
Abstract
PURPOSE:
To propose a diagnostic algorithm for improving the diagnosis of atypia of undetermined significance or follicular lesion of undetermined significance (AUS/FLUS) thyroid nodules.
METHODS:
This study retrospectively enrolled 77 consecutive patients with 81 AUS/FLUS nodules who underwent preoperative BRAFV600E mutation analysis. A new diagnostic algorithm was proposed that BRAFV600E mutation analysis for the Fine-needle aspiration cytology specimen was firstly carried out, in which positive BRAFV600E mutation indicated malignancy and classification of the nodules with negative BRAFV600E mutation was further performed based on ultrasound pattern-based risk stratification of American Thyroid Association Guidelines. The diagnostic performance of the new diagnostic algorithm was evaluated.
RESULTS:
The sensitivity, specificity, positive predictive value, negative predictive value, accuracy, and area under the receiver operating characteristic curve (AUROC) of new diagnostic algorithm were 94.6%, 84.0%, 91.4%, 86.9%, 90.1%, and 0.893, respectively. The proposed diagnostic algorithm significantly increased the diagnostic performances (AUROC: 0.893 vs. 0.837 and 0.795), sensitivity (94.6% vs. 71.4% and 75.0%), and accuracy (90.1% vs. 79.0% and 77.8%) compared with BRAFV600E mutation analysis alone and ultrasound pattern-based risk stratification alone (all P < 0.05).
CONCLUSION:
The proposed diagnostic algorithm is helpful for improving the diagnosis of AUS/FLUS nodules, which might be as a routine approach.
Keywords
Introduction
Thyroid cancer is the most common endocrine malignant neoplasm and the incidence has risen significantly whereas the mortality rate is relatively stable at lower levels in recent years [1]. Ultrasound (US) is a preferred diagnostic modality in the preoperative evaluation of thyroid nodules [2–5]. Previous studies have proven that thyroid nodule with suspicious US features, such as taller-than-wide shape, microcalcifications, and irregular margins, are related to a higher risk of malignancy [6]. And US-guided fine-needle aspiration (FNA) cytology examination based on the Bethesda System for Reporting Thyroid Cytopathology (BSRTC) is a standard and effective method to diagnose whether a nodule is malignant or not [7, 8].
However, one of the inevitable limitations in FNA cytology examination for thyroid nodules is atypia of undetermined significance or follicular lesion of undetermined significance (AUS/FLUS) cytology result (i.e. Bethesda category III), of which the recommended risk of malignancy is approximately 15% –30% [9, 10]. But previous some studies have shown that the risk of malignancy in AUS/FLUS nodules is often higher than the BSRTC system evaluated [11, 12]. The repeat FNA is often recommended as for AUS/FLUS nodules, however, approximately 30% of these nodules are diagnosed as AUS/FLUS again [2]. Therefore, the use of FNA alone still is not enough and auxiliary diagnostic methods are needed for diagnosing thyroid AUS/FLUS nodules.
Molecular testing is also recommended for the management of AUS/FLUS nodules [8]. B-type Raf kinase (BRAF) mutation, the most common genetic alteration in thyroid cancer, has a significant specificity in the diagnosis of papillary thyroid carcinoma (PTC). BRAF, a serine-threonine kinase, could be repositioned to the cytomembrane after being combined and activated, which leads to phosphorylation and excessive activation of BRAF and mitogen activated protein kinase (MAPK) signaling pathway and plays a pivotal role in the tumorigenesis and progress of cancer, and BRAFV600E mutation is the most common mutation that results in variation of the valine of the BRAF protein 600-bit codon to glutamate [13–16]. Positive BRAFV600E mutation is highly indicative of thyroid malignancy, and some previous studies have showed that the BRAFV600E test in FNA thyroid nodule specimens increases diagnostic sensitivity and accuracy in the diagnosis of thyroid nodules [17–19]. However, Kim et al. demonstrated that 88.2% thyroid nodules with benign cytology but positive BRAFV600E mutation were malignant [20]. Macerola et al. reported that BRAFV600E mutation had high specificity but were incapable of improving cytological diagnosis of thyroid nodules [21]. As an auxiliary diagnosis method, the validity of BRAFV600E test in AUS/FLUS nodules is still debated.
Meanwhile, there are still some PTC without BRAFV600E mutation (approximately 20% -60%) [17–19]. In addition, it is important to note that the BRAF mutation does not occur in follicular carcinoma, and follicular carcinoma may appear on AUS/FLUS nodule. How to deal with those nodules with negative BRAFV600E mutations remains unclear [16, 21]. Therefore, for AUS/FLUS nodules with negative BRAFV600E mutation, additional methods are needed to furtherly assist diagnosis. Recently, some studies about the 2015 American Thyroid Association (ATA) guidelines have demonstrated the role of US pattern in stratifying the malignancy risk of thyroid nodules [2, 23].
Therefore, we try to establish a new diagnostic algorithm with combination of BRAFV600E mutation analysis and US pattern-based risk stratification of 2015 ATA guidelines to improve the preoperative diagnosis for AUS/FLUS nodules.
Material and methods
Patients
This retrospective study was approved by the ethics committee of the university hospital. Informed consent was waived for this retrospective review. Written informed consents for FNA and preoperative BRAFV600E mutation analysis were obtained from all the enrolled patients before the procedures.
From December 2016 to July 2018, 259 thyroid nodules of 249 patients were diagnosed as AUS/FLUS at cytologic examination from US-guided FNA and undergone preoperative BRAFV600E mutation analysis at our university hospital. Of these patients, 178 nodules of 172 patients were excluded for the reasons as follow: (a) not undergoing subsequent surgery (175 nodules in 169 patients); (b) uncertainty of pathological results (one nodule in one patient); (c) incomplete thyroid US image data (two nodules in two patients). Finally, 77 consecutive patients with 81 surgery-proven AUS/FLUS nodules undergone preoperative BRAFV600E mutation analysis were enrolled (Fig. 1). One AUS/FLUS nodule was found in 73 patients whereas two AUS/FLUS nodules were present in 4 patients. If a patient has more than one nodule, details of the nodule which received FNA and BRAF gene test will be recorded, such as location, size, nodule composition, etc.
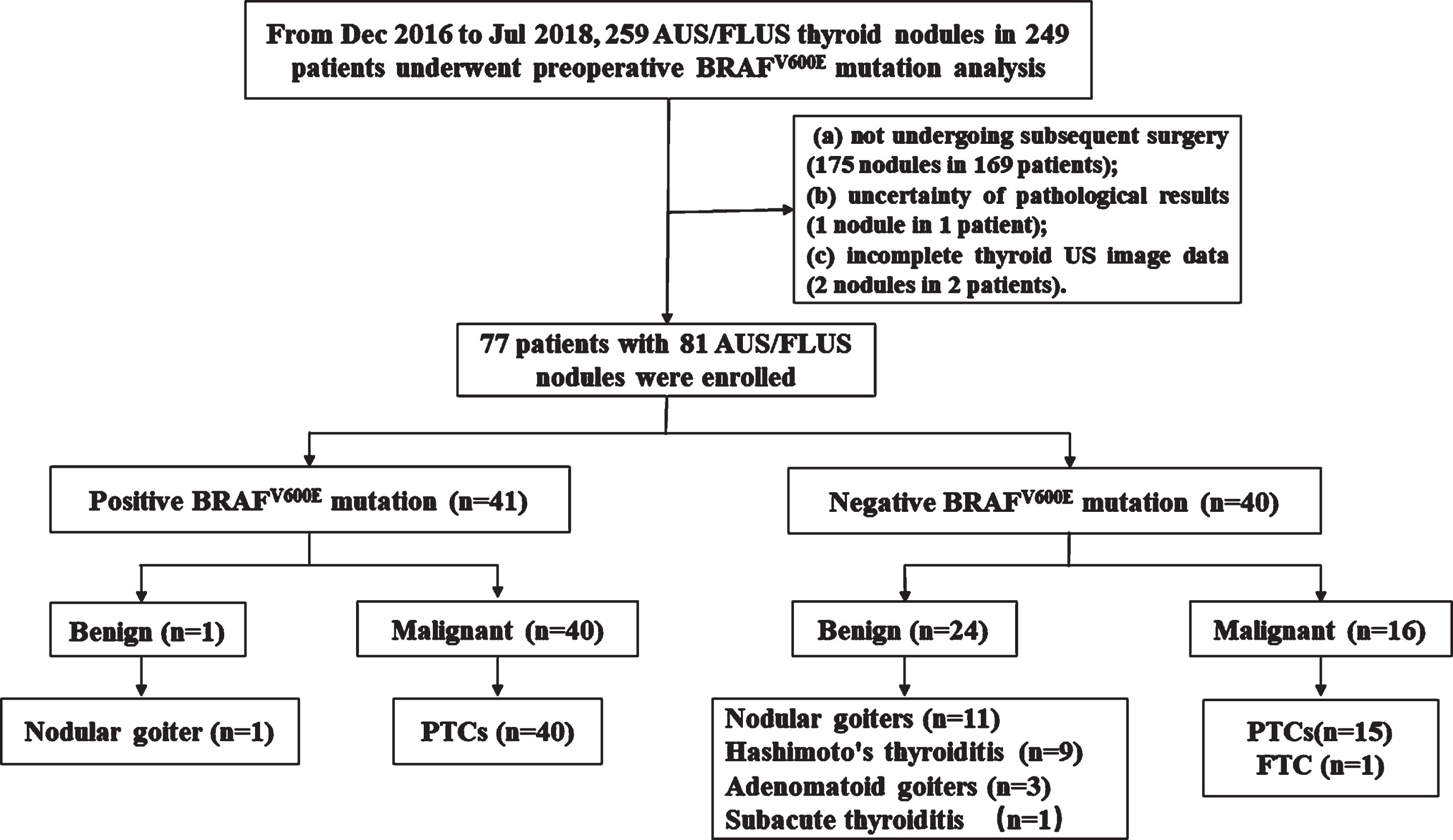
The flowchart of patient selection and the pathologic results in this study. Abbreviations: AUS/FLUS, Atypia of Undetermined Significance or Follicular Lesion of Undetermined Significance; PTC, Papillary Thyroid Carcinoma; FTC, Follicular Thyroid Carcinoma.
US examinations were performed using the Aixplorer US system (SuperSonic Imagine, Aix-en-Provence, France; 5–14 MHz linear transducer), Siemens S2000 (Siemens Medical Solutions, CA, USA; 6–15 MHz linear transducer) or LogiQ E9 (GE Medical Systems, Milwaukee, WI, USA; 6–15 MHz linear transducer). All the preoperative US examinations were performed by one of three radiologists with more than two years’ experience in thyroid US.
The thyroid US examinations were performed referring to the American Institute of Ultrasound in Medicine practice guideline for performing thyroid US, with the patient neck in hyperextension [24]. When thyroid nodule was found, the nodule was observed in transverse and longitudinal sections and the size of the nodule was recorded in three dimensions (anteroposterior, transverse, and longitudinal). The target nodule was positioned in the center of the US screen, and the image settings were optimized to exhibit the target nodules clearly. All the US images of target nodules were stored on the hard disk for further analysis.
FNA procedure and BRAFV600E mutation analysis
US-guided FNA was executed at the target nodule by one of three radiologists. After routine US evaluation, FNA was performed using the 5 mL disposable plastic syringe by the radiologists who had more than five years’ experience in thyroid FNA. The needle was inserted into the target nodule and rapidly moved forth and back in different directions within nodule. After acquisition of the sufficient sample for cytological diagnosis, additional aspiration was performed to obtain material for BRAFV600E mutation analysis. The samples were expelled onto frosted-end glass slides, smeared, and put immediately into 95% alcohol to fix for hematoxylin and eosin (H&E) staining. Cytological diagnosis was based on the BSRTC by one of four pathologists with more than three years’ experience in thyroid cytology. BSRTC diagnostic categories including: non-diagnostic or unsatisfactory (ND/UNS; BSRTC I), benign (BSRTC II), AUS/FLUS (BSRTC III), follicular neoplasm or suspicious for a follicular neoplasm (FN/SFN; BSRTC IV), suspicious for malignancy (SFM; BSRTC V) and malignant (BSRTC VI) [8]. AUS/FLUS cytology results must be confirmed by two independent pathologists.
The BARFV600E test in one of the FNA specimens was performed by fluorescent PCR detection kit (ADx-ARMS, Amoy Diagnostics Co. Ltd) using ARMS technique. The ARMS-qPCR is a very sensitive technique employed for specifically analyzing the BRAFV600E (c.T1799A in exon 15). The PCR reaction is executed by ABI 7500 Fast real-time fluorescence-PCR machine (Applied Biosystems). The mutation type (FAM) and wild-type (VIC) signals of sample are analyzed by the system when the reaction is over.
Images interpretation
Images of all nodules on preoperative US were reviewed and recorded independently by two radiologists who had 15- and 13-years’ experience in thyroid US respectively and were blind to patients’ identities, pathological diagnosis, and molecular results. In case of disagreement in the interpretation between the two radiologists, a third experienced radiologist with more than 20-years’ experience in thyroid US reviewed these images and made the final decision. The US characteristics of the target nodules (including compositions, echogenicity, margins, shape, calcifications, and extrathyroidal extension) were interpreted. Compositions were classified into solid, spongiform, or cystic proportion. Echogenicity was classified into anechoic, hyperechoic, isoechoic, or hypoechoic. Margin was classified into regular or not. Shape was defined as wider-than-tall or taller-than-wide. And calcification was described in microcalcifications, macrocalcifications or without calcification. According to the ATA guidelines, different US patterns in thyroid nodules were interpreted as follows: i. high suspicion nodules, solid hypoechoic nodule or solid hypoechoic component of a partially cystic nodule with at least one suspicious feature; ii. intermediate suspicion nodules, hypoechoic solid nodule with smooth margins without any suspicious features; iii. low suspicion nodules, hyper- or isoechoic solid nodule, or partial cystic nodule with eccentric solid areas without dubious characteristics; iv. very low suspicion nodules, spongiform or partial cystic nodules without any US features described above [2].
The new proposal diagnostic algorithm
The new proposal diagnostic algorithm of AUS/FLUS nodules is shown in Fig. 2. BRAFV600E mutation analysis was performed on AUS/FLUS nodules firstly, and the nodules with positive BRAFV600E mutation were considered malignant; the nodules with negative BRAFV600E mutation were subsequently classified by US pattern-based risk stratification with ATA guidelines.
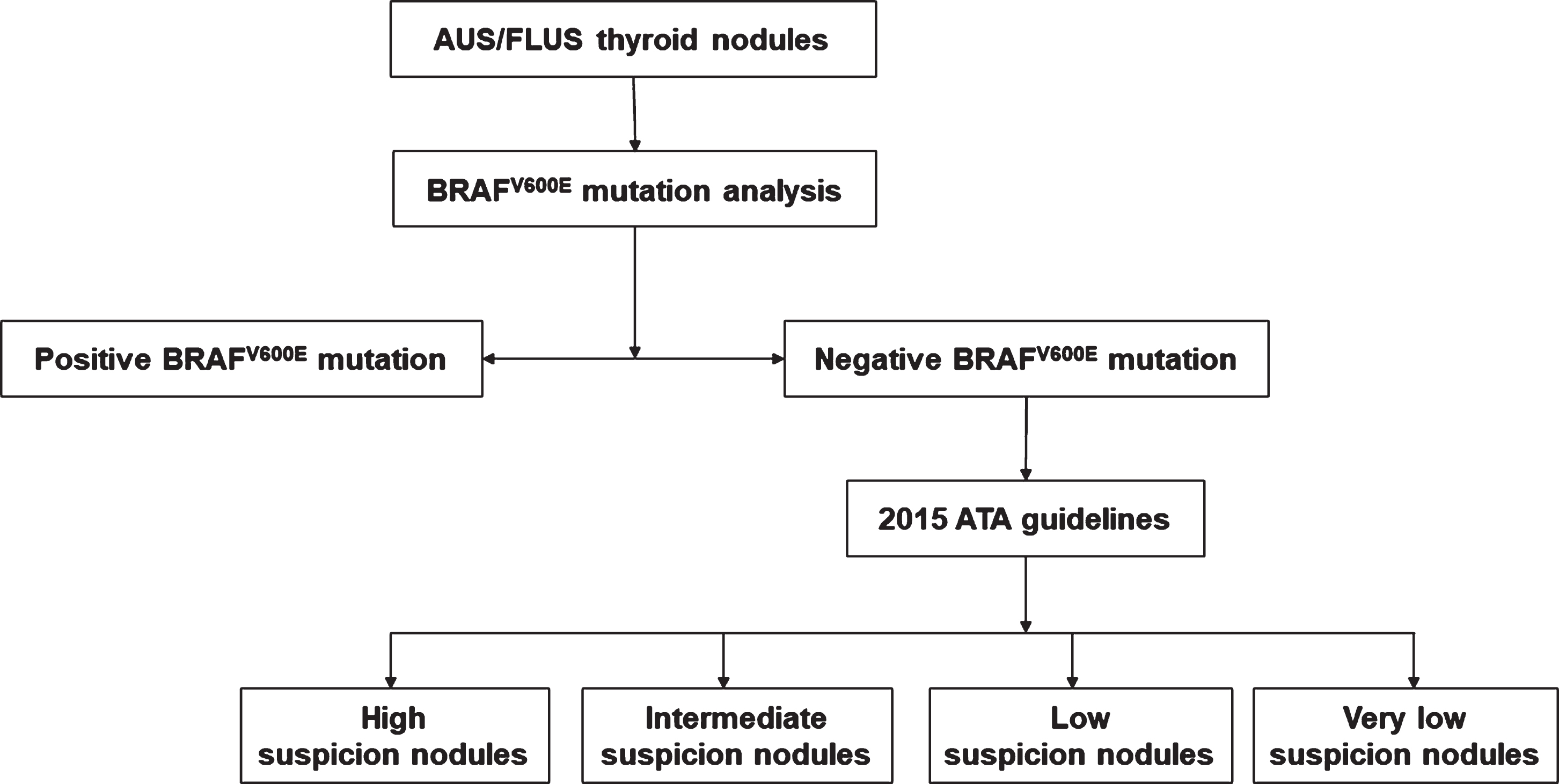
The diagnostic algorithm of thyroid nodules with AUS/FLUS cytology. Abbreviations: AUS/FLUS, Atypia of Undetermined Significance or Follicular Lesion of Undetermined Significance; ATA, American Thyroid Association.
The data analyses were performed by the SPSS software (Version 23.0; SPSS, Chicago, IL) and MedCalc software (Version 15.6). Mean±standard deviation was calculated for continuous variables if they coincided with normal distribution. Comparison of continuous variables was performed by independent-samples t-test, and the Fisher’s exact probability test or χ2 test for categorical variables. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated by the McNemar test or χ2 test. The best cutoff value for different US pattern-based risk stratification with ATA guidelines was obtained from the receiver operating characteristic (ROC) curves. The diagnostic performances for BRAFV600E mutation alone and the new diagnostic algorithm were performed by the area under ROC (AUROC) curves and were compared. All significance tests with a P value less than 0.05 were considered statistically significant.
Results
Pathologic diagnosis and basic characteristics of the AUS/FLUS nodules
The 81 AUS/FLUS thyroid nodules in 77 patients included 56 (69.1%) malignant nodules and 25 (30.9%) benign nodules. Of the 56 malignant nodules, 55 were PTCs and the remaining one was follicular thyroid carcinoma (FTC). The 25 benign nodules were 12 nodular goiters, 9 Hashimoto nodules caused by lymphocytic thyroiditis, 3 adenomatous goiters, and 1 subacute thyroiditis nodule (Fig. 1).
The basic characteristics of the patients and the nodules are shown in Table 1. The average age of all patients was 51±13 years old and the mean size of all nodules was 12±7 mm. The significant characteristics for identification between benign and malignant nodules were nodules size (P < 0.05). The malignant nodules were more frequently found in smaller nodules.
The basic characteristics of patients and AUS/FLUS nodules
The basic characteristics of patients and AUS/FLUS nodules
Abbreviations: AUS/FLUS, atypia of undetermined significance or follicular lesion of undetermined significance; No., number. # Data are means±standard deviations. *Indicates statistically significant difference between the two group (P < 0.05).
Of the 81 AUS/FLUS nodules, positive BRAFV600E mutation was found in 41 nodules, including 40 (97.6%, 40/41) malignant nodules and 1 (2.4%, 1/41) benign nodule. Of the 56 malignant nodules, 40 (71.4%, 40/56) nodules showed positive BRAFV600E mutation. Negative BRAFV600E mutation was found in the remaining 40 AUS/FLUS nodules, including 24 (60.0%, 24/40) benign nodules and 16 (40.0%, 16/40) malignant nodules. The sensitivity, specificity, PPV, NPV, accuracy, and AUROC of positive BRAFV600E mutation alone were 71.4%, 96.0%, 97.6%, 60.0%, 79.0%, and 0.837, respectively.
US pattern-based risk stratification with ATA guidelines in AUS/FLUS nodules
US features of all AUS/FLUS nodules and those with negative BRAFV600E mutation are shown in Table 2. Of the US features, margin, calcification, and taller-than-wide shape were associated with malignancy in all AUS/FLUS nodules and those with negative BRAFV600E mutation (all P < 0.05). US feature of solid composition was associated with malignancy in all nodules, but not in those with negative BRAFV600E mutation. The ROC curve demonstrated that the best cutoff of different US patterns was high suspicion US pattern. The sensitivity, specificity, PPV, NPV, accuracy, and AUROC of US pattern-based risk stratification were 75.0%, 84.0%, 91.3%, 60.0%, 77.8%, and 0.795, respectively, for diagnosis of all the AUS/FLUS nodules.
The US features of all AUS/FLUS nodules and those with negative BRAFV600E
mutation
The US features of all AUS/FLUS nodules and those with negative BRAFV600E mutation
Abbreviations: US, ultrasound; AUS/FLUS, atypia of undetermined significance or follicular lesion of undetermined significance. # Data are mean±standard deviations. *Indicates statistically significant difference.
For AUS/FLUS nodules with negative BRAFV600E mutation, the US risk classifications of ATA categories were classified as very low suspicion in 3 (7.5%), low suspicion in 8 (20.0%), intermediate suspicion in 12 (30.0%), and high suspicion in 17 (42.5%), respectively. In the 16 thyroid malignant nodules with negative BRAFV600E mutation, 6.3% (1/16) were low suspicion, 12.5% (2/16) intermediate suspicion, and 81.2% (13/16) high suspicion (Fig. 3); whereas, in the subgroup of benign nodules, 12.5% (3/24) were very low suspicion, 29.1% (7/24) low suspicion, 41.7% (10/24) intermediate suspicion, and 16.7% (4/24) high suspicion. The malignant rates of very low suspicion, low suspicion, intermediate suspicion, and high suspicion were 0, 12.5% (1/8), 16.7% (2/12), and 76.5% (13/17), respectively.

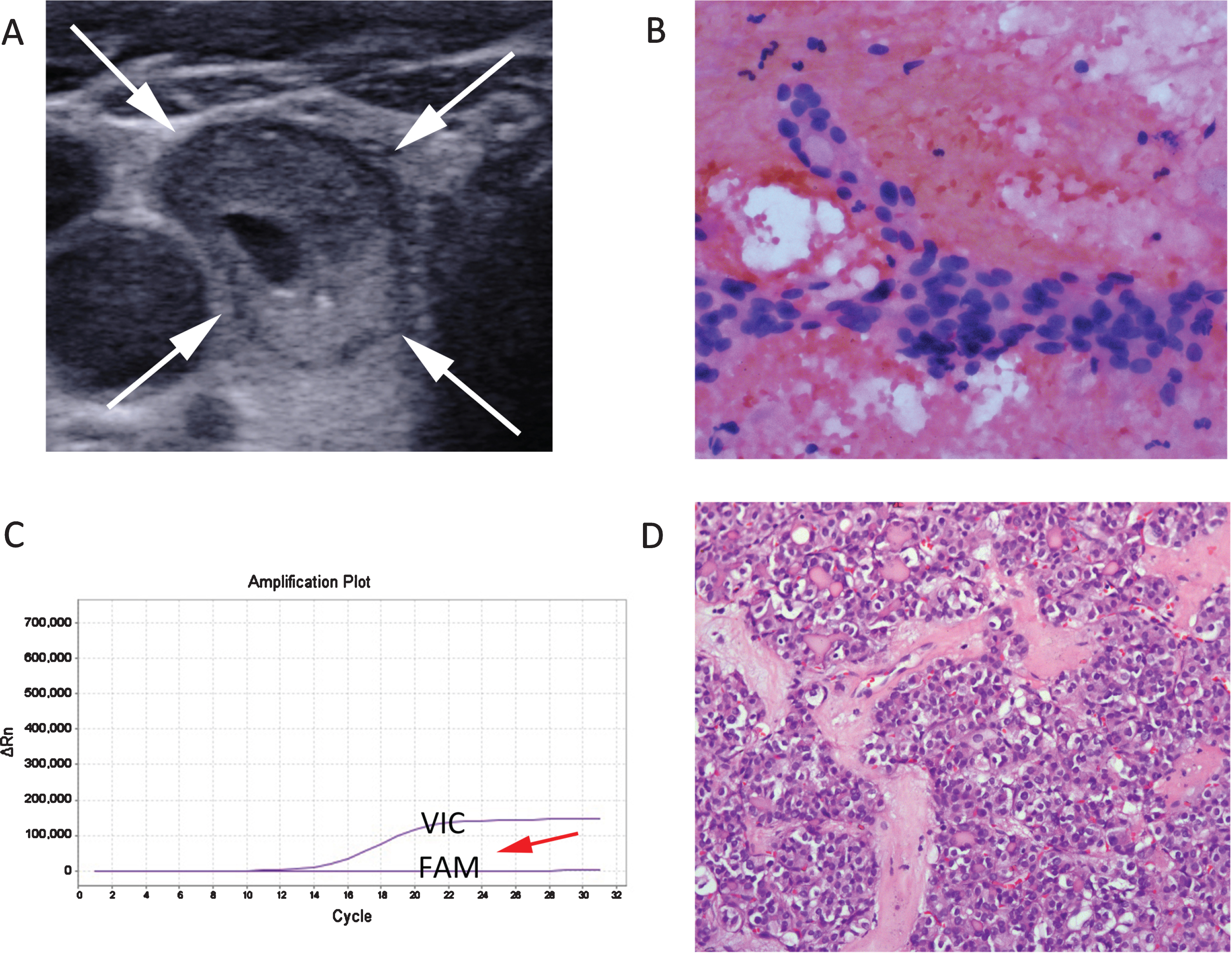
A 57-year-old woman with PTC. (A) The 10 mm thyroid nodule appears solid component, hypoechoic, irregular margin on US and is diagnosed as suspicious US pattern using 2015 ATA guidelines. (B) FNA cytology shows a few follicular epithelial cells with architectural atypia and eosinophilic changes under the background of lymphocytes and colloid and the nodule is diagnosed as AUS/FLUS (Hematoxylin-eosin stain; original magnification,×400). (C) BRAFV600E mutation analysis shows negative result by using ARMS-qPCR in FNA cytology specimens [The FAM signal does not rise (red arrow) when the VIC signal rises in the orange amplification plot]. (D) Histologic specimen confirms diagnosis of PTC (Hematoxylin-eosin stain; original magnification,×200).
According to the new diagnostic algorithm (Fig. 2), when positive BRAFV600E mutation or high suspicion US pattern was applied as the diagnostic criterion, the sensitivity, specificity, PPV, NPV, accuracy, and AUROC were 94.6%, 84.0%, 91.4%, 86.9%, 90.1%, and 0.893, respectively. The new diagnostic algorithm significantly increased AUROC (0.893 vs. 0.837 and 0.795), sensitivity (94.6% vs. 71.4% and 75.0%), and accuracy (90.1% vs. 79.0% and 77.8%) compared with BRAFV600E analysis alone and US pattern-based risk stratification alone (all P < 0.05) (Table 3).
Comparison of the diagnostic performance of BRAFV600E mutation analysis
alone, US pattern-based 2015 ATA guidelines, and the new diagnostic algorithm for
AUS/FLUS nodules
Comparison of the diagnostic performance of BRAFV600E mutation analysis alone, US pattern-based 2015 ATA guidelines, and the new diagnostic algorithm for AUS/FLUS nodules
Abbreviations: US, Ultrasound; ATA, American Thyroid Association; AUS/FLUS, Atypia of Undetermined Significance or Follicular Lesion of Undetermined Significance; PPV, Positive Predictive Value; NPV, Negative Predictive Value; AUROC, Area Under the Receiver Operating Characteristic Curve.
Of the misdiagnosis analysis, the rates of false-positive and false-negative were 8.6% (5/58) and 13.1% (3/23), respectively. Four benign nodules in the high-suspicion group included one nodular goiter which showed irregular margin, microcalcifications, and 'taller-than-wide shape, and three Hashimoto nodules. One nodule with positive BRAFV600E mutation was confirmed to be nodular goiter. Three nodules in the low-suspicion and intermediate-suspicion groups were confirmed to be one follicular variant of PTC (Fig. 4) and two PTCs, respectively.
A 67-year-old woman with follicular variant of PTC. (A) The 22 mm thyroid nodule appears mixed cystic and solid component, hypoechoic, regular margin, wider-than-tall shape, and macrocalcification on US and is supposed to be low suspicion by 2015 ATA guidelines. (B) FNA cytology exhibits a few follicular epithelial cells with architectural atypia under the background of colloid and blood and the nodule is diagnosed as AUS/FLUS (Hematoxylin-eosin stain; original magnification, ×400). (C) BRAFV600E mutation analysis shows negative result by using ARMS-qPCR in FNA cytology specimens [The FAM signal does not rise (red arrow) when the VIC signal rises in the purple amplification plot]. (D) Histologic specimen confirms diagnosis of follicular variant of PTC (Hematoxylin-eosin stain; original magnification, ×200).
Due to the heterogeneous characteristics of AUS/FLUS nodules, the appropriate management of these nodules is a major challenge for clinicians. For these nodules, supplemental diagnostic procedures are necessary to clarify the diagnosis for avoiding unnecessary repeat FNA and diagnostic thyroidectomies.
In this study, the incidence rates of BRAFV600E mutations and malignancy in the AUS/FLUS nodules were 50.6% (41/81) and 71.4% (40/56), respectively. This result was consistent with the results of previous studies that the incidence rate of BRAFV600E mutation in PTC is approximately 40% -80% [14, 17–19]. Of these AUS/FLUS nodules with preoperative positive BRAFV600E mutation, 2.4% (1/41) was surgery-proven benign. It is well-known that BRAFV600E mutation occurs exclusively in PTC and PTC-derived anaplastic or poorly differentiated carcinomas. The surgical tissue sample of this case was tested for BRAFV600E mutation analysis, and BRAFV600E mutation was not detected. This result was considered as the false-positive BRAFV600E mutation which is a result of the overly sensitive assay [25]; 97.6% (40/41) were malignant, which resembled the results of a previous study that BRAFV600E mutation analysis was beneficial in diagnosing malignant nodules [14, 20]. Therefore, preoperative BRAFV600E mutation analysis plays an important role in detecting malignancy among the AUS/FLUS nodules and should be regarded as the first step for management of these nodules.
Another issue is emerging that is how to deal with the AUS/FLUS nodules with negative BRAFV600E mutation, which accounted for 49.4% (40/81) AUS/FLUS nodules in the current study. This study showed that calcification, irregular margins, and taller-than-wide shape are significative in the differentiation of benign and malignant nodules in AUS/FLUS nodules with negative BRAFV600E mutation. This result was in line with the previous studies that calcification, lobulated or irregular margins, and taller-than-wide shape were the common findings associated with malignant thyroid nodules [26, 27]. However, single US feature has a relatively unsatisfactory predictor for the risk of thyroid nodules. Thus, we try to use US pattern-based system of 2015 ATA guidelines for stratifying the risk of AUS/FLUS nodules with negative BRAFV600E mutation. The malignant rate of those nodules with high suspicion US feature in our study was 76.5% (13/17), which was consistent with that reported in the ATA guidelines [2]. In other words, the 2015 ATA US pattern-based risk stratification can help us detect most malignant nodules from negative BRAFV600E mutation nodules when the cut-off value was high suspicion US pattern. Based on the results, more beneficial diagnostic procedures, such as lateral lobectomy, should be considered for the AUS/FLUS nodules when BRAFV600E mutation is negative and ATA US pattern is high suspicion.
Using the combination of positive BRAFV600E mutation in nodules and high suspicion US pattern in negative BRAFV600E mutation nodules, the new proposal diagnostic algorithm could get an increased accuracy and AUROC (90.1% and 0.893) in comparing with BRAFV600E test alone and US pattern-based 2015 ATA guidelines alone for diagnosis of AUS/FLUS nodules, which indicated that the new diagnostic algorithm can further improve the diagnosis of AUS/FLUS nodules, which might be as a routine approach for management of AUS/FLUS nodules. In this proposal diagnostic algorithm, the rates of false-positive and false-negative were 8.6% and 13.1%. Of the false-positive results, one nodule with three suspicious US features was nodular goiter and three nodules with one suspicious US feature were Hashimoto nodules caused by lymphocytic thyroiditis. For the nodular goiter, the microcalcification may be related to the formation of calcium oxalate crystals [28, 29], and the irregular margin and taller-than-wide shape were possibly related to the hemorrhage, necrosis, or colloid accumulation progressions in the nodules [30]. Oppenheimer et al. reported that some of Hashimoto’s thyroiditis nodules resembled malignant nodules on US [31], which was a challenge for radiologists and clinicians [32, 33]. Of the false-negative results, two nodules with intermediate suspicion US pattern were PTCs and one nodule with low suspicion US pattern was follicular variant of PTC. The relatively benign US characteristics of these nodules led to the misdiagnosis [34, 35].
This study had several limitations. First, all enrolled patients in this study underwent surgical resection, but we not included those not surgery-proven AUS/FLUS nodules with negative BRAF, without high suspicious US pattern or rapid growth during follow-up. It inevitably leads to selection bias in this retrospective study design. And, this may be one reason for the malignant rate (69.1%, 56/81) of this study was higher than that of normal population of AUS/FLUS nodules. However, this factor was hard to be avoided since the reference standard for AUS/FLUS had to be pathological results after surgery. Second, after applying the new proposed diagnostic algorithm, the follicular variant of the PTC with positive BRAF can be found out, and some the follicular variant of the PTC without positive BRAF and follicular carcinoma with highly suspicious US pattern can be ruled in. However, follicular carcinomas and follicular variant of PTC with negative BRAF do not show highly suspicious US pattern being classified as benign in this diagnostic method, which will lead to false negatives in the clinical practice. Thus, it is necessary to add some potential diagnostic approaches for follicular-patterned carcinomas such as shear-wave elastography or PAX8/PPARγ rearrangement test to this diagnostic algorithm for further ruling in the rest of carcinomas in the further studies [36–38]. In addition, contrast-enhanced ultrasound with the perfusion analysis of the arterial phase may provide some useful parameters to help determine malignancy and benignity of follicular-patterned thyroid lesions [39]. Third, our study included some suspicious thyroid nodules smaller than 10 mm that were subjected to the biopsy and surgery procedure. These patients actively sought for the FNA and further examination because of the psychological burden. In addition, some patients with thyroid microcarcinoma presented clinically evident metastases or local invasion, who were required for cytological diagnosis and treatment in clinical practice. Finally, this was a single-center and limited sample study thus the results should be validated in future multi-center and larger series studies.
In conclusion, preoperative BRAFV600E mutation analysis with FNA specimen is helpful for improving the diagnosis of AUS/FLUS nodules. Highly suspicious US pattern on 2015 ATA guidelines further improves the diagnosis of AUS/FLUS nodules with negative BRAFV600E mutation. The proposed diagnostic algorithm with combination of preoperative BRAFV600E mutation analysis with FNA specimen and US pattern-based risk stratification with 2015 ATA guidelines can effectively diagnose for AUS/FLUS nodules, which might be recommended as a routine approach for diagnosis of AUS/FLUS nodules.
Conflict of interest
The authors do not have any conflicts of interest to declare.
Footnotes
Acknowledgments
This work was supported in part by the National Natural Science Foundation of China (Grants 81671695, 81725008, and 81927801), Shanghai Municipal Health Commission (Grants 2019LJ21 and SHSLCZDZK03502), and the Science and Technology Commission of Shanghai Municipality (Grants 19441903200, 18441905500 and 19DZ2251100).