
Abstract
We described a patient with symptomatic giant hepatic hemangioma (GHH) treated with laparoscopic guided percutaneous microwave ablation (MWA). A 58 years’ old woman was referred to our hospital who presented with upper abdominal distension and appetite loss for more than 1 year. The medical history included untreated multiple hepatic hemangiomas (HH) that had been detected 13 years ago and hypertension for more than 12 years. Initial laboratory tests revealed D-dimer mild increase and negative tumor markers. Magnetic resonance (MR) imaging demonstrated multiple nodules of different sizes in the liver and the largest lesion was located on the left lobe (longest diameter 12.8 cm), which replaced the whole enlarged left lobe and compressed the gastric body and inferior vena cava. Contrast-enhanced ultrasound (CEUS) and contrast-enhanced MR imaging both showed the typical enhancement pattern of hemangioma and abnormal perfusion was seen in the surrounding liver parenchyma. With the laparoscopy guidance, we performed microwave ablation till the whole tumor was seen atrophy. The total operation duration was 2 hours, with intra-operative blood loss less than 20 ml. The post-operative course was uneventful. The patient was discharged 3 days after the operation. Abdominal distension decreased, appetite improved, blood pressure controlled at normal level after the operation. MR revealed significant volume reduction of the tumor after the operation.
Introduction
Hepatic hemangioma (HH) is the most common benign liver tumor with incidence rate between 0.4–20% [1, 2], which is usually discovered by health screening in asymptomatic population. Symptomatic or giant fast-growing hemangiomas should be referred to experienced multidisciplinary team (MDT), according to the European Association for the Study of the Liver (EASL) clinical practice guidelines on the management of benign liver tumors [1]. Surgical resection is the traditional therapy for symptomatic hepatic hemangioma [3–5]. Several studies have reported the treatment options for GHH, including trans-catheter arterial embolization (TAE) [6–9], radiotherapy, medication and intervention treatment [10–14], however, rare reports have been seen for giant hepatic hemangioma (GHH) >10 cm. Laparoscopy or image-guided percutaneous microwave ablation (MWA) has been proposed in recent years [10, 15] as a safe, feasible and effective treatment for GHH with better outcome, lower cost and less pain, compared with conventional open hepatic resection. Herein we described a patient with GHH treated with laparoscopic guided percutaneous MWA, and also the related literatures were reviewed.
Case report
A 58 years’ old woman presented with upper abdominal distension and appetite loss for more than 1 year, with no special finding in earlier gastroscopy. The medical history included untreated multiple hepatic hemangiomas that had been detected 13 years ago, which kept growing during long term follow-up. She also had hypertension for more than 12 years. The initial laboratory tests revealed the following: white D-dimer, 1.31 mg/L (normal, <0.55 mg/ml); total protein 75.5 g/L (normal, 65–75 g/L); the serum concentration of alpha-fetoprotein was <0.91 ng/ml (normal, <7).
US (Fig. 1A) and MR (Fig. 2A) demonstrated multiple nodules of different sizes in the liver and the largest lesion was located in the left lobe (longest diameter 12.8 cm, estimated volume 471.04 ml), which replaced the whole enlarged left lobe and compressed surrounding structures such as gastric body and inferior vena cava. Pre-operative CEUS (Fig. 1B) and Contrast-enhanced MR imaging (Fig. 2B) showed typical enhancement pattern of hemangioma, peripheral nodular enhancement in arterial phase and gradual inward fill-in in portal phase, and abnormal perfusion was seen in the surrounding liver parenchyma [16–18]. We diagnosed the leision as giant hepatic hemangioma (GHH).
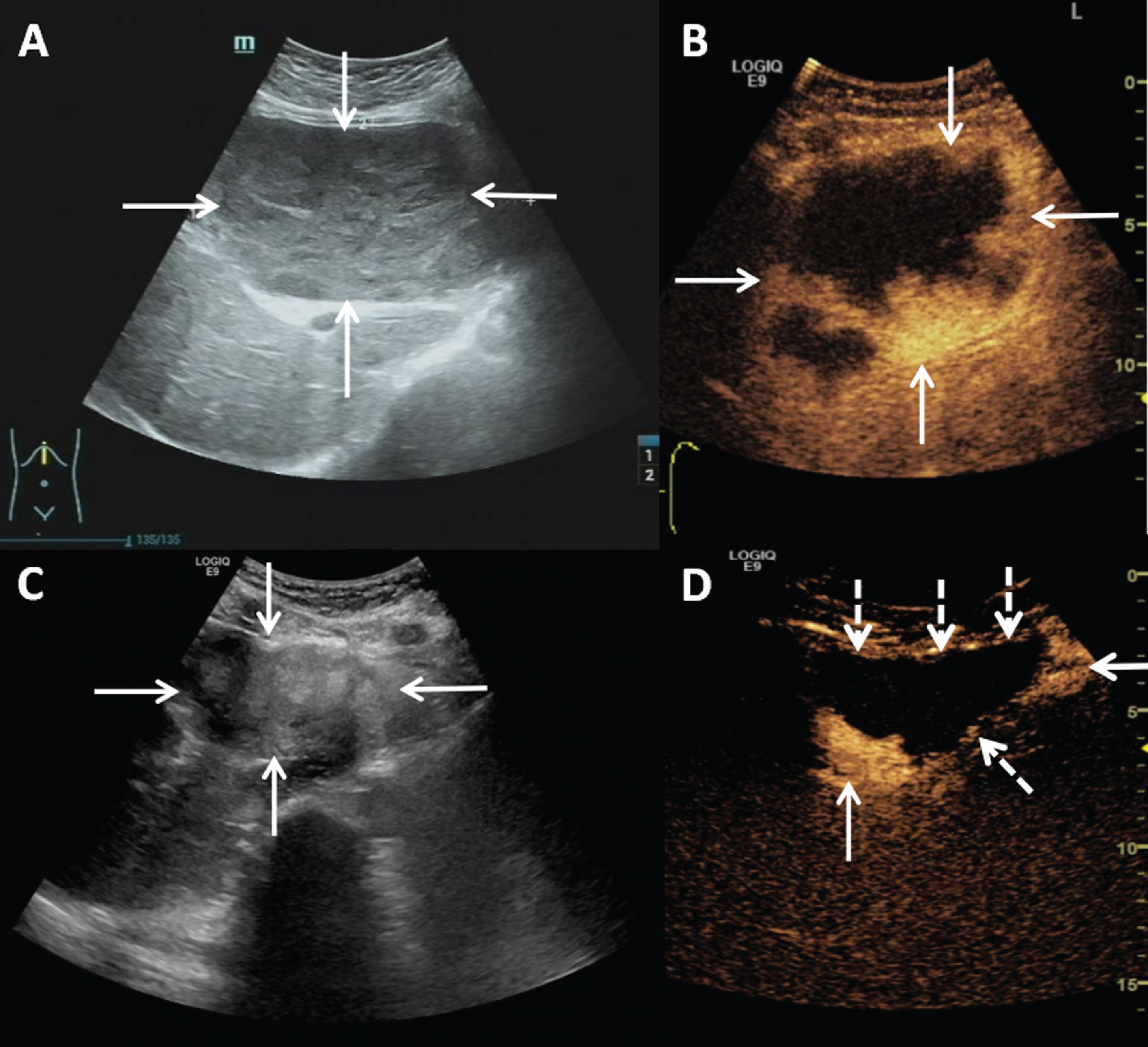
Pre-operative B mode ultrasound shows a well-defined giant hypoechoic mass which replaces the left lobe of the liver (A); Pre-operative CEUS shows peripheral nodular enhancement (the solid arrow) 1 minute 50 seconds after sonovueTM 1.5 ml injection (B). Post-operative B mode ultrasound reveals the tumor turns to be heterogeneous mixed-echoic mass with blurred boarder (C); post-operative CEUS shows no significant enhancement in most area of the tumor (the dotted arrow) except small residual peripheral nodular enhancement area on the left and right-posterior (the solid arrow) (D).
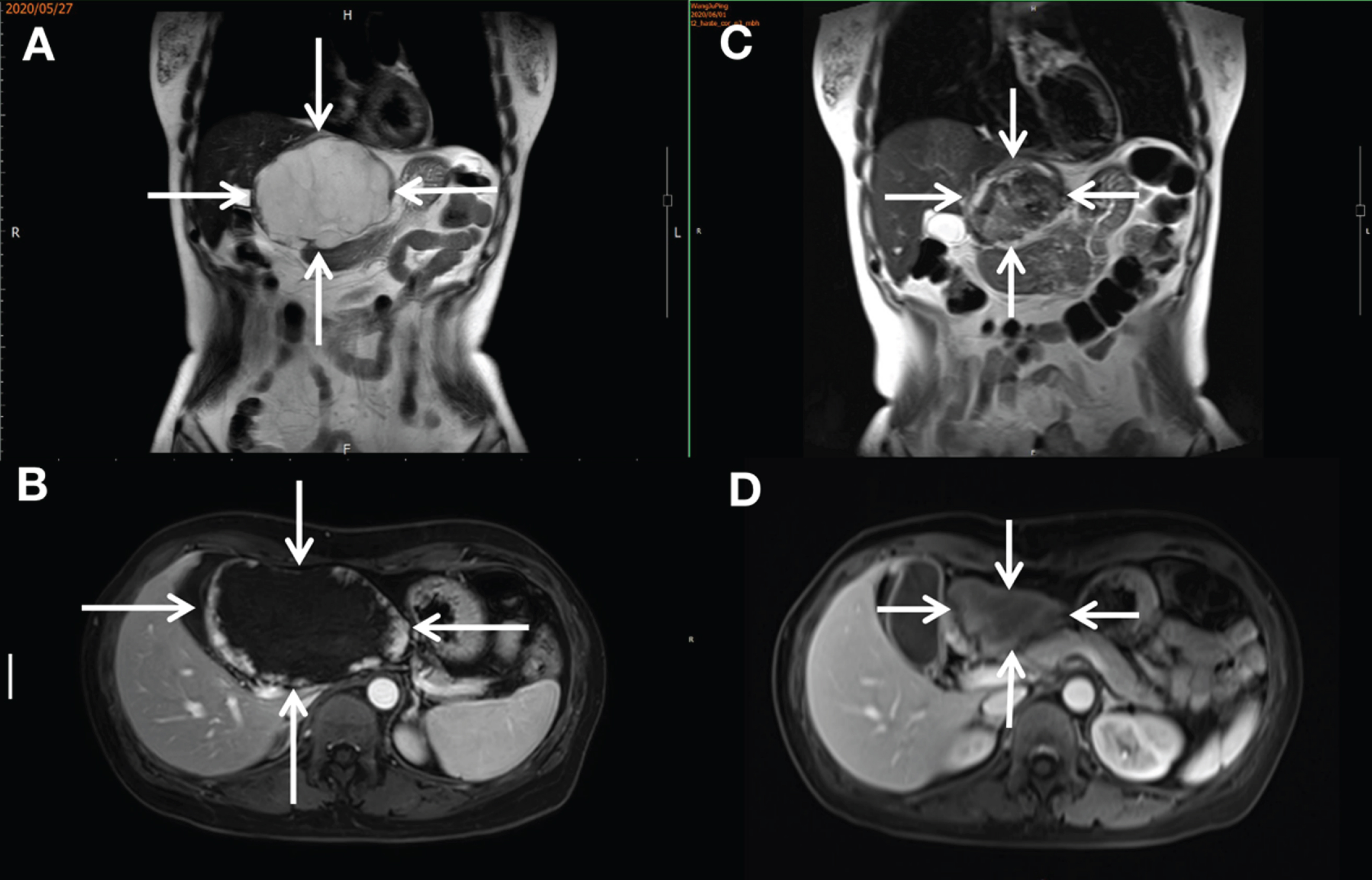
Pre-operative T1 weighted MR demonstrates that the left lobe of the liver is occupied by a huge long signal mass, with the longest diameter being 12.8 cm (A); the contrast-enhanced MR imaging shows peripheral nodular enhancement in the early arterial phase (B). Post-operative T1 weighted MR displays a shrinked tumor, with the longest diameter being 8.9 cm (C); the contrast-enhanced MR imaging shows no significant enhancement except peripheral inflammatory edema zone (D).
MWA was scheduled for the patient and laparoscopic guidance and assistance was selected instead of US guidance due to the close adjacency to cardia and gastric body.
With laparoscopic guidance, we saw the whole left lobe was replaced by the tumor (Fig. 3A). After separating the tumor with surrounding tissues, we placed 5 gauzes under the tumor to protect the peri-hepatic organs (Fig. 3); then we performed sequential MWA point by point under the auxillary support of laparoscopic lever (Fig. 3C), till the tumor were atrophic (Fig. 3D). The total ablation duration was 53 minutes 30 seconds, intra-operative blood loss controlled within 20 ml. The whole operation duration was 2 hours, including anesthesia, disinfection,etc. To prevent hemoglobinuria which could leads to acute renal dysfunction, we gave intravenous drip of 5% sodium bicarbonate solution 150 ml and equilibrium liquid more than 2000 ml during the operation and the first day after operation.

Pre-ablation laparoscopy shows the left lobe of the liver is occupied by huge hepatic hemangioma (A); 5 gauzes are placed under the tumor to protect the surrounding organs, the tumor is then lifted by the laparoscopic operating arms to facilitate ablation (B); percutaneous MWA is carried out from point to point (C); the tumor significantly shrinks after MWA (D).
The patient was closely monitored in the surgical intense care unit for 48 hours after the operation, and given symptomatic and supportive treatment according to the laboratory test result. The blood and urine routine test, liver and renal function examinations was performed every 12 hours. The patient had hematuria 2 hours after operation, which turned to normal in 20 hours. Serum alanine transaminase (ALT), aspartate aminotransferase (AST), direct bilirubin (DB) showed a transient rise and all returned to normal on the third day after operation. The patient was discharged 3 days after the operation, with abdominal distension decreased, appetite improved, and blood pressure controlled at normal level. The radiological shrink rate of the tumor estimated by MR on the third day after operation was 80.8% (tumor volume 471.04 ml –90.4 ml).
Post-treatment US (Fig. 1C) and MR (Fig. 2C) both revealed hypertrophy of the left lobe of the liver after the operation, the tumor shrinked significantly (longest diameter 7.9 cm, estimated volume 90.4 ml); CEUS (Fig. 1D) displayed no enhancement and contrast-enhanced MR imaging (Fig. 2D) showed no significant enhancement in the leision.
Hepatic hemangioma is usually asymptomatic, but 61% will grow during long term follow up [19] and up to 44.7% grows with volume-increase rate more than 5% [20]. The peak growth rate of hemangioma size was reported to be 8–10 cm in young people. The incidence rate of spontaneous bleeding, rupture and other severe complications was low (9/239) [19, 21], but it might be under-estimated. During a giant hepatic hemangioma rupture, it takes less than 30 minutes from abdominal pain to death. Some patient died on the way to hospital or even before rescue came or died suddenly without anyone knowing.
It is a common consensus that treatment should be considered to symptomatic HH patients, those with continuous growth, and those with adjacent organ compression or other severe complications (Kasabach-Merrit Syndrome or spontaneous bleeding). In the treatment of giant hepatic hemangioma patients, minimally invasive, effective, safe, fast recovery should be considered as the main factors [1, 22]. Since hepatic hemangioma has specific manifestation in enhanced ultrasound and MR imaging, the accuracy of diagnosing hemangioma based on imaging examination is relatively high. Thus, we considered puncture biopsy unnecessary before the ablation procedure, as it might cause uncontrollable hemorrhage.
Here we reviewed all the literatures related to intervention therapy retrievable as shown in Table 1. Image-guided percutaneous ablation has been used for treatment of HH in clinical practice for several years, and has been reported to be as effective as resection in both radiological and clinical response, which has the advantages such as less blood lose, less pain, less analgesia use, shorter operation duration, shorter hospital stay, less cost than resection [12, 23]. Radio frequency ablation (RFA) is usually used for HHs between 5 to 10 cm [11, 14], whereas it has high rate of severe post-operation complications [14] for GHH > 10 cm. The first study about the application of MWA in the treatment of GHH was reported by Timothy in 2014 [24], with clinical effectiveness rate up to 98%, volume decrease rate 60–62% after operation [24, 25]. In a report of 13 giant hepatic hemangiomas (>10 cm, mean diameter: 11.7±1.6 cm) in 12 patients, the mean operation duration is 39.0±14.4 minutes for a single leision when 2 electrodes were used at the same time, but the discomfort and complication incidence rate was as high as 100% [10]. During the ablation, it should be kept in mind that extra-high output power at the beginning could induce a rapid temperature and pressure increase inside the tumor, which would even cause massive bleeding from the puncture site. Since the output power of single-electrode percutaneous MWA is relatively stable, it might prolong the operation duration but decrease the massive bleeding risk. In this case, we used single-electrode MWA with mean power 80 W maintained for 3–10 minutes till the tumor near the puncture site was coagulated, started ablation from the center of the tumor, then moved the electrode from point to point till the whole tumor was ablated. Finally, the intra-operative blood lose was within 20 ml.
Retrievable literatures related to thermal ablation therapy for GHH
Note: VSR, volume shrink rate; CR, complication rate.
Laparoscopy guided MWA is recommended as a valid option for the treatment of sub-capsular tumors, but with higher complication rate compared with percutaneous MWA [15]. In the case we described, we used laparoscopic arm’s assistance to achieve complete tumor ablation. At the same time, separating the tumor with adjacent organs could help avoiding thermal injury of diaphragm, cardia and gastrointestinal ducts.
Ablation of a hyper-vascular hemangioma could lead to hemolysis, even acute kidney dysfunction [19, 22]. The patient should be given sufficient hydration before, during and after the ablation operation. Once the duration of ablation reaches half an hour, intravenous drip of sodium bicarbonate solution should be given immediately to alkalize the urine. If the indicators of hemolysis such as body temperature increase or hemoglobinuria arises showed during the operation, the WMA procedure should be terminated.
In summary, laparoscopy-guided percutaneous MWA is an effective, minimal invasive procedure for GHH, which has the potential to become an alternative treatment in the future.
Conflicts of interest
The authors declare that there are no conflicts of interest regarding the publication of this article.
Footnotes
Acknowledgments
This work was supported in part by the National Natural Science Foundation of China (Grants 81671695, 81725008 and 81927801), Fundamental Research Funds for the Central Universities (Grants 22120190213), Shanghai Municipal Health Commission (Grants 2019LJ21 and SHSLCZDZK03502), and the Science and Technology Commission of Shanghai Municipality (Grant 19DZ2251100).