
Abstract
BACKGROUND:
Red blood cell (RBC)-modifying therapies have provided new opportunities for patients with sickle cell disease, although the absence of validated biomarkers of RBC function is a barrier to FDA approval and clinical adoption. Flow Adhesion (FA) and Mechanical Fragility (MF) biomarkers objectively stratify individuals with SCD into pro-adhesive vs pro-hemolytic phenotypes respectively, which may potentially help predict therapeutic responses.
OBJECTIVE:
A Phase 3 clinical trial to determine the effectiveness of vepoloxamer, an RBC-modifying therapy in sickle cell disease (SCD), failed to meet its primary clinical outcome. The aim of this study was to determine whether standardized flow adhesion and mechanical fragility bioassays could differentiate cellular level “responders” from “non-responders” to vepoloxamer treatment.
METHODS:
Standardized biomarkers of RBC function (adhesion and mechanical fragility) were utilized in this study to assess the effect of veploxamer on blood samples collected from SCD subjects and to determine whether our assays could differentiate cellular-level “responders” from “non-responders” to vepoloxamer treatment. A Wilcoxon signed-rank test was used to test for differences in adhesion in response to varying vepoloxamer treatments and a Wilcoxon Mann-Whitney test was used to assess differences in mechanical fragility, pre- and post-vepoloxamer treatment. A p-value<0.05 was considered significant.
RESULTS:
In this study, we report that in vitro treatment with vepoloxamer reduced adhesion by >75%in 54%of patient samples and induced changes in the membranes of sickle erythrocytes (SSRBCs) making sickle cells behave more like normal erythrocytes (AARBCs) in terms of their resistance to hemolysis.
CONCLUSION:
This study demonstrates that the standardized flow adhesion and mechanical fragility biomarkers described here may be useful tools to predict clinical responders to RBC-modifying therapies.
Background
Vaso-occlusion is the primary pathophysiologic sequela of sickle cell disease (SCD), and results in intense pain and tissue damage. The accumulative life-time burden of tissue damage results in frequent, painful acute vaso-occlusive episodes (VOEs). Pain is highly subjective and a very difficult clinical outcome to measure in clinical trials and clinical practice. Other endpoints have been used such as length of stay, time to readiness for discharge, and intravenous pain medication requirements. These pain surrogates require a subjective third-party assessment and vary from patient-to-patient, thus making them inadequate clinical endpoints to assess the efficacy of an RBC-modifying therapy.
Sickle erythrocytes (SSRBCs) contribute to the pathogenesis of vaso-occlusion, in part, by abnormally adhering to the vascular endothelium. The degree of adherence correlates with clinical vaso-occlusive severity [1, 2]. Very late antigen-4 (VLA-4) is one of the most well-characterized adhesion receptors on SSRBCs. Reticulocyte VLA-4 expression is higher in SCD subjects with frequent VOEs and decreased in SCD patients treated with HU [3, 4]. VLA-4 is present on SSRBC populations with increased adhesiveness and supports adhesion between SSRBC and endothelial vascular cell adhesion molecule-1 (VCAM-1) [5, 6]. VLA-4 on SSRBCs also mediates SSRBC and mononuclear leukocyte cell-to-cell adhesion either directly or indirectly via fibronectin, forming cell aggregates on the endothelial surface or in suspension [7, 8]. In murine SCD models, adhesion of SSRBCs and leukocytes to endothelium are reversed by antibodies that block VCAM-1 [6, 9].
SSRBC membrane properties play a key role in adhesive and obstructive events in SCD [10, 11]. Sickle hemoglobin (HbS) polymerization critically impacts membrane structural proteins, like Band-3 complex, resulting in membrane micro-vesiculation [12]. Associated oxidative damage causes defects in membrane structures resulting in irreversible micro-rheologic abnormalities of SSRBC membranes,[13] structural membrane rearrangements, and ultimately plastic membrane damage [14, 15]. Accumulated “sub-lethal” red blood cell (RBC) damage may be a key factor in accelerated SSRBC senescence [16] and ultimately hemolysis and/or premature cell removal from the circulation by the spleen [17]. SSRBCs with “fragile” membranes are prone to hemolysis, which results in the release of intracellular contents that promote inflammation and induce expression of adhesion molecules (e.g.VCAM-1) [18]. Destabilization of the RBC membrane and cell sickling also results in premature cell destruction and release of hemoglobin, which contribute to SCD pathology by limiting nitric oxide bioavailability [19] and promoting oxidative damage [20]. Hemolysis is associated with SCD complications such as pulmonary hypertension, priapism, ulcers and stroke, [21] with even low levels of serum Hb increasing RBC aggregation [22]. Toxicity of cell-free Hb contributes to impaired microcirculation, vasoconstriction, diminished oxygen delivery, [23–25] as well as, proinflammatory and vaso-occlusive effects [26–28].
A Phase 3 clinical trial (EPIC) to determine the effectiveness of vepoloxamer (purified MST-188) in alleviating VOEs in SCD recently failed. Vepoloxamer, an amphipathic triblock copolymer, is believed to improve rheology in SCD by non-specific intercalation with the RBC membrane, resealing damaged pores and increasing lipid packing density [29, 30]. Prior clinical studies demonstrated the ability of MST-188 to reduce acute VOE duration and total opioid analgesic requirements in SCD [31]. In the EPIC trial, vepoloxamer failed to meet its primary outcome to significantly reduce the duration of acute VOEs, an endpoint based on patient’s subjective perception of pain. In the absence of standardized biomarkers of RBC function, the discrepancy between promising preclinical data and the clinical endpoints is difficult to ascertain.
Since the EPIC trial, there have been more promising RBC-modifying therapies that have failed to show a reduction in acute pain crises duration in phase 3 clinical trials. As more RBC modifying therapies are investigated in SCD, it is critical to deploy objective measures of cellular-level response as predictive, monitoring, and surrogate biomarkers. The aim of this study was to determine whether standardized flow adhesion and mechanical fragility bioassays could be applied to assess changes in select functional properties of RBCs induced by vepoloxamer. Simultaneous use of both Flow Adhesion (FA) and Mechanical Fragility (MF) biomarkers dovetails with the two main SCD phenotypes, adhesive and hemolytic, which can be linked to different clinical disease states, and potentially to different response to the therapy [32]. Of particular interest was whether the bioassays could differentiate “responders” from “non-responders” to vepoloxamer treatment, exploring a potential scaffold for validating biomarkers to predict clinical responders to RBC-modifying therapies.
Material and methods
Reagents
Vepoloxamer was a gift from Mast Therapeutics (San Diego, CA). Recombinant human VCAM—1 (rhVCAM-1) was purchased from R&D Systems (Minneapolis, MN) and human umbilical vein endothelial cells (HUVECs) from Lonza (Walkersville, MD).
Blood donors
Informed consent protocols were performed following institutional review board (IRB) approval by Wayne State University and the University of Michigan. Blood samples were collected in sodium citrate from non-SCD (n = 15) and SCD subjects (HbSS; n = 26; Table 1).
SCD Demographics
SCD Demographics
Flow adhesion assays were performed with a commercial well-plate, microfluidic flow system (BioFlux 1000Z, Fluxion, San Francisco, CA) by modification of published methods [33, 34]. To assess adhesion, channels were seeded with human umbilical vein endothelial cells (HUVECs; Lonza, Basel Switzerland) or coated with VCAM-1. Blood samples were pretreated with varying concentrations of vepoloxamer (0.1, 1, 10 mg/mL) and perfused through microfluidic channels during flow (1.0 dyne/cm2, 1.67 Hz). Images were acquired with a high—resolution CCD camera and analyzed with Montage imaging software (Molecular Devices, Downington, PA). Adherent cells were quantified to generate an adhesion index (AI; cells/mm2).
Mechanical fragility (MF) assay
Whole blood samples were diluted to Hb concentration of 1.7 g/dl and verified with a Hemoglobin 201 system (HemoCue; Angelholm, Sweden). Mechanical stress was applied using a TissueLyser LT (Qiagen, Dusseldorf, Germany) vertical bead mill at an oscillation frequency of 50 Hz in the presence of one 7 mm diameter stainless steel ball, as previously described [35]. Following centrifugation, hemolysis was measured in supernatants by calculating the difference between absorbance at 576 nm (wavelength of oxygenated Hb maximum) and 685 nm (local minimum for the oxygenated Hb form) using a NanoDrop N100 spectrophotometer (Thermo Scientific, Waltham, MA) while accounting for the Sowemimo-Coker correction [36]. Hemolysis metrics (Hem) were used to represent amount of hemolysis from i) a labile RBC subpopulation lysed after 3 minutes of stress application (L-Hem), ii) a more stress-resistant RBC fraction that lysed between 3 and 10 minutes of stress application (R-Hem), or iii) the cumulative hemolysis induced over the full 10 minute stress-supplication time (C-Hem). Values were obtained from best-fit second-order polynomial regression of the experimental data.
Statistical analysis
Statistical analysis was performed with GraphPad Prism software (San Diego, CA). Differences within each patient were analyzed using Wilcoxon signed-rank test, a non-parametric statistical hypothesis test used for repeated measurements on the same sample to compare their population means. Wilcoxon Mann-Whitney tests were used to assess differences in samples pre- and post-vepoloxamer treatment. A p-value <0.05 was considered significant.
Results
This study enrolled SCD volunteers (n = 26) aged between 1 and 19 years. The study included comparable numbers of males and females and volunteers on (N = 5) and off (N = 21) hydroxyurea therapy. Hematology and chemistry labs were obtained during research draws. Blood samples were obtained from SCD subjects at steady state benign clinic visits.
Flow adhesion
Blood samples from SCD subjects were pretreated with varying concentrations of vepoloxamer (0, 0.1, 1, 10 mg/mL) and perfused through microfluidic channels seeded with HUVECs or coated with VCAM-1 to assess the effect of vepoloxamer on whole blood adhesion to HUVECS and VCAM-1. Flow conditions (1.0 dynes/cm2, 1.67 Hz) simulate blood flow in the post-capillary blood venules where these adhesive interactions are likely to occur. Steady state adhesion varied from patient-to-patient (HUVECs: mean = 20.67±28.4 cells/mm2, range = 8–34 cells/mm2; VCAM-1: mean = 302.4±3.2 cells/mm2, range = 50–492 cells/mm2; Fig. 1A). As shown in prior studies [33], steady state adhesion of whole blood to VCAM-1 was significantly higher in SCD subjects with higher reticulocyte counts (R2 = 0.22; p = 0.017; Fig. 1B), although steady state adhesion of whole blood to HUVECs did not correlate with clinical lab data (data not shown). Vepoloxamer (0.1, 1, and 10 mg/mL) significantly reduced adhesion to HUVECs (mean = 41%inhibition, p = 0.0002; Fig. 2A) and VCAM-1 (mean = 69.5%inhibition, p < 0.0001; Fig. 2B) at 1 mg/mL. Steady state adhesion indices were not predictive of cellular-level response to vepoloxamer (data not shown). 54%of patients’ samples were classified as responders (n = 14; from 44.0 to 91.4%) at 1 and 10 mg/mL vepoloxamer, while 46%were classified as non-responders (n = 12; from 43.7 to 91.4%) (Fig. 2C).

Flow adhesion in SCD blood samples. A) Steady state adhesion to HUVECs (left y-axis) and VCAM-1 (right y-axis) varies in SCD blood samples. B) SSRBC adhesion to VCAM-1 correlates with reticulocyte percent.
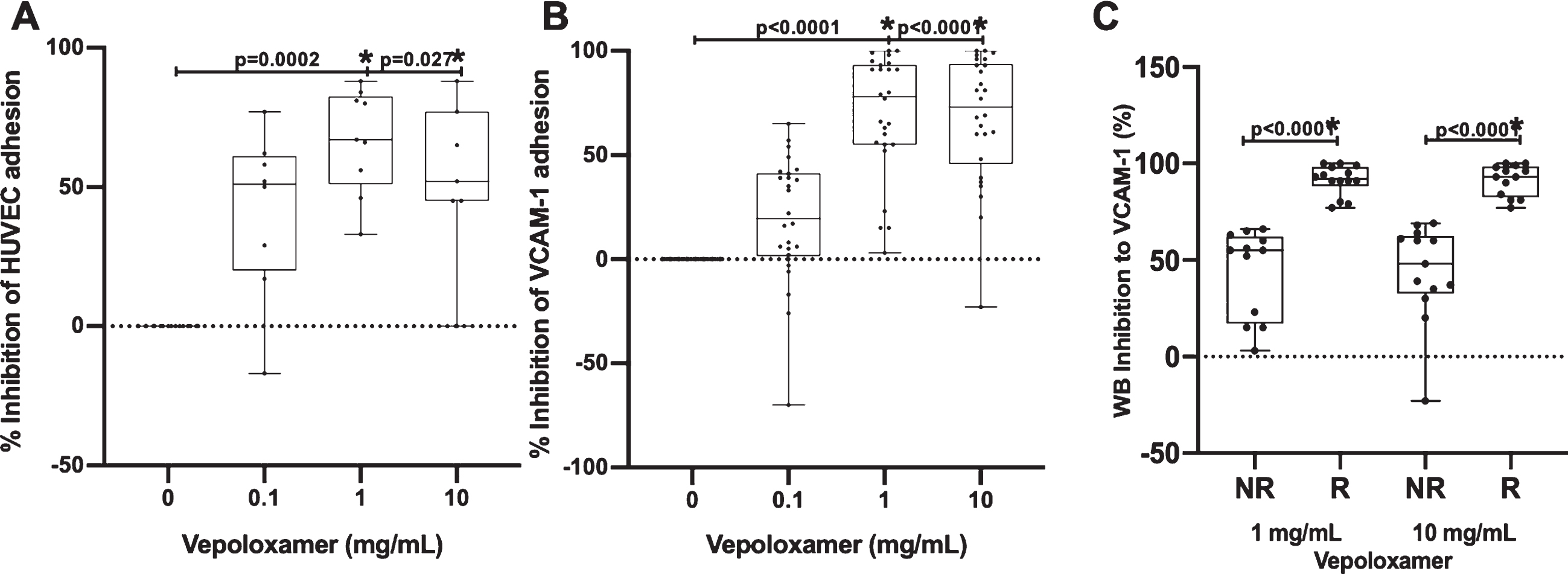
Effect of vepoloxamer on SSRBC adhesion in SCD. Vepoloxamer significantly reduces adhesion to HUVECs (A) and VCAM-1 (B) in SCD blood samples. C) Veoploxamer responders were classified as SCD patients demonstrating > /=75%inhibition at 1 and 10mg/mL vepoloxamer. Responder and non-responder groups were significantly different at both vepoloxamer concentrations.
Mechanical fragility was assessed at baseline and at 1 mg/mL vepoloxamer. The higher volume requirement for this assay precluded testing multiple doses. A statistically significant reduction in L-Hem (p = 0.0452) was observed in response to 1 mg/mL vepoloxamer treatment of SSRBCs, whereas there was no significant difference observed in the more resistant fraction, R-Hem (p = 0.6162) and C-Hem (p = 0.0892) (Fig. 3A; Table 2).
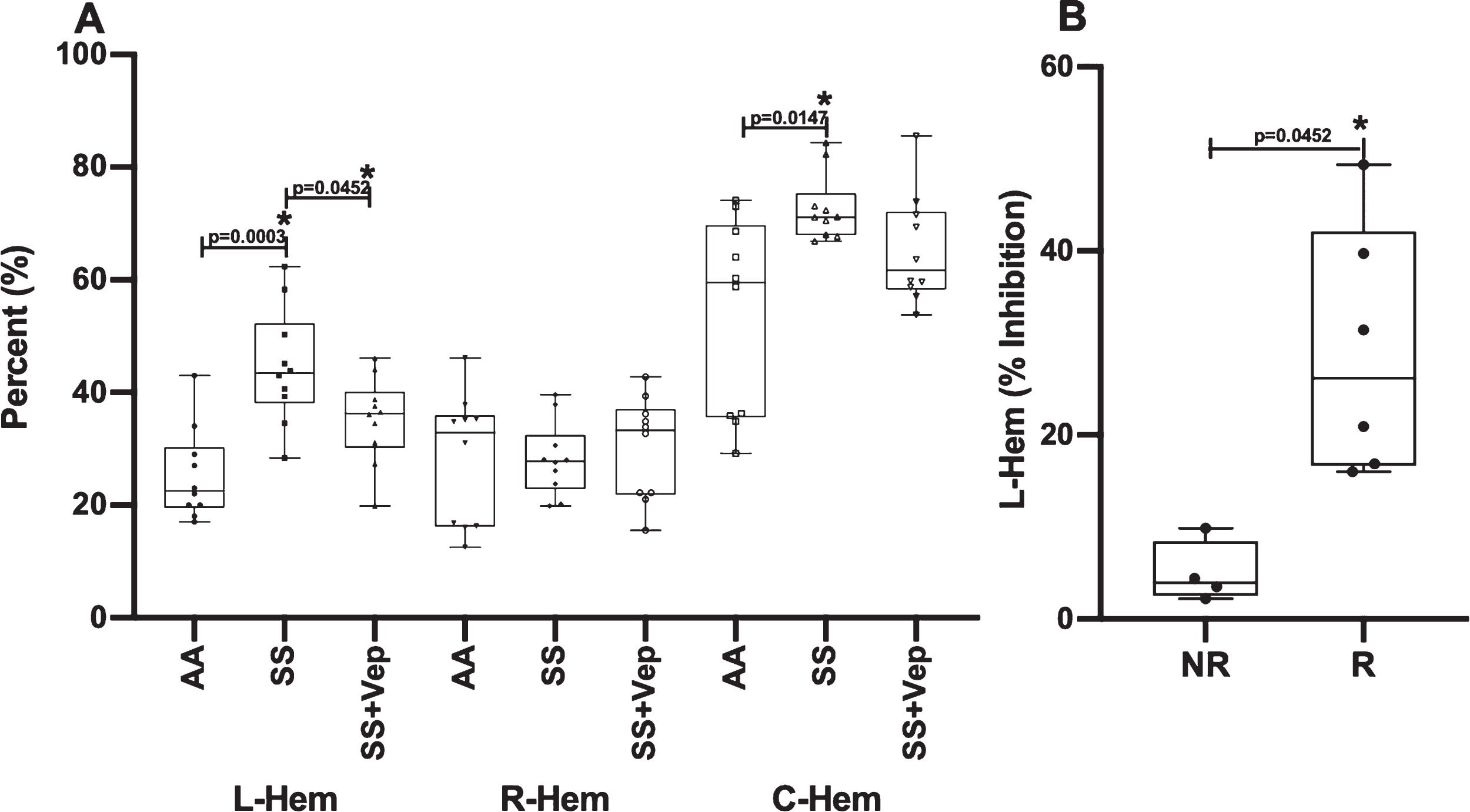
Vepoloxamer reduces mechanical fragility in SSRBCs. A) Induced hemolysis in labile (L-Hem; p = 0.0003) and cumulative (C-Hem; p = 0.0147) SSRBC fractions was significantly higher than normal erythrocytes (AARBCs), however there was no difference for the resistant fraction (R-Hem). Vepoloxamer (1mg/mL) significantly reduced L-Hem (p = 0.0452), whereas there was no significant difference observed in the more resistant fraction, R-Hem (p = 0.6162), and C-Hem (p = 0.0892). B) SCD subjects were stratified into two groups based on the magnitude of the decline in labile SSRBC fractions (L-HEM) in the presence of vepoloxamer and designated as “responder” or “non-responders”.
Mechanical Fragility
In untreated SSRBC blood samples, induced hemolysis in both labile (L-Hem; p = 0.0003) and cumulative (C-Hem; p = 0.0147) SSRBC fractions was significantly elevated as compared to normal erythrocytes (AARBCs), however significance was not achieved for the more resistant fraction (R-Hem; p > 0.9999) (Fig. 3A; Table 2). Similar to the difference between SSRBCs and AARBCs, following vepoloxamer treatment of SSRBCs, C-HEM was no longer significant (p = 0.0.0892).
SSRBC exhibited significant subject-to-subject variability in the magnitude of vepoloxamer-associated reduction in induced hemolysis. SCD subjects in this study can be stratified into two groups based on the magnitude of the decline in labile SSRBC fractions (L-HEM) in the presence of vepoloxamer. The average decline in L-Hem on vepoloxamer supplementation was 19.44±5.097 percent with subjects naturally falling into two groups based on their response to therapy (Fig. 3B). The “responder” group showed a decline in L-HEM (29.06±5.527%) vs. “non-responders” (5.007±1.679%). This difference was statistically significant (p-value = 0.0095). While there was no statistically significant difference between the two groups in white blood cell count, total hemoglobin, hematocrit or platelet count, the groups demonstrated significant difference in reticulocyte counts (responders: 7±4, non-responders: 15±5%; p < 0.05).
Standardized biomarkers of RBC function (adhesion and mechanical fragility) were utilized in this study to assess the effect of veploxamer on blood samples collected from SCD subjects and to determine whether our assays could differentiate cellular-level “responders” from “non-responders” to vepoloxamer treatment. Adhesion indices, obtained from our standardized, flow-based adhesion bioassay, varied from patient-to-patient in SCD subjects at steady state and likely represents highly variable SCD phenotypes amongst patients. Adhesion indices were correlated with hematologic parameters to identify influencers of adhesion in our flow system. Steady state adhesion of whole blood to VCAM-1 positively correlated with reticulocyte percent. Reticulocytes highly express VLA-4, a ligand for VCAM-1, which likely accounts for the positive relationship with adhesion to VCAM-1.
Blood samples pretreated with vepoloxamer (0.1, 1, and 10 mg/mL) significantly reduced adhesion to HUVECs and VCAM-1 at 1 mg/mL. Similarly, previous reports have demonstrated that vepoloxamer reduces adhesion to microvascular endothelial cells [37]. HUVECs, a macro-vascular cell line, has been used in numerous sickle cell, flow-adhesion studies to evaluate SSRBC adhesion to an endothelial substrate [6, 39]. TNF-alpha upregulates the expression of VCAM-1 on the endothelial surface [40]. While stimulated HUVECs used in this study are an effective in vitro model, integration of an endothelial cell-based bioassay into clinical studies is not practical. VCAM-1 is a more reliable, standardized alternative for assessing RBC adhesive properties. Interestingly, vepoloxamer’s non-specific mechanism did not interfere with its ability to inhibit specific high avidity interactions such as VLA-4/VCAM-1. These data validate the use of an isolated adhesive substrate as a surrogate for a more physiologic endothelial substrate in a standardized clinical adhesion assay.
The in vitro effect of vepoloxamer was highly variable in this sickle cell population, similar to the variable response observed in prior studies evaluating blood function biomarkers [41, 42] and clinical response to SCD-modifying therapy given in the acute setting [43], as well as, maintenance therapy [44, 45]. Steady state adhesion indices were not predictive of cellular-level response to vepoloxamer. In vitro treatment with vepoloxamer reduced adhesion by > 75%in 54%of patient samples may be useful tools to predict clinical responders to RBC-modifying therapies.
For the purposes of this study, we set 75%inhibition as the “responder” threshold. Based on this definition 54%of patients’ samples were classified as responders at 1 and 10 mg/mL doses of vepoloxamer concentrations, while 46%were classified as non-responders.
Elevated mechanical fragility in SSRBCs, as compared to AARBCs, has been reported previously [14, 46] along with high subject-to-subject variability, however those studies did not differentiate between RBC fractions based on their stability under applied stress. The findings presented here indicate that vepoloxamer induced changes in the membranes of SSRBCs making sickle cells behave more like AARBCs in terms of their resistance to hemolysis. This “normalization” of sickle cell response to stress relative to cells from normal donors, can be interpreted in terms of the compound facilitating stabilization of RBC membranes through the reversal of accumulated polymerization-induced membrane damage. Mechanical Fragility data indicate that vepoloxamer predominantly affects labile/fragile (less resistant to mechanical stress) SSRBC fractions (described by L-Hem). The labile fraction of RBCs is characterized by higher accumulated sub-hemolytic membrane damage. Our data is consistent with vepoloxamer’s mechanism of action which is expected to have little or no effect on cells with less perturbed membranes that are presumably less susceptible to hemolysis. These findings also align with previous reports demonstrating that vepoloxamer reduced hemolysis during RBC storage and increases preservation of the most labile cell fraction (impact on more resistant cell fractions was not assessed) [47].
These observations are consistent with the observation that the responder group had elevated, reticulocyte counts compared to non-responders. High reticulocyte counts reflect a potentially younger average sickle RBC populations, presumably with less accumulated membrane damage due to cell age and thus to potentially fewer incidences of polymerization-inducing hypoxia. It could be indeed expected that such RBC populations with less accumulated membrane damage would be less impacted by vepoloxamer treatment. Sandor et. al. reported that RBC deformability assessed by ektacytometry and microfluidics, was not affected by vepoloxamer [37]. These data were interpreted by the authors to suggest that vepoloxamer “does not affect RBC mechanical properties”, thus contradicting the data reported here. However, RBC deformability and MF are regulated by different interactions of skeletal proteins [48]. Although related, the effect of RBC-modifying therapies on these membrane properties are not necessarily identical. The hemolytic propensity of RBCs is known to vary significantly between individuals, [49] due in part to individual differences in RBC metabolic age [50, 51] and ATP levels, [52–54] with likely contributions from ethnicity, age, gender, lifestyle, and genetic pathologies [55–57]. Subject-to-subject variability may be a root cause of differences between an individual’s response to vepoloxamer as assessed by either VCAM-1 adhesion or RBC MF. Differences in the severity of sub-hemolytic SSRBC damage and adhesive properties between patients may be further amplified by the history of hypoxic events and VOEs, and treatment, including hydroxyurea and transfusions [14].
While the causes of differences between responders and non-responders in our study remain to be elucidated, it can be suggested that those may be related to the amount and types of preexisting membrane perturbations and/or damage. For example, the asymmetrical distribution of phospholipids is well conserved throughout the RBC lifespan and its exposure on the membrane surface plays a key role in RBC apoptosis and removal from circulation [58, 59]. Similar to senescent RBCs, abnormal erythrocytes with e.g. membrane disorders, have PS exposed on the external membrane resulting in premature hemolysis [60]. Elevated PS exposure had been suggested as one of the key features of sickle RBC impaired survival in circulation [61] with strong positive correlation observed between exposed PS and cellular adhesion in SCD [62]. Notably, the levels of PS exposure vary significantly even between normal donors, contributing e.g. to RBC loss of viability during storage with original, pre-collection, PS expose levels correlated with RBC oxidative stress markers and fragility [57].
Despite progress made in understanding of molecular mechanisms behind SCD phenomena, lack of reliable biomarkers remains a major barrier to approving emerging therapies in SCD. In this study, we demonstrated that the flow adhesion assay could identify 54%of the vepoloxamer-treated population as responders (>75%inhibition of adhesion). Previous studies have established that baseline adhesion to VCAM correlates to historical disease severity [63]. As a result, vepoloxamer-induced normalization of adhesion indices in 54%of the population may correlate to a clinical response as well. Additionally, our data demonstrated that vepoloxamer predominantly affected more labile/fragile RBC populations, likely characterized by higher accumulated sub-hemolytic membrane damage. As a result, elevated labile fraction of RBCs, as indicated by the mechanical fragility index, may identify individuals more likely to respond to RBC-modifying therapies such as vepoloxamer. Present work shows the potential of drug-induced normalization in adhesion and fragility could serve assurrogate biomarkers for RBC-modifying therapies. In addition to providing new tools for monitoring a patient’s response to therapy, utilization of such biomarkers could enable efficient stratification of patients based likelihood of therapeutic response and/or allow for enrichment in clinical trials by developing and implementing optimal inclusion/exclusion criteria.
The magnitude of clinically meaningful response to a therapy cannot be ascertained solely through pharmacodynamic response to in vitro treatment, but ultimately requires confirmation from biomarker data obtained from treated patients. Variability observed in vepoloxamer response utilizing our flow adhesion and mechanical fragility assays allowed for potential stratification of SCD subjects based on in vitro response and showed the potential of RBC functional assays to differentiate patients based on cellular level pharmacodynamic responses to a RBC-modifying therapy. However, the clinical relevance of responder vs. non-responder stratification remains yet to be validated through clinical outcomes. Further studies are ongoing to determine the utility of RBC function assays such as flow adhesion and mechanical fragility to predict and monitor therapeutic response in both clinical trials and clinical practice.
Footnotes
Acknowledgments
The authors would like to thank Ashley D’Agostino for helping to identify and recruit patients for this study.
Authorship contributions
Jennell White: Experimental design and execution, data analysis, and manuscript preparation.
Xiufeng Gao: Data analysis, and manuscript preparation.
Michael Tarasev: Data acquisition and analysis, and manuscript preparation.
Sumita Chakraborty: Data acquisition and analysis.
Ke Liu: Data analysis, and manuscript preparation.
Marty Emanuele: Data analysis and manuscript review.
Patrick Hines: Project conception and experimental design, and manuscript preparation.
Conflict of interest statement
J. White, X. Gao, M. Tarasev, and P. Hines are employees and shareholders of Functional Fluidics Incorporated, a company developing and commercializing assays for blood cell assessment. M. Tarasev and S. Chakraborty are shareholders of Blaze Medical Devices, a company holding some of the intellectual property pertaining to Mechanical Fragility assays. M. Emanuele was a shareholder of Mast Therapeutics, who participated in the manuscript review in his private capacity. Financial support was received from Mast Therapeutics for the completion of the study. Mast Therapeutics did not participate in the design of the study or in the interpretation of the study results and no longer pursues the use of vepoloxamer for treatment of SCD.