
Abstract
BACKGROUND:
Post-therapeutic tissue is bradytrophic and thus has low perfusion values in PCT. In contrast, malignant tissue is expected to show higher perfusion values as cancer growth partially depends on angiogenesis.
OBJECTIVES:
This prospective study investigates perfusion computed tomography (PCT) for the post-therapeutic detection of cancer in the head and neck region.
METHODS:
85 patients underwent PCT for 1) initial work-up of head and neck cancer (HNC; n=22) or 2) for follow-up (n=63). Regions of interest (ROIs) were placed in confirmed tumour, a corresponding location of benign tissue, and reference tissue. Perfusion was calculated using a single input maximum slope algorithm. Statistical analysis was performed with the Mann-Whitney U-test.
RESULTS:
PCT allowed significant differentiation of malignant tissue from post-therapeutic tissue after treatment for HNC (p=0.018). Significance was even greater after normalization of perfusion values (p=0.007). PCT allowed highly significant differentiation of HNC from reference tissue (p<0.001).
CONCLUSIONS:
PCT provides significantly distinct perfusion values for malignant and benign as well as post-therapeutically altered tissue in the head and neck area, thus allowing differentiation of cancer from healthy tissue. Our results show that PCT in conjunction with a standard algorithm is a potentially powerful HNC diagnostic tool.
Keywords
Introduction
Head and neck cancer (HNC) is the sixth most common malignancy by incidence worldwide, with about 600,000 new cases each year and a five-year survival of about 40%. Accounting for 90% of all HNCs, squamous cell carcinoma (SCC) is the most common subtype, and patients with SCC often have locally advanced disease at the time of presentation [1, 2]. Tobacco and alcohol consumption are the most critical risk factors, with synergistic effects [3, 4]. Furthermore, sexually acquired infections with human papillomavirus (HPV) are an emerging cause, especially in HNC of the oropharyngeal subsite [1, 4].
Therapeutic decisions are, among others, determined by the tumour stage and subtype. While early-stage SCCs are generally treated surgically, patients presenting with advanced SCC are usually treated with a combination of surgery, radiotherapy and chemo- or immunotherapy [5, 6].
Computed tomography (CT) and magnetic resonance imaging (MRI) are routinely used for the diagnosis of HNC and accurate staging [7, 8]. However, based on signs in contrast-enhancement CT or MRI alone, it can be difficult to differentiate between cancer and surrounding inflammation or oedema. This may result in overestimation of the actual extent, thus contributing to false diagnostic information and suboptimal treatment [9–11]. HNC patients with unfavourable factors, such as large tumour extent, bone invasion or lymph node metastases especially with extracapsular extension (ECE) have a higher risk of cancer recurrence. Depending on these factors, patients may benefit from post-operative, adjuvant therapy such as radio- and/or chemotherapy [12, 13]. Radiotherapy commonly leads to scarring of the target tissue. This tissue is bradytrophic and precludes the early detection of recurrent cancer, though essential in the early post-therapeutic period.
The fact that angiogenesis is essential for tumour development and growth offers a promising approach for targeting post-therapeutic tissue [14]. As enhanced angiogenesis leads to the formation of more blood vessels, higher levels of perfusion in tumour tissues are given [15]. Perfusion can be measured and visualized by perfusion CT (PCT), which has recently attracted attention as a non-invasive technique for the assessment of pathological angiogenesis [16]. In general, PCT works by recording changes in x-ray attenuation in a predefined target area during the passage of a fast, intravenous bolus of iodinated contrast medium over time. This technique has been proven useful for imaging neoplasms in several organs including the prostate, colon, liver, and lungs [17–19] but also for the evaluation of patients with vascular diseases [20].
Studies investigating PCT in HNC have mainly focused on experimental protocols and algorithms, such as deconvolution and compartmental analysis [16, 21]. Overall, published data suggest that malignant tissue has an increased blood volume, blood flow and permeability surface area product but an increased mean transit time [9, 11]. The maximum slope algorithm used in this study is the most common and generally available algorithm.
The study presented here was conducted to investigate the clinical practicality of PCT in conjunction with a single input maximum slope algorithm in patients with head and neck cancer. We hypothesize that PCT can accurately differentiate malignant from healthy tissue in suspected HNC and also from therapeutically altered tissue at follow-up. We furthermore assume that perfusion values determined with PCT are more reliable if normalized to individual perfusion aspects.
Materials and methods
The institutional review board approved this study (board reference number: EA4/066/14). Patient informed consent was obtained.
Study population
A total of 110 patients who either presented for initial work-up of suspected HNC or were seen for routine follow-up at our outpatient department were considered for inclusion. Patients who underwent HNC for initial work-up were included if they had histopathologically proven HNC without extra--oral or dermal tumour manifestation. Additionally, full clinical, histological and radiological data had to be available for inclusion. Twenty-two patients with a diagnosis of HNC at initial work-up met the inclusion criteria, see flow chart in Fig. 1. The reference group included 63 patients who under-went routine follow-up PCT and were free of tumour. If no biopsy was obtained due to missing clini-cal or radiological evidence of a recurrent tumour, a bland follow-up period of at least 10 months was assured.
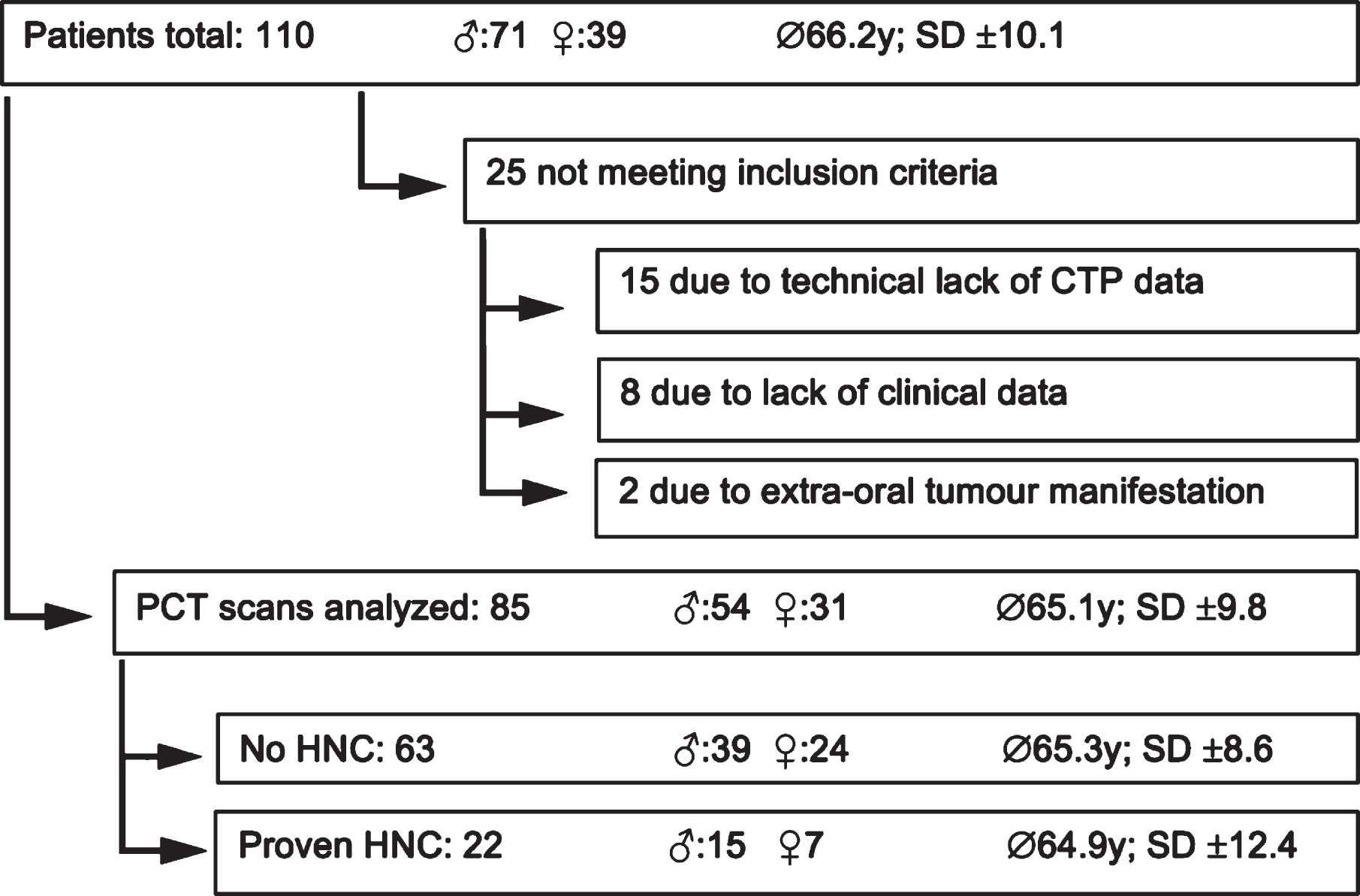
Flow chart of patient enrollment with exclusion criteria and demographic data.
Twenty-five patients did not meet the inclusion criteria and were excluded from analysis. Eighty-five patients could be comprehensively evaluated (31 females and 54 males; mean age 65.1 ± 9.8 years, minimum age 47, maximum age 94).
Among the 22 patients diagnosed with primary HNC, 21 had oropharyngeal SCC and one patient adenosquamous carcinoma of the nasopharynx. All HNC cases were confirmed histologically (Fig. 1).
The tumour localizations in the 22 patients diagnosed with primary HNC are presented in Table 1.
Distribution of tumour localizations at initial diagnosis
All CT examinations were performed on an 80-slice CT scanner (Aquilion PRIME, Canon Medical Systems, Otawara, Japan). To improve compliance and reduce motion artefacts, patients were informed about the different steps of the examination and the possible occurrence of a heat sensation. They were instructed to breathe quietly without swallowing during acquisition.
PCT scans were acquired with the following parameters: 200mA, 100kV, 0.35s/rotation, and 1 mm slice thickness. For perfusion imaging, 40ml Iomeprol with an iodine concentration of 400 mg/ml (Imeron 400, Bracco Imaging, Milan, Italy) were injected at a rate of 4ml/s.
Perfusion imaging was performed over a period of 120 sec, during which a total of 40 3D volumes were acquired and reconstructed with 1mm slice thickness and a spatial resolution of 512×512 pixels and a temporal resolution of 3 sec, resulting in a total of 5080 images per patient. To cover the entire anatomic target area, perfusion imaging was performed in shuttle mode with constant bidirectional table movement. The 3D volumes were then reconstructed using a FC11 convolution kernel.
CT image analysis
PCT analysis was performed using a dedicated research computer (Canon V6.3) that allows to register the images, ruling out image distortion caused by minimal motion (breathing/swallowing), and to precisely measure and evaluate perfusion maps. To quantify perfusion, two radiologists measured regions of interest (ROIs) in the tumour, in the external carotid artery, in site-matched benign tissue in follow-up PCT datasets and in ipsi- and contralateral nuchal muscle tissue, which was defined as reference. In placing the ROIs, the radiologists paid special attention to an adequate size and avoided air, surrounding fat and large vessels. ROIs were placed in anatomical images, which were automatically matched with functional perfusion images of corresponding locations see Fig. 2.
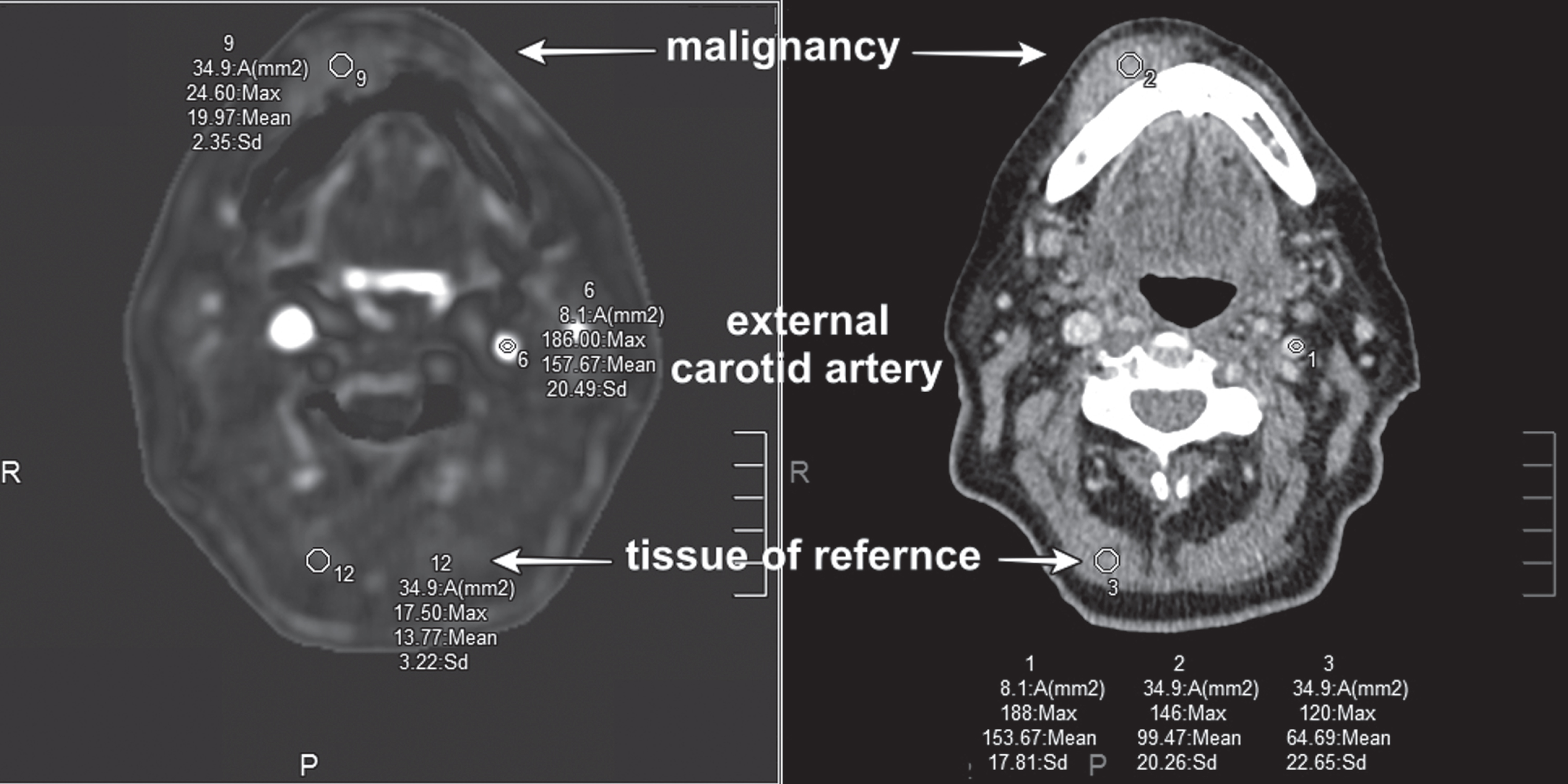
Placement of regions of interest (ROIs) in anatomic CT image and corresponding PCT map.
A standardized protocol was used to calculate perfusion values and arterial flow [22] see Fig. 3.
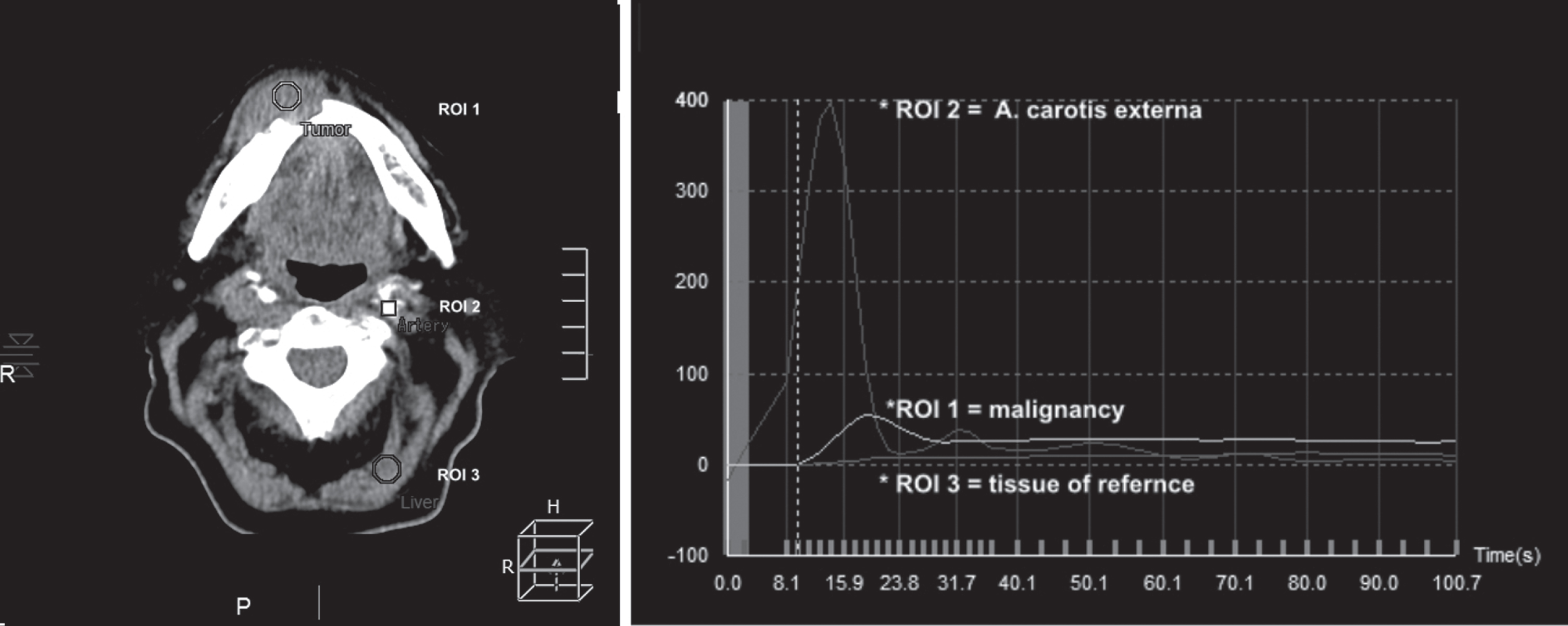
Regions of interest (ROIs) with corresponding arterial flow diagrams.
If indicated, perfusion values of pathological tissue and benign tissue were normalized to the values of their tissues of reference before comparative statistical analysis. Perfusion was calculated as follows:
perfusion tumour
perfusion benign
The normalized perfusion values were used in statistical analysis as described below.
Statistics
Statistical analysis was performed with SPSS Statistics 24 (IBM, USA). The Kolmogorow-Smirnow-Test was chosen to check for normal distribution. Data were not normally distributed so the Mann-Whitney-U-test was performed for the comparison of perfusion values of malignant and benign tissue and their reference tissues. Standard deviation (SD) was calculated as mean SD from primary data.
A p-value of<0.05 was considered statistically significant.
Results
The three main results of this study are summarized below.
Dynamic volume PCT allows differentiation of primary HNC from benign post-therapeutic tissue of corresponding locations
Without normalization
Without normalization of perfusion values to the respective reference tissues,malignant tissue perfusion in patients with primary HNC differs significantly from that of benign tissue in corresponding locations (p < 0.05) (Table 2).
Improved differentiation of primaryHNC tissue frombenign tissue by PCT with normalization
Malignant tissue perfusion in patients with primarily diagnosed HNC differs highly significantly from that of benign tissue after normalization of perfusion values to reference tissues (p < 0.01) (Table 3).
PCT allows highly significant differentiation of HNC from tissue of reference
Using the maximum slope algorithm, perfusion values in malignant tissue differ significantly from perfusion values of reference tissue (p < 0.001) (Table 4).
PCT yields similar perfusion values in different types of reference tissues –Data is comparable
Mean perfusion of primary HNC tissue compared to benign tissue without normalization
Mean perfusion of primary HNC tissue compared to benign tissue without normalization
Normalized mean perfusion of HNC tissue compared to benign tissue in corresponding locations
Mean perfusion of malignant tissue and reference tissue
Using the maximum slope algorithm, PCT-derived perfusion values in tissues of reference do not differ significantly between patients with HNC and those without HNC (follow-up) (p>0.05). PCTs of patients with confirmed HNC and no tumour in this study are comparable. Furthermore, perfusion values of reference tissues do not differ intra-individually between values measured ipsi- and contralaterally (Table 5).
Mean perfusion in different types of reference tissues in patients with and without HNC
This study in a large patient population shows that perfusion computed tomography yields perfusion values calculated with the generally available single input maximum slope algorithm that allow significant differentiation between HNC tissue, adjacent benign tissue and post-therapeutic changes. Furthermore, as tissue perfusion varies between individuals, the performance of PCT can be improved by intra-individual normalization of perfusion values to tissue of reference. To the best of our knowledge, little data is available on PCT of the head and neck region, and earlier studies mostly used a deconvolution algorithm [16, 21]. In our study we used the maximum slope algorithm, which is widely available by default with contrast-enhanced CT packages from most manufacturers and also on vendor-independent imaging platforms (i.e. Visage Imaging, San Diego, USA). Our experience suggests that PCT can easily be implemented and applied on a large scale.
In the routine clinical setting, it is often a challenging task to distinguish HNC from post-therapeutic changes, either after surgery with reconstruction using microvascular flaps or after radio(chemo)therapy. Our results with PCT are promising in terms of differentiating cancer from post-therapeutic changes in the follow-up of patients with HNC. The results also indicate that even higher significance levels can be achieved in differentiating tissues by normalization of PCT-derived perfusion values to tissues of reference.
Unlike conventional CT or MRI techniques, PCT not only allows accurate delineation of cancer extension into the surrounding soft tissue but also offers the unique ability to quantify the abnormal neoangiogenesis of malignant tissue noninvasively. This is significant, as the information derived from PCT may predict a patient’s response to radio- and chemotherapy. Low perfusion of HNC may be associated with higher failure rates of radiotherapy [2, 23–27]. In fact, Mukherji et al. suggest that pre-treatment identification of non-responders can spare patients an unnecessary radiotherapy, thus allowing earlier initiation of an alternative strategy such as surgical resection and adjuvant chemotherapy. Therefore, complications of salvage surgery and associated wound-healing problems after radiotherapy as well as other complications associated with radiation could be avoided in patients not likely to respond [28].
Although the results presented here are promising, our study has some limitations. First, PCT requires additional imaging series and thus involves higher radiation exposure. So, it may be advisable to perform PCT with a low tube voltage protocol (80–100 kV) to reduce radiation. The mean dose-length product (DLP) of head and neck PCTs in this study was 565,5mGy*cm. This results from multiple repeated helical scans (n=40) used to calculate PCT. In comparison, the diagnostic reference level for one singe helical standard head and neck CT in Germany is given as 330mGy*cm [29].
Most patients received or are going to receive radiation therapy in the course of their treatment. Therefore, diagnostic doses of radiation as applied here with PCT are not expected to have a significant impact on the health of these patients.
Further, applying contrast media to high-risk patients poses the risk of the development of a contrast induced nephropathy (CIN) [30, 31].
While PCT of the head and neck remains a novel technique, MRI and positron emission tomography (PET) are strong competitors. While MRI has the obvious advantage of not using ionizing radiation and providing high soft-tissue contrast, absolute quantification of tumour perfusion with diffusion imaging remains difficult because the relationship between signal intensity and the gadolinium concentration is not always linear [32]. More recently, reports on possible gadolinium deposition in the brain have raised concerns about the uncritical widespread use of gadolinium-based contrast agents [33]. Finally, it must be noted that the processing of PCT images is time consuming, and normalization has to be done manually so far.
In conclusion, this study shows that PCT, using the maximum slope algorithm, can significantly differentiate between cancer, benign and post-therapeutic tissue in the head and neck region, allowing cancer detection in initial work-up and identification of tumour-free patients during follow-up.