correlated with the clinical scores (Mini-Mental-Test, CFS, Barthel-Index). sPPV had a highly significant negative correlation with the Mini-Mental-Test (Correlation according to Spearman-Rho -0.812 Significance (2-sided) P = 0.001), the Barthel-Index (Correlation according to Spearman-Rho -0.657 Significance (2-sided) P = 0.015) and a highly positive correlation with the Clinical Frailty Scale (Correlation according to Spearman-Rho 0.708 Significance (2-sided) P = 0.007).
Microcirculation in dehydrated old patients in comparison to non-dehydrated old patients
All microcirculatory parameters for small vessels demonstrated high correlations with each other (Correlation according to Pearson p < 0.01 for sTVD, sPVD, sPNC, sNC; P < 0.05 for sPPV). Dehydration resulted in impaired microcirculatory values (sNC 15.4±9.0/mm², sTVD 3.3±1.9 cpll/mm², sPNC 12.0±6.7, sPVD 2.6±1.4 mm/mm², sPPV 83.1±8.0%). In comparison, non-dehydrated patients had a trend towards better microcirculatory values (sNC 17.7±7.6/mm², sTVD 3.8±1.6 cpll/mm², sPNC 15.1±6.3, sPVD 3.2±1.3 mm/mm²) with a statistically significant higher sPPV in the control group (88.9±6.2%; see Fig. 3). Patients in the control group were younger (83±8 years in the dehydrated group versus 77±9 years, P < 0.05) with similar distribution of sex (38% male versus 41% respectively).
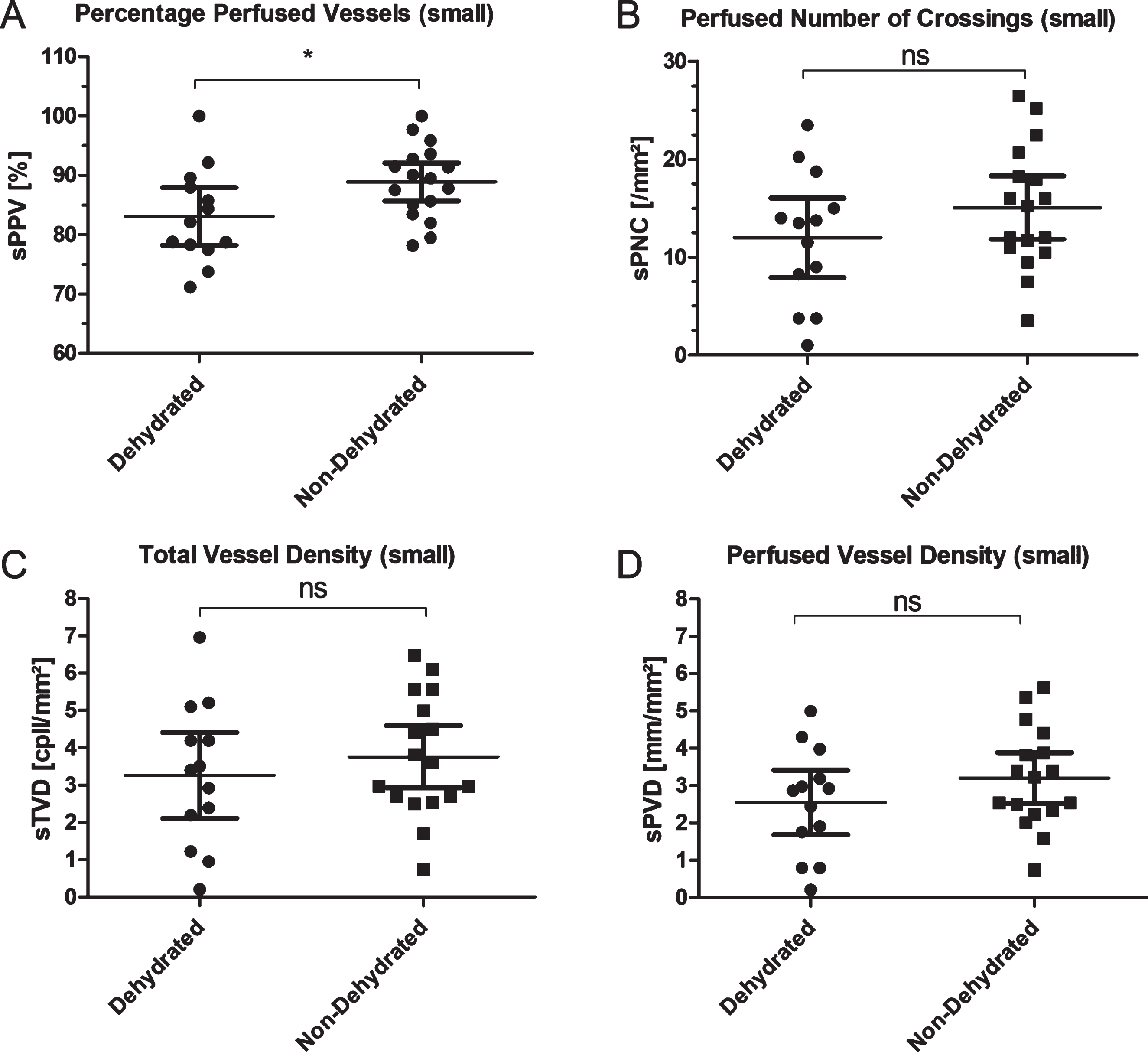
Microcirculatory parameters comparing dehydrated and non-dehydrated patients. (A) Percentage of Perfused small Vessels. (B) Perfused Number of Crossing of small Vessels. (C) Total small Vessel Density. (D) Perfused small Vessel Density. A point represents the mean value of each patient for each time point. The horizontal line through the center of each group represents the mean with 95% -CI (horizontal bar of the top and the bottom of each group). (n = 13 for dehydrated patients, n = 17 for non-dehydrated patients). *=P < 0.05, ns = P≥0.05.
Before rehydration, microcirculatory values were impaired, but in an early control after four hours, none of the measured parameters showed a significant change compared to admission (sNC 16.6±9.1/mm² versus 17.9±8.2/mm² p = 0.652, sTVD 3.5±1.9 cpll/mm² versus 3.8±1.7 cpll/mm² p = 1.0, sPNC 12.8±6.5 versus 14.2±6.1 p = 0.906, sPVD 2.7±1.4 mm/mm² versus 3.0±1.3 mm/mm² p = 0.96, sPPV 81.8±9.2% versus 83.5±10.2% p = 0.91, see Fig. 4). In the detailed analysis, in some patients, there was an improved microcirculation after four hours, but in some, there was even an impairment. A trend showing remarkable microcirculatory improvements mostly in patients that were impaired on admission could be shown, while patients with higher values did not profit in this early re-assessment.

Microcirculatory parameters comparing dehydrated patients ad admission and early changes four hours after rehydration. (A) Percentage of Perfused small Vessels. (B) Perfused Number of Crossing of small Vessels. (C) Total small Vessel Density. (D) Perfused small Vessel Density. A point represents the mean value of each patient for each time point. The connecting lines indicate connected samples. (n = 9). ns = P≥0.05.
In the next step, data about the amount of fluids administered in the emergency department within the first four hours was collected. The only used fluid was Jonosteril®, a balanced full electrolyte solution. The mean dosage was 555±726 ml per patient. To investigate the relationship between the amount of administered fluid and the changes in the measured microcirculation after four hours, Δ sPPV (sPPV after 4 hours –sPPV at admission) was calculated. However, there was no correlation between Δ sPPV and the administered fluid (Correlation according to Pearson –0.320 Significance (2-sided) 0.401).
There was no significant difference between dehydrated and non-dehydrated patients in the POEM-Score (Mann Whitney test P = 0.0892, see Fig. 5). No correlation could be found between the results that were calculated by AVA 4.3C and those that were assigned manually using AVA-POEM-BETA (Spearman-Rho >0.05).
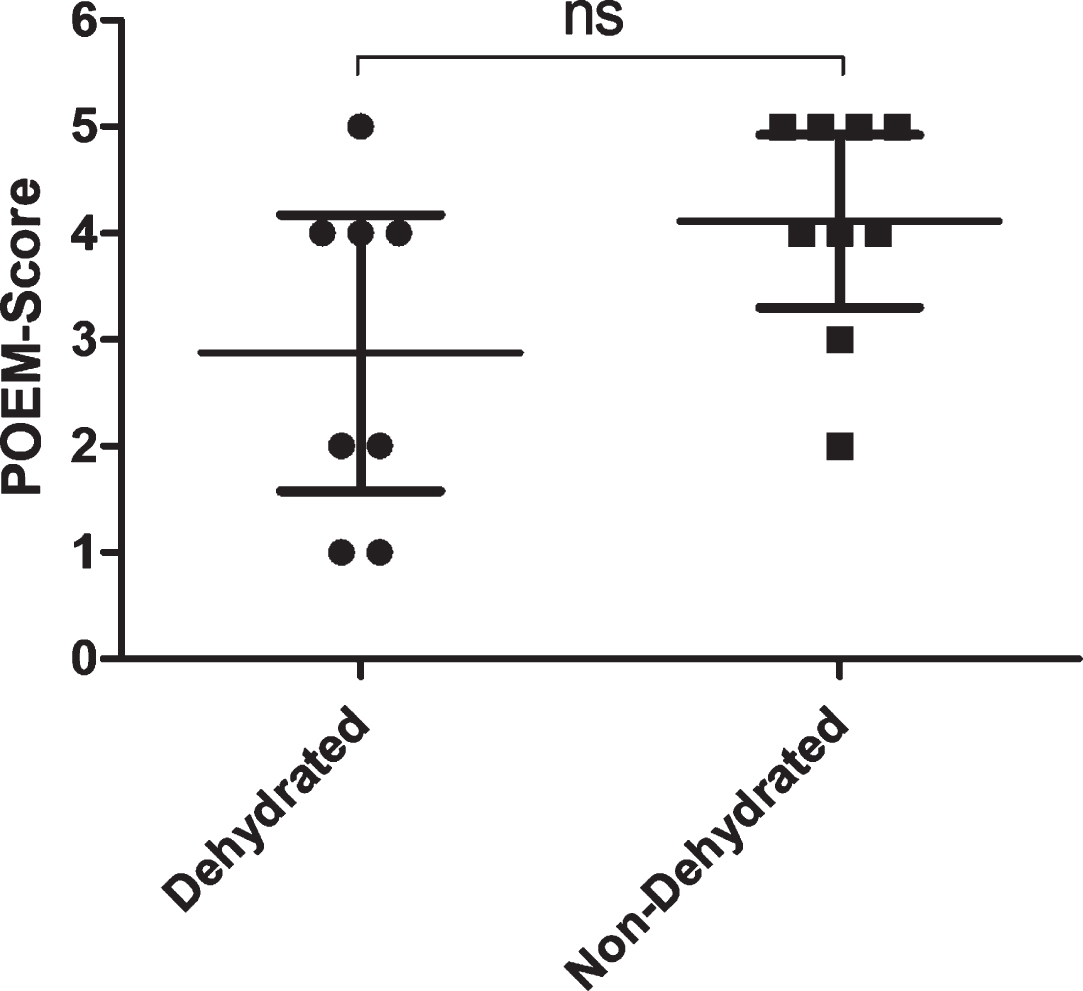
Application of AVA POEM BETA. A point represents the POEM-Score value of each patient. The horizontal line through the center of each group represents the mean with 95% -CI (horizontal bar of the top and the bottom of each group) n = 8. ns = P≥0.05.
No correlation between microcirculatory parameters at admission and length of stay could be found (e.g. for sPPV no correlation according to Pearson –0.136, Significance (2-sided) 0.658). Hospital mortality was 0%.
Discussion
In daily clinical routine, dehydration in elderly patients occurs frequently. It represents a well-known trigger for a variety of disease states such as atrial fibrillation [8] or delirium [47]. Thus, the phenomenon constitutes a significant economic burden since it leads to avoidable hospitalizations [48, 49]. Despite this discovery, the majority of studies available in the literature dealing with dehydration were conducted in children [50], investigated drug-associated fluid loss (e.g. empagliflozin [51] or tolvaptan [52]) or were focused on dehydration in diabetes mellitus [53]. Dehydration in nursing homes is a chronic and current problem [54]. However, only very few data exist about the old patient who is admitted to the emergency department with clinically manifest dehydration. In this acute setting, decision-making is often time-critical. This problem is aggravated by the fact that old dehydrated patients are often only partially oriented and not cooperative. In this study, cognitive impairment, nursing or frailty did not impair video-quality of sublingual intravital sidestream darkfield microscopy; this technology is both feasible and safe in dehydrated old patients.
The patients included in our current study demonstrated a significantly impaired microcirculation as assessed by the percentage of perfused vessels compared to non-dehydrated elderly patients. It is important to underline that the control group did not represent healthy volunteers, but patients suffering from chronic disorders such as heart failure, but without clinical signs of dehydration. This might explain the relatively impaired microcirculation observed in the control group when compared to reports from the literature. Another fact possibly explaining the marginal difference is chronic malnutrition, which frequently occurs in the elderly and might adapt to this chronic lack of fluids. In contrast, dehydrated children or younger patients suffering from, e.g., acute gastroenteritis exhibit an acute disease state. In contrast, the patients investigated by us were not critically ill reflected by both, the low lactate value and the minimal length of stay and in-hospital mortality in the cohort. On the other hand, elderly patients with chronic cognitive impairment are in particular susceptible to abnormalities of their electrolyte and body water homeostasis [55]. The used definition of dehydration might also explain some findings of this study: For inclusion, the clinical impression (dry tongue mucous membrane, reduced skin turgor) was sufficient. The commonly used definition of dehydration is a loss of body water to a greater extent than the body can replace. Two types of dehydration can be distinguished: a water loss dehydration (hyperosmolar, due either to increased sodium or glucose, mostly hypernatremia) and a combined salt and water loss dehydration (hyponatremia) [56]. Therefore, severe dehydration should always affect intravasal osmolality with sodium-disorders (both hyper- and hyponatremia) [57] or impaired kidney function. In fact, serum osmolality is considered the gold standard for the diagnosis of water-loss dehydration [58]. In this study, six of 13 patients had an initial osmolality higher than 295 mosmol/kg (cut-off value for dehydration [59]). In the investigated cohort, no relevant disturbs in the sodium homeostasis could be observed. A few patients suffered from acute impairment of kidney function. Of note, creatinine and urea as markers for dehydration in old patients are often of limited value, because they may be biased by a catabolic state (sepsis, glucocorticoids), sarcopenia, heart, and renal failure. In sum, the present data indicate, that the clinical judgment is not sufficient to diagnose relevant dehydration in old patients. This is in line with current evidence. Fortes et al. demonstrated, that apart from low systolic blood pressure, all physical signs offer only little utility for recognizing dehydration in old patients [60]. Further studies should use stricter criteria to rule in dehydrated patients.
Another important topic was to enlighten the role of fluid restoration. The correct fluid management remains controversial, both in emergency and intensive care medicine. In a perioperative setting, sublingual intravital sidestream darkfield microscopy has been used for periinterventional management of blood transfusions [61] and fluids [62]. In this study, the impact of fluid administration was exclusively investigated after four hours and did not result in a significantly improved microcirculation. Nevertheless, there is a clear trend: Patients who initially had an impaired microcirculation developed an improved microcirculation even in this early re-assessment. In future studies, more follow-up measurements should be performed. It should be mentioned that less than half of the patients received parenteral fluids. However, it is questionable if there had been a clear indication for parenteral rehydration. In fact, in absence of instable hemodynamic variables, markers of tissue hypoperfusion such as elevated lactate, prolonged capillary refill time or skin mottling, there is no clear indication for parenteral fluid administration [63]. Future studies should investigate the role of SDF-measurement for fluid balancing.
Limitations
This investigation has some major limitations. The cohort was small and the inclusion criteria were liberal. Due to its design as explanatory proof-of-concept-study, no confirmatory target was defined. Further studies should recruit more patients and define stricter inclusion criteria.
Conclusion
This pilot study proofed that sublingual microcirculatory measurement is feasible and safe in dehydrated old patients regardless of their mental status. Dehydration correlated with impaired microcirculation. In sum, the assessment of sublingual microcirculation in acutely ill elderly patients was possible and safe.