
Abstract
BACKGROUND:
Broad hemodynamic changes, is believed to have a profoundly damaging effect on donor livers after brain death (DBD) or cardiac death (DCD). It remains unclear whether Doppler ultrasonography (DUS) and contrast-enhanced ultrasonography (CEUS), the imaging modalities to evaluate perfusion, could provide more information of liver discarded.
OBJECTIVE:
To evaluate the ability of DUS and CEUS to predict the risk of DBD or DCD liver discarded.
METHODS:
The consecutive DBD or DCD donors with DUS/CEUS examinations before surgical procurement from February 2016 to June 2018 at our institution were included. The US and CEUS images of each donor liver were analyzed and the parameters were recorded.
RESULTS:
Among the 67 eligible donor livers, 15 (22.4%) were discarded and 52 (77.6%) were used. The discarded livers showed prolonged SAT of hepatic artery (0.08s vs 0.06s, OR = 2.169, P = 0.008) on DUS, less cases with homogeneous enhancement (40.0% vs 73.1%, OR = 0.243, P = 0.028) on CEUS, more cases with decreased enhancement (53.3% vs 19.2%, OR = 4.800, P = 0.009), and less difference of the peak time between portal vein and liver parenchymal (0.5s vs 6.7s, OR = 0.917, P = 0.034). The multivariable analysis showed that donor liver with prolonged SAT of hepatic artery (OR = 7.304, 95% CI: 1.195–44.655, P = 0.031) and decreased enhancement (OR = 2.588, 95% CI: 1.234–5.426, P = 0.012) were independent factors of liver discarded.
CONCLUSIONS:
DUS/CEUS could be applied as a promising predictive tool to screen high-risk liver donors. The prolonged SAT of hepatic artery on DUS and the decrease of liver donor in enhancement on CEUS, indicating hemodynamic changes in DBD and DCD donor livers, were risk factors of liver discarded.
Introduction
Expanded-criteria donors (ECD), or marginal allografts, provides an effective alternative means of liver transplantation and is a method of expanding the donor pool considering the demand and supply imbalance for organ transplants [1]. Its use indeed decreases the waiting time for liver transplantation without a severe impact in post-transplant survival [2], but a consequence of a higher rate of discarded livers [3, 4], which inevitably causes a waste of manpower and hospital resource utilization, should be also considered.
In China, the organ donations after citizens’ death have been the sole source since 2015 [5]. To predict discard of these donor livers after brain death (DBD) or cardiac death (DCD) before procurement could spare many unnecessary efforts. Despite some models that use donor risk factors to predict liver allograft discard [3, 6], it’s believed that direct evaluation of the donor liver is the most reliable way to screen a high-risk donor [7].
Imaging, which can provide an accurate picture of liver parenchyma, vascular anatomy, volume measurement and focal lesions, plays an important role in liver transplantation [8]. Ultrasonography (US) is a highly specific imaging tool in screening high-risk liver donors through showing abnormalities in liver parenchyma and presence of focal lesion [7, 8]. For DBD or DCD donors, which broad hemodynamic changes, including compromised organ perfusion, is believed to have a profoundly damaging effect on organ system [9, 10], evaluation of the perfusion of donor liver is also important. Doppler US (DUS) is the first-line imaging method for analyzing hemodynamic changes in macroscopic liver vessels, and contrast-enhanced US (CEUS) is a valuable imaging modality to evaluate microcirculation perfusion of the liver and also focal liver lesions [11–19]. It remains unclear whether DUS/CEUS could provide more information of liver discarded. Therefore, the aim of this study was to evaluate the ability of DUS/CEUS to predict the risk that the DBD and DCD donor livers would be discarded.
Materials and methods
Patients
This study was approved by our institutional review board ([2010] 2–27), and informed consent was obtained from each recipient and immediate family members of each donor. Donor livers from executed prisoners were not used in this study. We identified consecutive DBD or DCD donors with DUS/CEUS examinations before surgical procurement from February 2016 to June 2018 at our institution. Donors who underwent a DUS/CEUS examination more than 24 hours prior to surgical procurement were excluded from the study.
US and CEUS examinations
Using the standard department protocol, all DUS/CEUS examinations of the donors were performed by a trained radiographer (with 5 years of experience in liver US and CEUS examinations) using a GE LOGIQ9 US scanner (GE Healthcare, Milwaukee, WI). The US protocol consisted of a series of both B-mode and Doppler images. In B-mode examinations, the parenchymal echotexture, edge and surface of the liver were recorded [20]. In the Doppler examinations, the color Doppler flow images and spectral Doppler images of the hepatic vessels were recorded.
For the subsequent CEUS examinations, the livers were studied through a longitudinal intercostal scan, in which the trunk and right branch of the portal vein and right liver parenchyma could be easily identified. Dynamic CEUS, with a bolus injection of 1.5 ml of SonoVue™ (Bracco, Milan, Italy) followed by 5 ml of saline solution via a central venous catheter, was performed with a low mechanical index (MI < 0.16). The digital recording was started and performed for 6 min. The probe was kept still on the above mentioned longitudinal intercostal plane for the first 3 min and then moved for another 3 min to scan the entire liver to detect whether there was an anomalous enhanced area.
Imaging analysis
Two radiologists (with 4 and 18 years of experience, respectively, in liver US and CEUS imaging), blinded to all clinical information, independently analyzed the images and video recordings. Discrepant results were reassessed to achieve consensus.
For B-mode US images, the donor livers were classified as normal (with a smooth liver surface, a sharp edge, and normal parenchymal echotexture), liver steatosis (a “bright liver” with evident contrast between hepatic and renal parenchyma) [21, 22] and liver fibrosis (with surface nodularity, coarse echotexture, and blunting of liver edge) [20]. For Doppler images, the caliber and velocity of portal vein (PV), resistance index (RI) and systolic acceleration time (SAT) of hepatic artery (HA) were recorded.
For the CEUS video recordings, the enhancement homogeneities and levels of liver parenchyma were evaluated in the arterial, portal and late phases, as defined by international guidelines [23, 24]. The enhancement homogeneity of liver parenchyma was classified as homogeneous and inhomogeneous (with irregular hypo- or hyper-enhancement area) during the portal phase. The decreased enhancement of liver parenchyma (significantly lower enhancement lever of liver parenchyma than that of PV at the same depth) and the posterior enhancement attenuation (significantly lower enhancement lever of liver parenchyma in the far field than that in the near filed) during the portal phase were also recorded.
Besides, a time-intensity-curve analysis was performed. The arrival time of HA (HAAT) and PV (PVAT), the peak time of PV (PVPT) and liver parenchyma (LPPT), the peak intensity of PV (PVPI) and liver parenchyma (LPPI); the difference values between HAAT and PVAT (PVAT-HAAT), PVPT and LPPT (LPPT-PVPT), PVPI and LPPI (LPPI-PVPI); and the ratio of PVPI and LPPI (LPPI/PVPI) were recorded.
Outcome and risk factors
The outcome in our study was whether the donor livers were discarded. We defined a discarded liver as any liver that was recovered for transplantation but not ultimately used [25]. Potential risk factors of the donors were collected.
Statistical analysis
Statistical analysis was performed with STATA 11 (StataCorp, College Station, TX, USA) and the SPSS 17.0 package (IBM Corp., New York, USA). All reported P values are two-sided, and P values <0.05 were considered statistically significant. Quantitative variables are expressed as mean ± standard deviation or means (range). Differences between qualitative variables were assessed with a chi-square test or Fisher’s exact test. Differences between quantitative variables were analyzed with t test or Wilcoxon test. Risk factors were analyzed by univariate analysis, and variables with a P value <0.05 were included in a multivariate analysis.
Results
Patient characteristics
From February 2016 to June 2018, 72 consecutive DBD or DCD donors with DUS and CEUS examinations before surgical procurement who underwent LT at our institution. We excluded donors who underwent a DUS/CEUS examination more than 24 hours prior to surgical procurement (n = 5). In total, this study included 67 donors.
Risk factors of liver discarded
Among the 67 eligible donor livers, 15 (22.4%) were discarded due to fibrosis (n = 7), steatosis (n = 6), or fibrosis combined with steatosis (n = 2), and the remaining 52 (77.6%) were used.
The baseline demographics, US and CEUS parameters of the liver discarded and liver used groups were summarized in Tables 1-2- and Tables 1-2. There were no significant differences in the baseline demographics between the liver discarded and liver used groups (P = 0.069–0.991). The liver discarded group showed prolonged SAT of hepatic artery (0.08s vs 0.06s, OR = 2.169, P = 0.008) on DUS, less cases with homogeneous enhancement (40.0% vs 73.1%, OR = 0.243, P = 0.028) on CEUS, more cases with decreased enhancement (53.3% vs 19.2%, OR = 4.800, P = 0.009), and less difference of the peak time between PV and LP (0.5s vs 6.7s, OR = 0.917, P = 0.034).
Donor data of liver discarded and liver used groups
Donor data of liver discarded and liver used groups
Note: Data are expressed as mean±standard deviation, median and range or number (percentage) as appropriate. Donor data were collected prior to surgical procurements. PGD: primary graft dysfunction; BMI: body mass index; DBD: donation after brain death; DCD: donation after cardiac death; CVA: cerebrovascular accident; HBV: hepatitis B virus; CPR: cardiopulmonary resuscitation; ICU: intensive care unit; ALT: serum alanine aminotransferase; AST: aspartate transaminase; ALB: albumin; GGT: glutamyl transpeptidase; ALP: alkaline phosphatase; TB: total bilirubin; INR: and international normalized ratio; DRI: donor risk index.
US and CEUS data of liver discarded and liver used groups
Note: Data are expressed as mean±standard deviation, median and range or number (percentage) as appropriate. RI: resistant index; SAT: systolic acceleration time; HAAT: arrival time of hepatic artery; PVAT: arrival time of portal vein (PV); PVAT-HAAT: difference value between HAAT and PVAT; PVPT: peak time of PV; LPPT: peak time of liver parenchyma; LPPT-PVPT: difference value between PVPT and LPPT; PVPI: peak intensity of PV; LPPI: peak intensity of liver parenchyma; LPPI-PVPI: difference values PVPI and LPPI; PVPI/LPPI: ratio of PVPI and LPPI.
The multivariable analysis showed that donor liver with prolonged SAT of hepatic artery on DUS (OR = 7.304, 95% CI: 1.195–44.655, P = 0.031) and decreased enhancement on CEUS (OR = 2.588, 95% CI: 1.234–5.426, P = 0.012) were independent factors of liver discarded (Fig. 1).
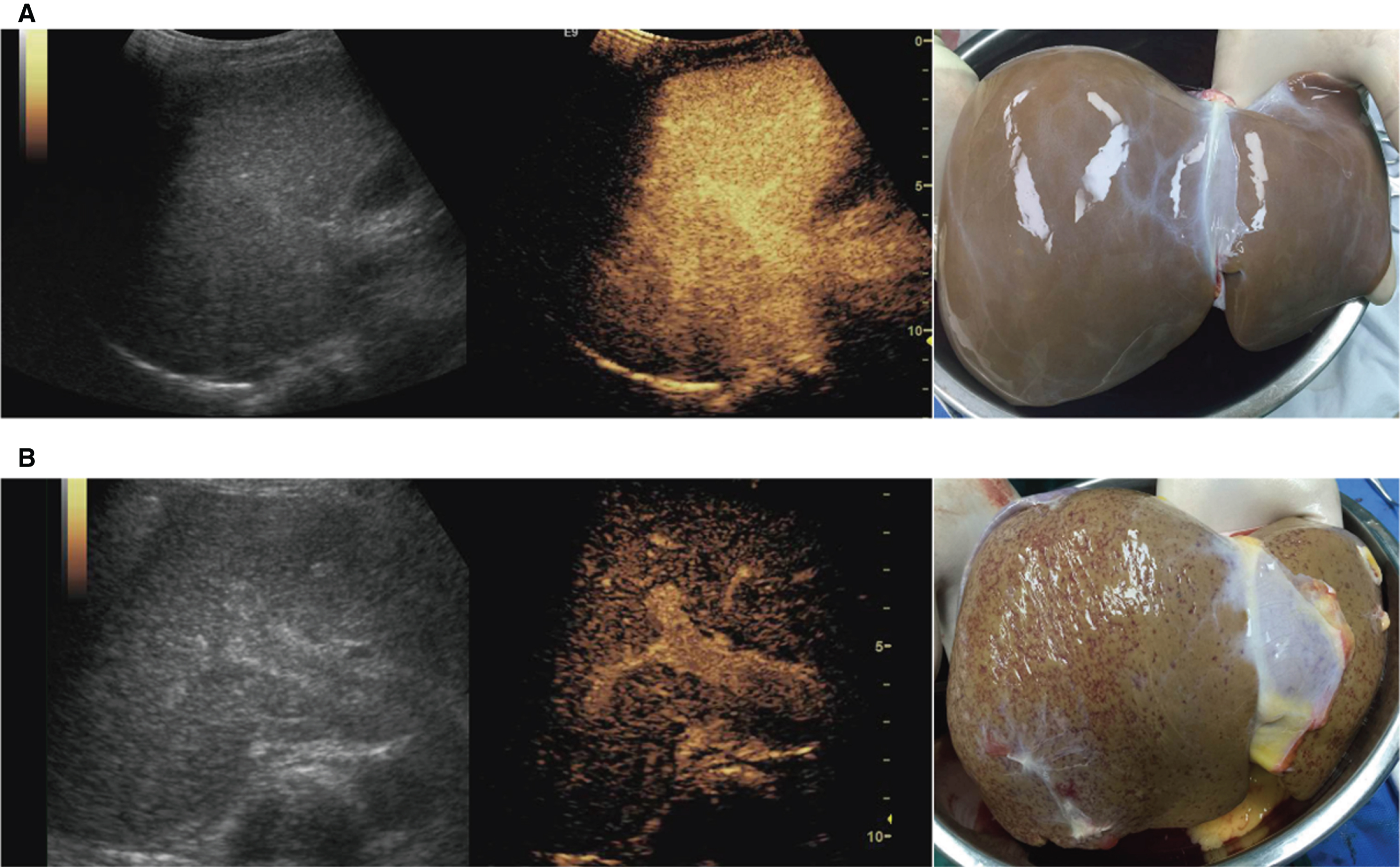
Enhancement at contrast-enhanced ultrasonography (CEUS) on donor livers used and discarded. A: The case of donor liver used showed normal homogeneous enhancement. B. The case of donor liver discarded showed inhomogeneous decreased enhancement with posterior enhancement attenuation.
We conducted this study to analyze the risk factors of liver discarded using clinical and imaging information. We found that the prolonged SAT of hepatic artery on DUS and the decreased enhancement of donor livers on CEUS were independent factors of liver discarded.
The decrease in perfusion of donor livers could be the explanation of the delayed systolic upstroke and the decrease enhancement level. It could be probably due to two reasons: one is the compromised organ perfusion, caused by the irreversible changes of circulatory and respiratory functions in DBD and DCD donors [9, 10]; another is the impaired hepatic microcirculation, caused by the significant constriction of the sinusoidal area in some liver diseases [26]. The status of hypoperfusion in donor livers would cause cellular hypoxia, liver dysfunction, lactic acidosis and hypoxic liver injury, which would compromise the quality of donor livers, and cause donor livers more vulnerable to cell death after liver harvesting and ischemia reperfusion injury [9, 27]. Decreased enhancement on CEUS may be an indicator of more positive strategies and management needed, such as vasoactive drugs and machine perfusion, to improve hemodynamic stability and allograft quality of donor livers [9, 27–30, 9, 27–30].
To the best of our knowledge, our study is the first application of DUS/CEUS to predict the probability of liver discarded before the procurement. DUS/CEUS could be applied as a promising screening tool for high-risk donor livers, especially ECD or marginal allografts. Besides, as we know that procuring high-risk organs must be balanced against the resources that are “wasted” when an organ is found to be unsuitable at procurement laparotomy [7], it also helps decide the activation of a procuring team to optimize human and economic resources.
We should consider the limitations of this study. The major limitation is the small sample size in our study comparing with the previous researches about liver discarded. That might cause that although a variety of donor variables have been reported to be risk factors for liver discarded, such as older donors, liver steatosis, viral hepatitis, and laboratory derangements [3, 6], they didn’t show any correlation in our study. Besides, CEUS isn’t considered as the first-line imaging method for the diagnosis of liver diseases in most western countries due to its invasiveness and additional costs to patients, and its applicability would be limited [31]. Third, though US is highly dependent on the expertise of the operator, we didn’t evaluate the interobserver agreement of the CEUS examinations and evaluations in our study but all were performed by the experienced radiologists. We believe that special training to learn the standard scanning approach and imaging analysis should be essential to avoid incorrect evaluation. Fourth, we didn’t analyze the correlations between CEUS and histopathological findings or between CEUS and other US technique findings, such as elastography, though it must be helpful to provide more convincing support for CEUS in donor evaluation. Fifth, CT and MRI have also been reported to assess liver microcirculation in chronic liver diseases for evaluation of liver function [11, 32], but we didn’t compare CEUS with these two imaging modalities in our study. Further studies should increase the sample size and perform comprehensive evaluation including more information, such as efficiency analysis and comparative studies, to aid transplant physicians in the decision-making process and provide more possibility for the tools in donor evaluation.
In summary, the prolonged SAT of hepatic artery on DUS and the decrease of liver donor in enhancement on CEUS, indicating hemodynamic changes in DBD and DCD donor livers, are independent risk factors of liver discarded. DUS/CEUS could be applied as a promising predictive tool to screen high-risk liver donors.