
Abstract
OBJECTIVE:
To investigate prostate cancer detection rate of different biopsy protocols in different PSA value groups in rural China.
METHODS:
A total of 186 patients underwent contrast-enhanced ultrasound (CEUS) in order to determine the puncture target prior to biopsy were enrolled in this retrospective study. All patients underwent 12-core SB combined with CEUS-TB. The biopsy results of different biopsy protocols were compared in patients with stratification by PSA value.
RESULTS:
Among the 186 patients underwent prostate biopsy, the histopathologic results revealed prostate cancer (PCa) in 117 cases (62.9%) and benign lesions in 69 cases (37.1%). The PCa detection rate between 8-core SB and 12-core SB showed no significant difference in PSA 4–10 ng/ml group, while the 12-core SB was significantly higher than CEUS-TB (44.9% versus 32.7%, P = 0.01). In PSA 10–20 ng/ml group, the significant difference was not seen between SB and CEUS-TB (50.0% versus 45.7%, P = 0.15). As for PSA greater than 20 ng/ml group, the PCa detection rate by SB was higher than CEUS-TB, but showed no statistically significance (79.1% versus 76.9%, P = 0.15). In the overall patients, the biopsy core positive rate of CEUS-TB was significantly higher than SB (97% versus 55.5% and 28.5%, P = 0.0001).
CONCLUSION:
The flexible use of SB combined with CEUS-TB can reduce the number of biopsy cores in higher PSA groups. It has clinical importance in the detection of PCa in different PSA value groups in rural China.
Prostate cancer (PCa) is one of the common malignancies of male urogenital system [1]. In worldwide, (PCa) counted for 27% of new cases and 9% of death for male patients who were diagnosed as malignant diseases [2]. Although incidence of (PCa) in China is relative lower than that in western countries, it is increasing in recent years due to prolonged average life expectancy and western life style [3, 4].
Early diagnosis of (PCa) is relative difficult because of its occult symptoms. Most of patients are found at advanced or metastatic disease when they are diagnosed, subsequently resulting in poor outcome. Therefore, early diagnosis of (PCa) is critical to improve quality of life and prognosis of patients [5].
At present, digital rectal examination (DRE), serum prostate specific antigen (PSA) and transrectal ultrasound are the routine methods for (PCa) screening, while it is difficult to discriminate benign diseases such as prostatitis and benign prostatic hyperplasia. Transrectal ultrasound guided prostate biopsy (TRUS) remains the golden standard to diagnose (PCa) [6]. However, false negative rate of traditional 6-core biopsy method was over 30%. For 10-core or 12-core systemic biopsy (SB), the false negative rate was also approximately 20% [7].
It has been reported that contrast-enhanced ultrasound (CEUS) has relative high sensitivity and specificity for (PCa), suggesting that CEUS-targeted biopsy could improve (PCa) detection rate and reduce the number of biopsy cores [8]. the aim of this study is to compare the diagnostic accuracy of SB and CEUS-targeted biopsy in order to reduce the number of biopsy cores in different PSA value groups in rural China.
Patients and methods
Patients
We retrospectively analyzed 186 patients who underwent prostate biopsy in our department from July 2013 to July 2016. All patients approved by the institutional review board were enrolled retrospectively in the present study. All of them are Chinese men, local residents of rural areas in Chongming island. The inclusion criteria for biopsy were: 1) abnormally elevated PSA value (>4 ng/ml); 2) gradually increased PSA value by 0.75 ng/ml/year; or 3) positive DRE or magnetic resonance imaging (MRI) result. Patients were exclude as receiving any treatment before examination.
Conventional transrectal ultrasonography of prostate
The ultrasound examinations were performed by commercially available equipment (LOGIQ® E9 with IC5-9-D probe, GE, USA, with frequency of transducer from 5 to 9 MHz). The patient was in the left decubitus position, and transrectal ultrasound showed the largest cross-section of the prostate. The left and right diameters of the prostate were measured. Then to rotate probe 90 degrees to display the largest longitudinal section of the prostate. According to the formula, the prostate volume can be obtained by left and right diameter×anterior and posterior diameter×up and down diameter×0.52. The PSA density (PSAD) value was obtained by dividing PSA value by prostate volume.
Procedure of contrast-enhanced ultrasound guided transrectal prostate biopsy
The ultrasound examinations were performed by commercially available equipment (LOGIQ® E9 with IC5-9-D probe, GE, USA, with frequency of transducer from 5 to 9 MHz). Ultrasonic contrast agents SonoVue® (Bracco, Italy) was used in present study. The contrast agents SonoVue was prepared in a standard fashion and 2.4 ml was administered as a bolus via an antecubital vein of the left arm, followed by a flush with 5 ml of 0.9% sodium chloride injected. Scanning was started after the microbubbles reached the prostate capsule, using a standard sequence of transverse imaging from base to apex to identify significant enhanced region. If so, the region would be the position for CEUS-targeted biopsy (CEUS-TB). If not, 12-core SB was performed (Fig. 1).
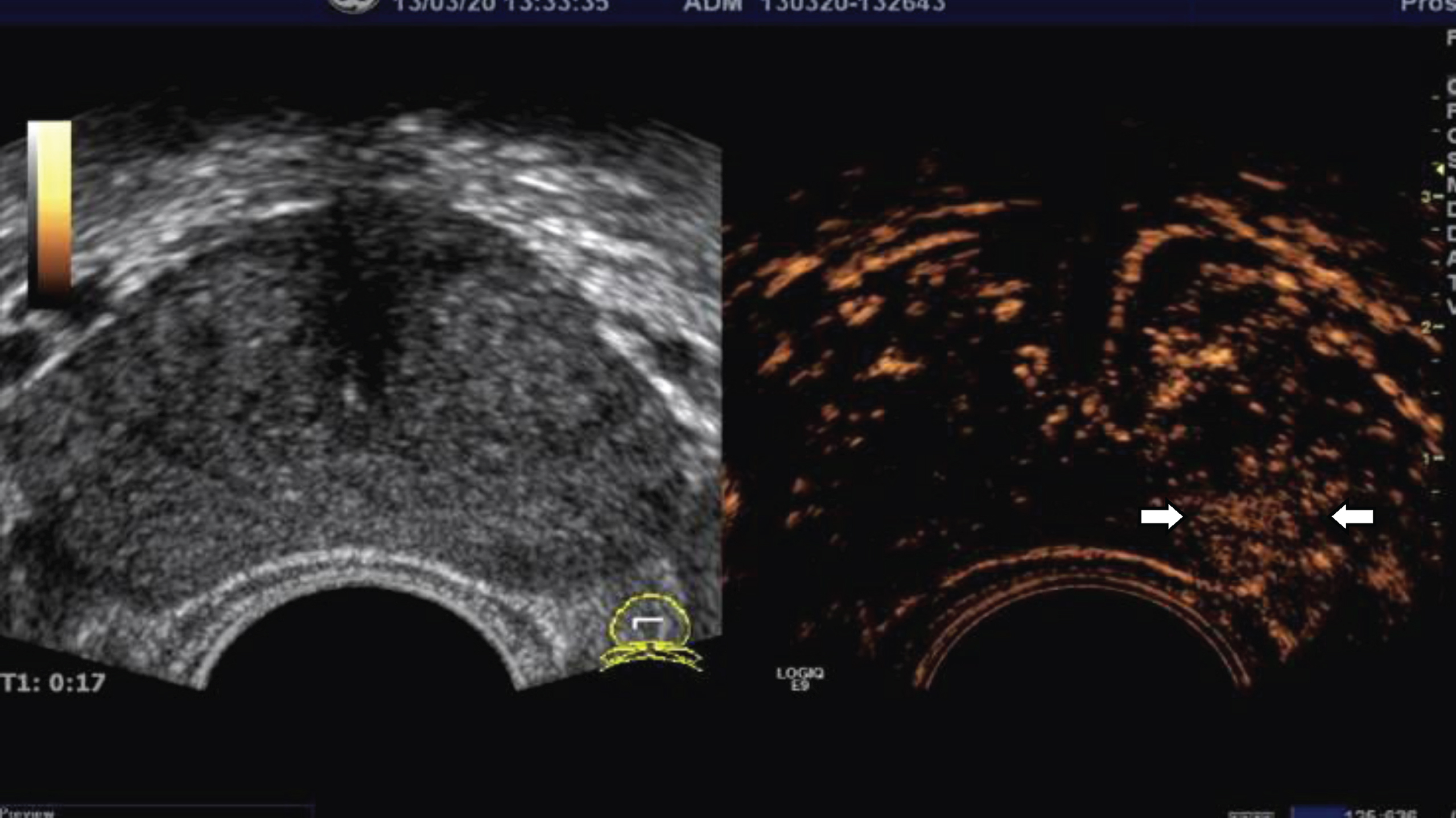
Shows significant enhanced region(arrow); At the early stage of enhancement, a significant enhancement region was found in the left peripheral zone.
After the completion of the CEUS examination, the ultrasound guided transperineal prostate biopsies were performed using a MylabTMTwice (EsaoteSpA, Genoa, Italy) scanner with a TRT33 biplane probe by two radiologists. Both the SB and CEUS-TB were taken with a spring-loaded biopsy gun (BARD Maxcore, Covington, GA). Patients were divided into 3 groups according to the value of PSA. In all groups, the area with “fast in, fast out and significant enhancement” on contrast-enhanced ultrasound was used as the CEUS-TB point (one or two cores). For patients without significant enhancement area, 12-core SB was performed (five cores distributed equably at in peripheral zone and one core in transition zone in bilateral prostate). During the biopsy, the probe was rotated and angulated to the desired sagittal plane and the needle was introduced on the same plane. After the biopsy gun was fired, the probe was switched to a convex transducer to confirm the location of biopsy needle (Fig. 2). Each biopsy core was referred in micro-biopsy cassette immediately and labeled to identify the location.

Shows the position of the biopsy needle(arrow); The needle was located in the early significant enhancement area.
All samples of prostate biopsy were reviewed by a senior pathologist with specialty of urology blinded to patients’ information. Each biopsy core was diagnosed as benign prostatic hyperplasia, inflammation, prostatic intraepithelial neoplasia and PCa with assigning Gleason score.
Statistical analysis
All statistical analyses were performed by SPSS 17.0 software (SPSS, Chicago, IL). The quantitative data were expressed as means±standard deviation. The detection rate of PCa in each group was tested by non-paired Chi-square test. The detection rate and the biopsy core positive rate of PCa by SB and CEUS-TB in each group were tested by McNemar test. P-value < 0.05 was considered as statistically significant.
Results
Characteristics of the patients
The mean age of 186 participants was 76.5±6.6 y, and with mean serum PSA value of 32.1±27.48 ng/ml. Among them, there were 49 cases with PSA value of 4–10 ng/ml (low PSA), 46 cases with 10–20 ng/ml (median PSA), and 91 cases with PSA more than 20 ng/ml (high PSA). In 186 patients, 117 patients were diagnosed as PCa (62.9%), 69 cases were diagnosed as benign prostate diseases (37.1%) which including 60 cases with benign prostatic hyperplasia, five cases with inflammation and four cases with prostatic intraepithelial neoplasia. The PCa detection rate of the high PSA group is significantly higher than that of the median PSA and low PSA groups (Table 1).
The characteristic of patients underwent prostate biopsy
The characteristic of patients underwent prostate biopsy
PSA: prostate specific antigen; PSAD: prostate specific antigen density; PCa: prostate cancer. #Compared with the median and low PSA group, P < 0.01.
We extracted the first, third and fifth core in peripheral zone and one core in transition zone in bilateral prostate from 12 needles as a 8-core SB.
In low PSA group, the PCa detection rate of 12 core-SB was 44.9%, and the CEUS-TB was 32.7%. There was significant difference between the two methods, and the detection rate of 12 core-SB was better than that of CEUS-TB. The difference was not seen between the 12-core SB (44.9%) and 8-core SB (38.8%). The biopsy core positive rate of CEUS-TB was significantly higher than 8-core SB and 12-core SB (P = 0.0001).
In median PSA group, the difference was not seen among the 8-core SB, 12-core SB and CEUS-TB in PCa detection. The biopsy core positive rate of CEUS-TB was significantly higher than 8-core SB and 12-core SB (P = 0.0001).
In high PSA group, 72 patients were diagnosed as PCa by 8-core SB, and consistent with the 12-core SB. For CEUS-TB, 70 PCa were diagnosed. There was no statistically difference. The biopsy core positive rate of CEUS-TB was significantly higher than 8-core SB and 12-core SB (P = 0.0001) (Table 2, 3).
Comparison of the prostate cancer detection rate between the CEUS-TB and the SB
Comparison of the prostate cancer detection rate between the CEUS-TB and the SB
*Compared with 12-core SB, P = 0.01; #Compared with 8-core SB, P > 0.05
Comparison of the biopsy core positive rate between the CEUS-TB and the SB
*P-value: compared with 8-core SB and 12-core SB, P = 0.0001; #compared with 8-core SB, P > 0.05
Since 1989, sextant biopsy guided by transrectal ultrasound has been used to diagnose PCa as the standard procedure [9]. Along with the investigations of PCa screening and diagnosis, it was thought that the diagnostic sensitivity of sextant biopsy could be improved by increasing number of core samples because of variant prostate volume of patients might interfere sensitivity of sextant biopsy [10]. Ojewola et al. found that for patients with PSA value of 4.0–10.0 ng/ml, PCa detection rate of 10-core SB was 33%, higher than sextant biopsy [11]. However, some other studies suggested that simply increasing the number of biopsy cores did not significantly increase PCa detection rate [12, 13]. There was no significant difference in the positive rate between the sextant biopsy and the extended biopsy for patients with higher PSA value,
In this retrospectively study, the PCa detection rate between 8-core and 12-core method has no statistically significance in low PSA group, as well as the biopsy core positive rates. Therefore, simply increasing the number of biopsy cores might not improve the PCa detection rate in low PSA group. Similar results were also reported by other researches. Abd et al. found that detection rates of 12-core and 8-core methods were 51.2% and 49.2% [14], respectively. As for the median PSA group, the detection rates of PCa of 8-core and 12-core method were similar, with the positive rate of core samples were higher in 8-core method compared with 12-core, which might suggest that 8-core method could be enough for those patients to avoid unnecessary puncture.
SonoVue is a vascular contrast agent and so only useful in cases of prostate cancer with hypervascularization. CEUS using SonoVue is an off label use for prostate imaging considering the EFSUMB guidelines [15]. Although CEUS is blood pool imaging, the effect is not good without high enhancement, but abnormal perfusion area is found through software analysis [16, 17]. CEUS can improve diagnostic capability of ultrasound by displaying tumor vessel, and is now being widely investigated [18]. CEUS can identify the location of PCa and thus achieve targeted biopsy by imaging prostate micro-vessels [19].
In this study, the PCa detection rate of CEUS-TB in low PSA group was similar with 8-core SB, while was inferior than 12-core SB, which suggested that for those patients, SB remains the standard procedure. As for median and high PSA groups, detection rates of CEUS-TB, 8-core SB and 12-core SB were similar, thus CEUS-TB could reduce not only number of biopsy cores but also patients’ suffering, while did not interfere sensitivity of PCa diagnosis. Similar result was also reported. Sharma et al. showed that CEUS with reduced number of core biopsy showed similar PCa detection rate with SB [20]. Halpern et al. found that CEUS can reduce the number of cores per person and increase the biopsy core positive rate for patients with low and median PSA value [21].
The biopsy core positive rate of CEUS-TB, which was above 95%, was significantly higher than SB in present study. The display of tumor tissue by contrast agent facilitated locating tumor lesions which might increase the positive rate of core samples. Mitterberger M et al. reported that CEUS-TB detected more cancer than SB in 690 patients [22].
Our study has some limitations. First, the CEUS was performed using LOGIQ® E9 with intracavity probe while the prostate biopsy was performed using MylabTMTwice with biplane probe for the sake of sterility. The probe transfer increased the likelihood of introducing localization errors. Second, biopsy results were served as reference standard in this study, therefore verification bias might be occurred, especially for patients diagnosed with benign disease. Third, patients enrolled in this study lived in rural areas lacking of medical resources and the mean age is over 70 years old, PSA values are higher when found which resulting in the number of the low and median PSA groups is relatively small. The aim of our study is focus on rural China, the stratification of PSA value is relatively reliable. Forth, according to international the gold standard is MRI with CEUS including diffusion imaging. Unfortunately, our hospital belongs to the basic units, and the popularization rate of MRI is not enough. As for the import of MRI in last year in our hospital, the use of MRI and MRI fusion biopsy could be play important role in future. Fifth, in our study we chose SonoVue which may missing some less aggressive cancers. BR55® as a new type of vascular endothelial growth factor receptor 2 (VEGFR2) specific contrast agent showed better tumor specificity, better imaging, and early diagnosis of metastasis [23, 24] which need further study.
In summary, although the significant difference was not seen between 12 core-SB and 8 core-SB of PCa detection rate in low PSA group, the detection rate of 12 core-SB is higher than that of 8 core-SB, thus multi-point systematic biopsy is still very necessary for patients with low PSA. As for patients with higher PSA value, the PCa detection rate by CEUS-TB was similar with SB, while could relieve patients’ suffering by reducing the number of biopsy cores, especially for older people.
Funding
The financial support by the Science and Technology Commission of Shanghai Chongming District Foundation (CKY2017-05).