
Abstract
OBJECTIVE:
To assess the impact and procedural input of intraoperative ultrasound (IOUS) with contrast-enhanced ultrasound (CEUS) and ultrasound elastography on surgical decision making during the procedure and consequently the outcome after hepato-pancreatico-biliary (HPB) surgery.
MATERIALS AND METHODS:
Data of 50 consecutive patients, who underwent HPB surgery from 04/2018 to 07/2018 were prospectively collected for this study. During surgery, IOUS with a high-resolution ultrasound device using CEUS after bolus injection of 2.4–5 ml dulphur hexafluoride microbubbles using a 6–9 MHz probe and a share wave and strain elastography was performed by an experienced examiner. Process and time analysis were carried out using mobile phone timer.
RESULTS:
The IOUS with CEUS and elastography correctly identified 42 malignant tumors and 4 benign lesions. In 3 cases, the examination provided false positive result (identifying 3 benign lesions as malignant) and in 1 case a malignant lesion was incorrectly assessed as benign (sensitivity 97,7%, specificity 57,1%, PPV 93,3% and NPV 80%).
The specific question by the surgeon could be answered successfully in 98% of the cases. In 76% of the cases, there was a modification (42%) or a fundamental change (34%) of the planned surgical approach due to the information provided by the IOUS. Within the last group, the IOUS had a major impact on therapy outcome. In 7 patients an additional tumor resection was required, in 5 patients the tumor was assessed as inoperable, and in total in 5 patients an intraoperative RFA (4/5) or postoperative RITA (1/5) was required.
Regarding procedural input, there was only a slight, but significant difference between the transport and set-up times before the intraoperative use (mean: 14 min 22 s) and the return transport (mean 13 min 6 s), (p = 0,038). The average examination time was 14 minutes, which makes only one third of the overall time demand.
CONCLUSION:
Combination of IOUS with CEUS and elastography in oncological HPB surgery provides valuable information that affects surgical decision-making. The procedural input of about 45 minutes seems to be a good investment considering the improvement of the surgical procedure and a significant modification of the therapy approach in the majority of the cases.
Introduction
Intraoperative ultrasound (IOUS) has been established as imaging technique in hepato-pancre-atico-biliary surgery. Technological development over recent years enabling a higher resolution with each new generation of ultrasound device and new techniques such as strain (SE) or shear wave elastography (SWE) [1–4], together with the use of contrast enhanced ultrasound (CEUS) [5, 6]. emphasizes the increasing significance of ultrasound as intraoperative diagnostic tool [7]. The use of IOUS together with CEUS and elastography offers a more accurate localization and characterization compared to surgeon’s palpation, especially considering the fact that not all malignancies are palpable [8]. Furthermore, IOUS provides exact information about the anatomical relationship to the surrounding tissue and macrovascular invasion. In addition, CEUS gives detailed information on the microvascularization which can help to differentiate between benign and malignant lesions [9, 10]. Furthermore, the second generation microbubbles contrast agents, currently used by CEUS are safer compared to iodinated or gadolinium chelate contrast agents used by contrast enhanced computed tomography (CT) or magnetic resonance tomography imaging (MRI), respectively [11–13]. New ultrasound elastography techniques like strain elastography (SE) and shear wave elastography (SWE) allow to investigate the stiffness of the tissue and represent an extension of conventional ultrasound [3]. This can be useful as an additional tool to surgeon’s palpation in inaccessible areas. By exact tumor localization and a high resolution depicting of the anatomical relationship of a potential macrovascular invasion (portal vein, coeliac trunk, common hepatic artery, superior mesenteric artery), the combination of intraoperative CEUS and elastography can help to assess surgical resectability of a tumor with great influence on complication rate as well as on patient’s long-term out-come [1, 14].
The aim of our study was to analyze the impact of IOUS on surgical decision-making during hepato-pancreatico-biliary surgery using the combination of CEUS and ultrasound strain as well as shear wave elastography. Furthermore, we investigated the whole logistical process and including time and costs of IOUS and elastography in a high-volume university hospital in order to compare impact and input.
Material and methods
Data collection
Data of 50 consecutive patients, who underwent hepato-pancreatico-biliary surgery from 04/2018 to 07/2018 were prospectively collected for this study. In all cases, a preoperative imaging with CT or MRI was performed. During surgery, IOUS with CEUS and elastography was carried out by an attending radiologist with more than 10 years of clinical experience (DEGUM III). All IOUS examinations were performed on high-end ultrasound device (LOGIQ E9, GE) using multifrequency (6–9 MHz) linear probe in virtual convex mode. In some cases, a special T-shaped probe was used to examine hardly accessible areas.
Intraoperative and postoperative histopathological findings were used to assess the accuracy of IOUS. Therefore, results from preoperative CT or MRI imaging were compared with data from IOUS with CEUS and elastography as well as with the histopathological findings. All acquired data were retrospectively analyzed using Youden’s statistic and t-test for paired samples.
The use of CEUS, CT or MRI for this study was approved by the local ethical committee (University of Regensburg) and patient’s informed consent was obtained prior to the surgery. The study was approved by the local ethics committee (approval number 18-1137-104). Inclusion criteria were age >18, preoperative imaging with either CT or MRI, suspected lesion in the hepato-pancreatico-biliary tract and potential resectability.
Analysis of IOUS impact
In order to examine the relevance of the obtained information and its influence on the surgical procedure, a questionnaire was used to assess whether the surgeon’s questioning could be answered and whether the surgical procedure was changed due to the IOUS examination. We quantified the influence on the surgical procedure with three subgroups - low influence, partial influence and fundamental influence. In the first case, the examination did not resolve in any significant modification of the surgical procedure. In the second subgroup, the IOUS was used to exactly mark the tumor margin. In the last subgroup, either previously unknown lesions were found (requiring additional resection, intraoperative or postoperative RFA) or the examination revealed inoperability of the tumor.
Process and principles of IOUS examination
During the surgical procedure, the senior surgeon usually made the final decision to what extent high-resolution intraoperative ultrasound was required. Therefore, the interdisciplinary ultrasound center was contacted and the first phase – the transport phase of the ultrasound device with introduction into the operating room – began. After sterile wrapping of the ultrasound probe and patient registration, the examination phase started. First, the surgical site examined in fundamental B-mode and vascularization supplemented by Color-Coded Duplex sonography (CCDS) was performed, followed by an elastography (Fig. 1–5 for patient A and Fig. 6–10 for patient B). Currently, all available elastography techniques are based on measuring tissue displacement [2]. This can be achieved either by palpation with the probe (strain elastography or SE) or it is ultrasound induced in shear wave elastography (SWE) (in this case the probe generates radiation force impulses, that cause the tissue displacement in tens of μm). The tissue displacement can then be measured directly in m/s or kPA converted to the tissue strain (SE), or used to detect the speed of induced shear waves (SWE). Since all these values differ depending on tissue elasticity, they can be used to display different tissue stiffness [2, 3].

CT of patient A, a 67 year old female patient with the diagnosis of an intraductal papillary mucinous neoplasia of the main duct of the pancreas. An irregular dilatation of the pancreatic duct throughout the entire organ is shown which is even better represented in Fig. 8. In the pancreatic head region, the main duct also shows partly complicated cystic formations (arrow).
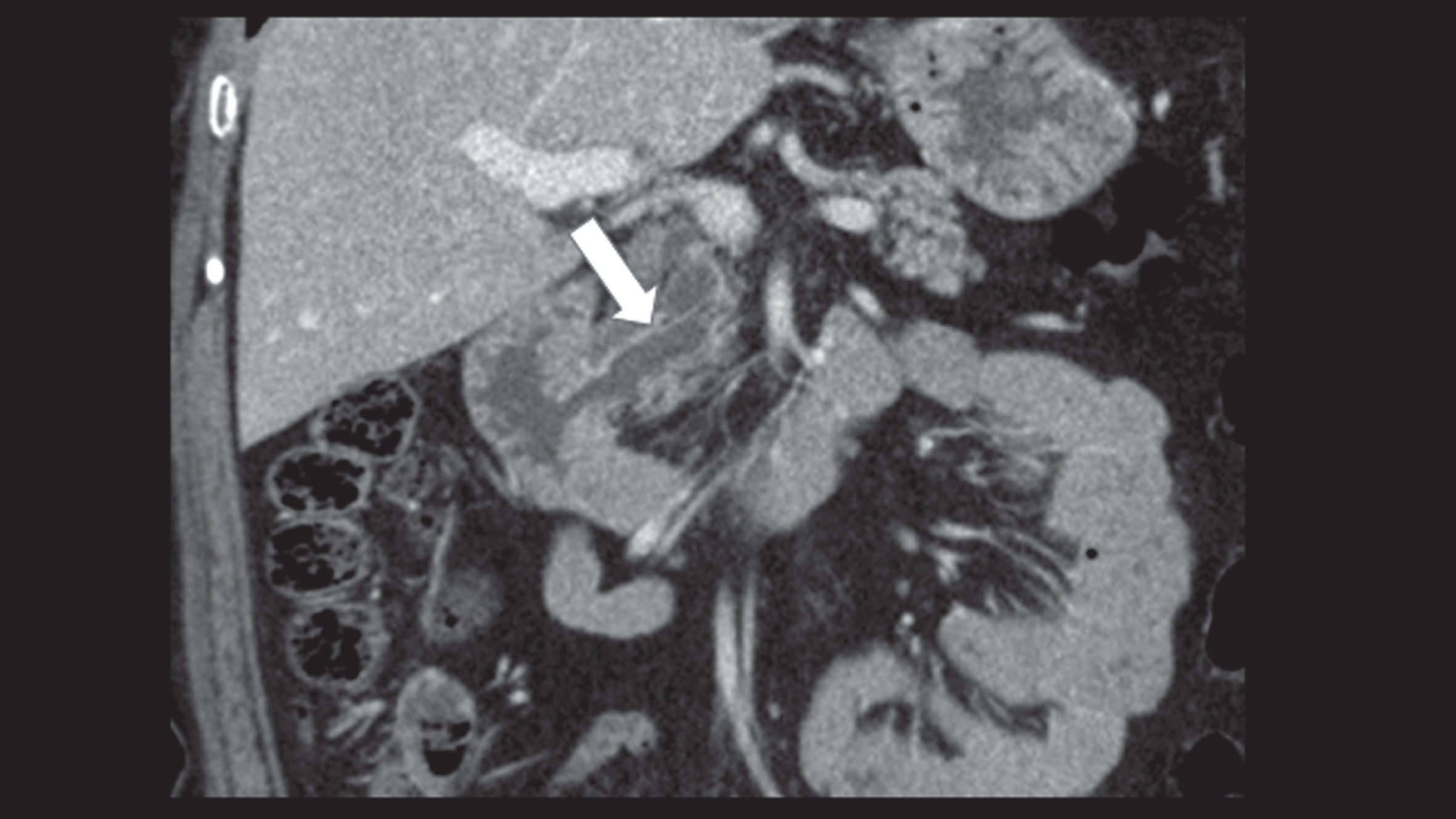
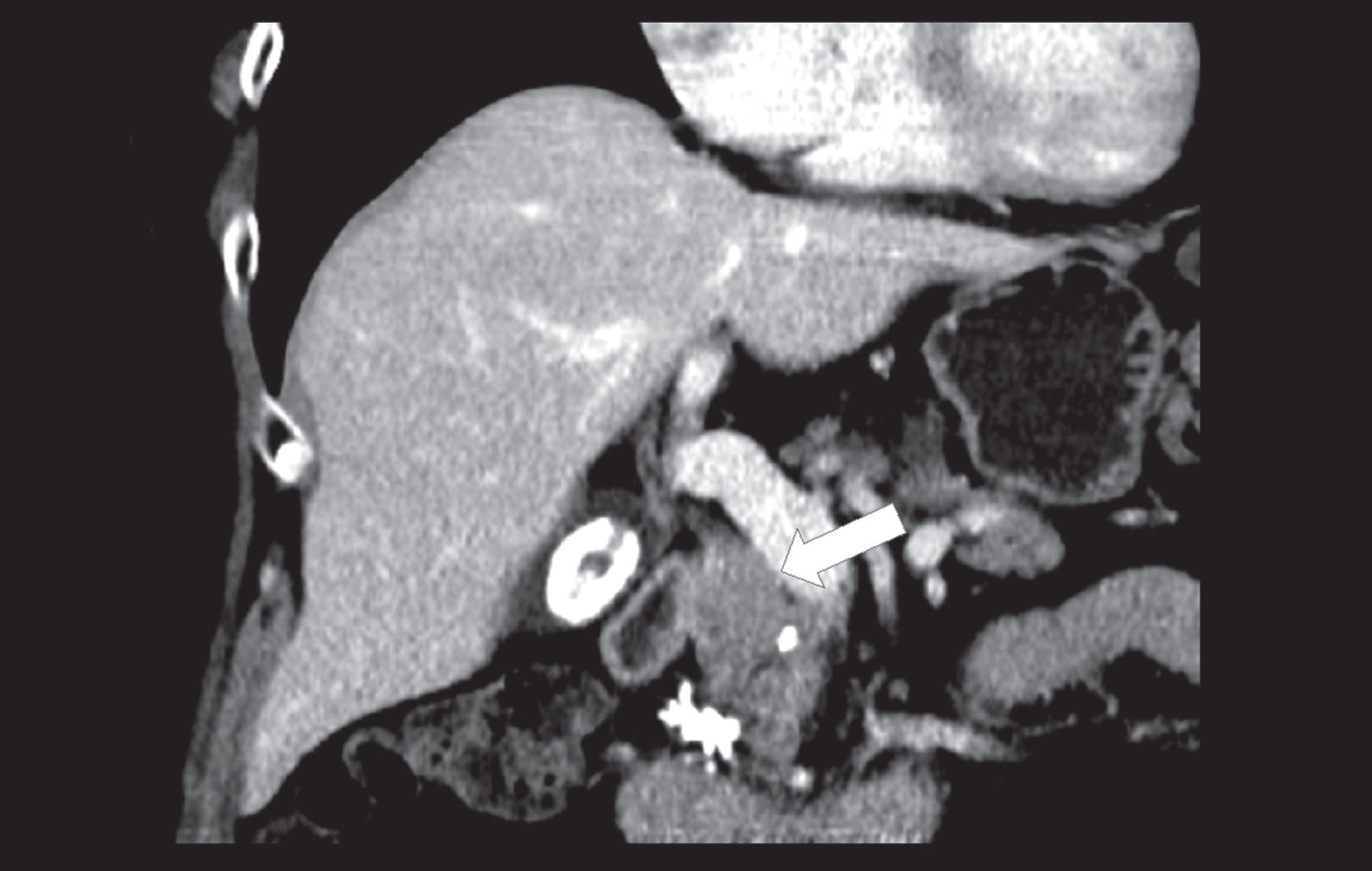
A CT of the same patient in the coronary layer with an irregular dilatation of the pancreatic duct throughout the entire organ with an intraductal papillary mucinous neoplasia of the main duct of the pancreas.
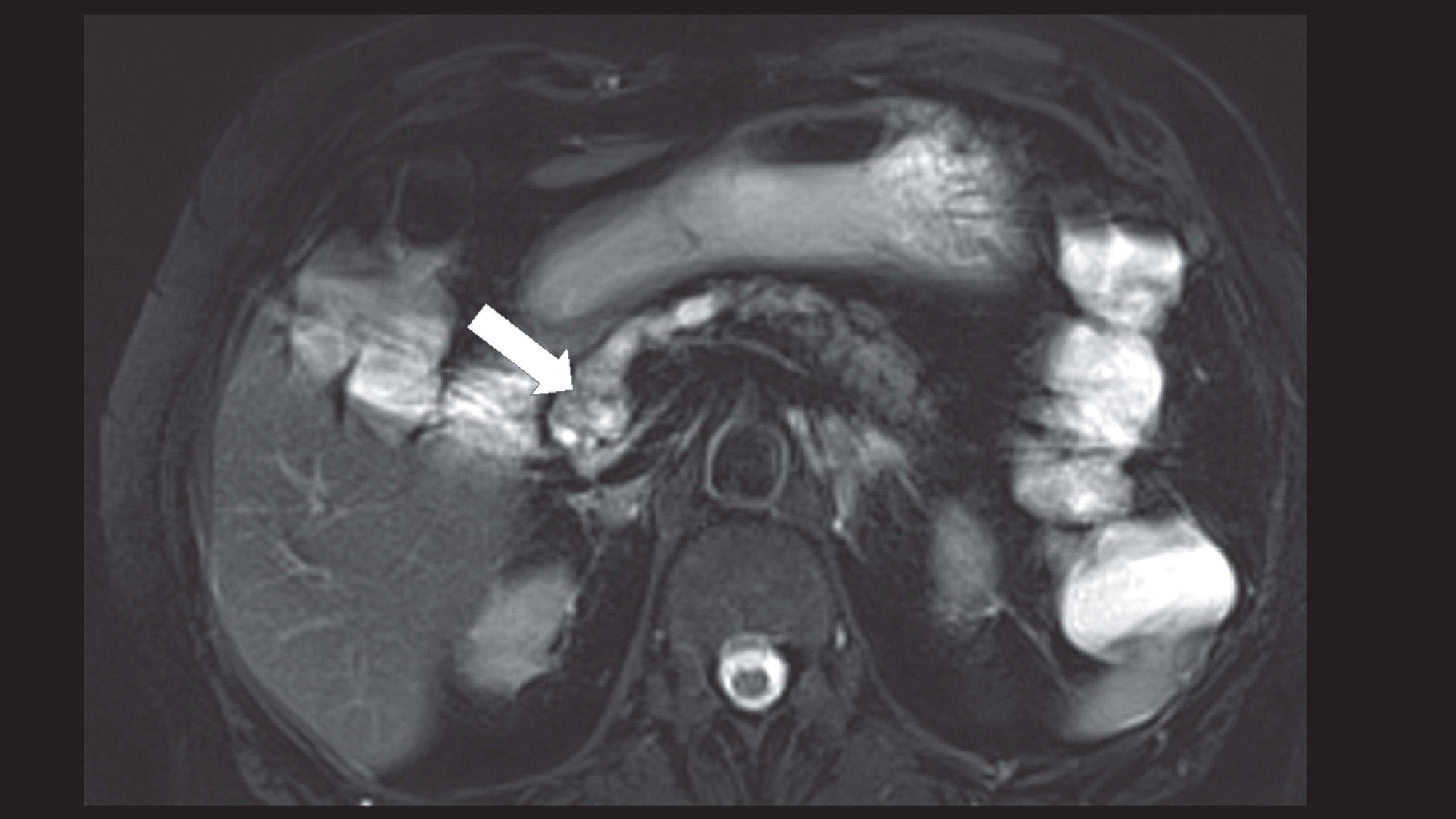
In the MRI of the same patient, the T2 BLADE fat saturation sequence also shows a dilatation of the pancreatic duct with cystic formations in the head area of the pancreas (arrow).
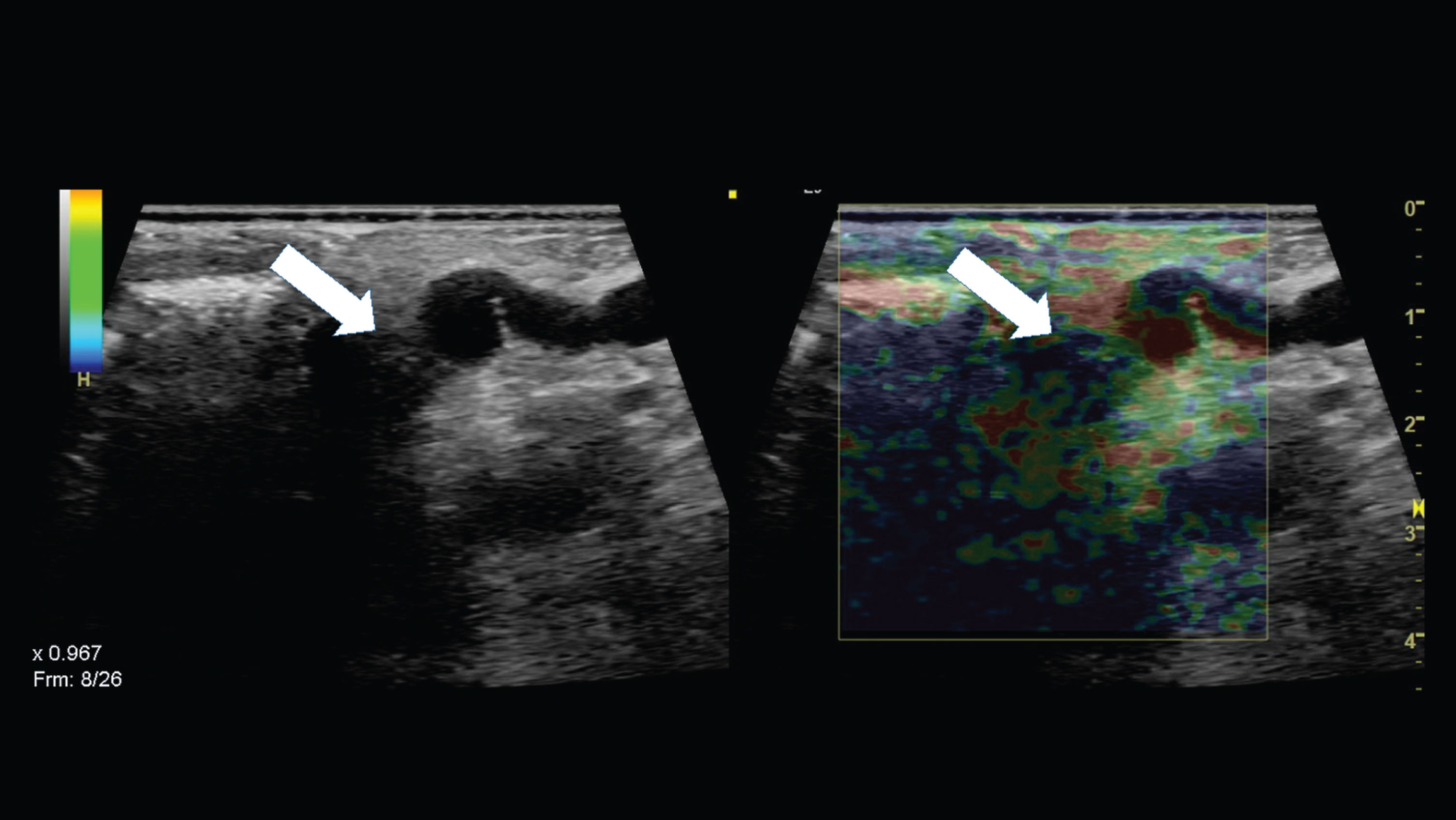
The same patient received a Whipple-operation. Intraoperatively, we performed an ultrasound with a 6–9 MHz linear probe. The strain elastography showed an inhomogeneous hardening of irregular wall structures in the pancreatic head area (arrow).
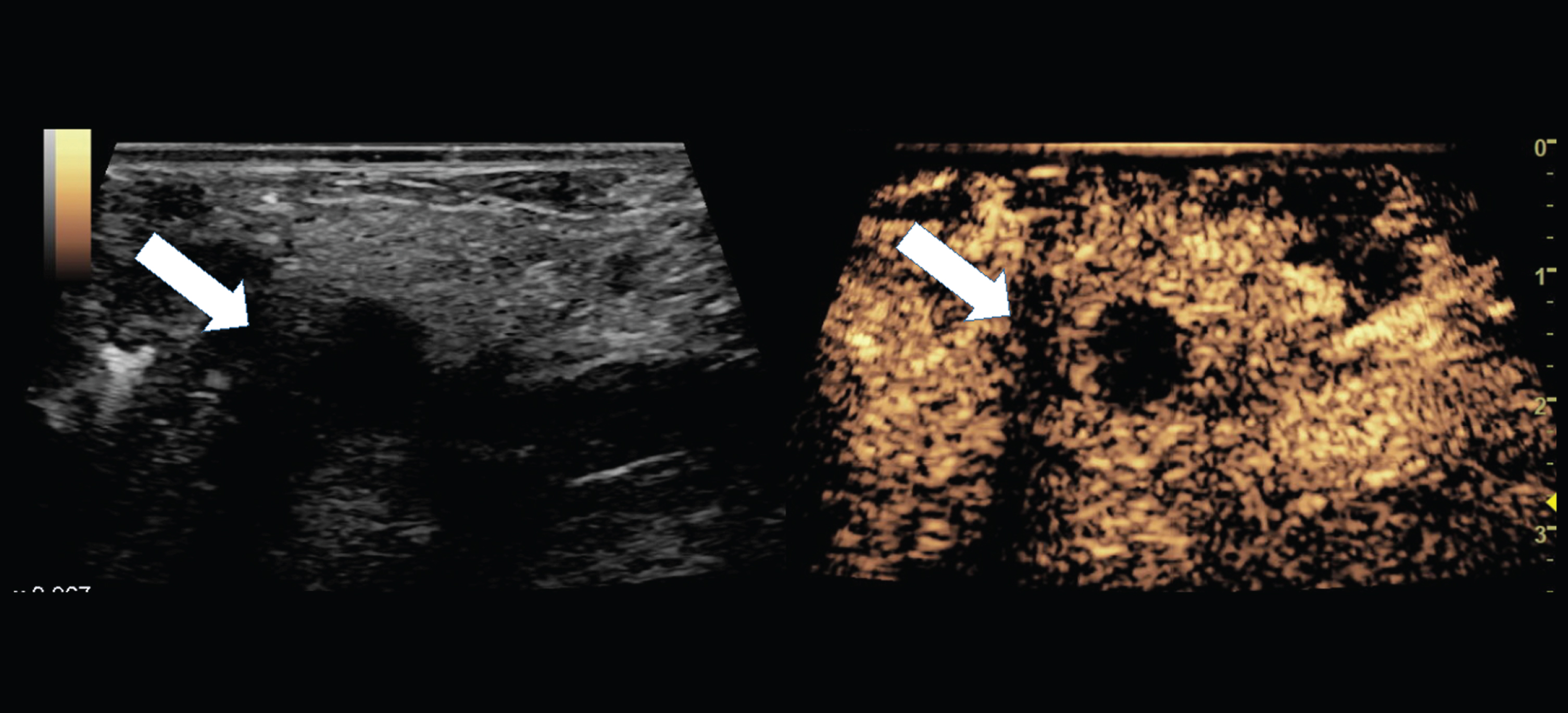
We also conducted a CEUS intraoperatively. For this purpose, 5 ml SonoVue® was administered intravenously to the patient via a central venous catheter. Irregular, marginal vascularized cystic (contrast medium recess) formations in the sense of an intraductal papillary mucinous neoplasia of the main duct were observed (arrow).
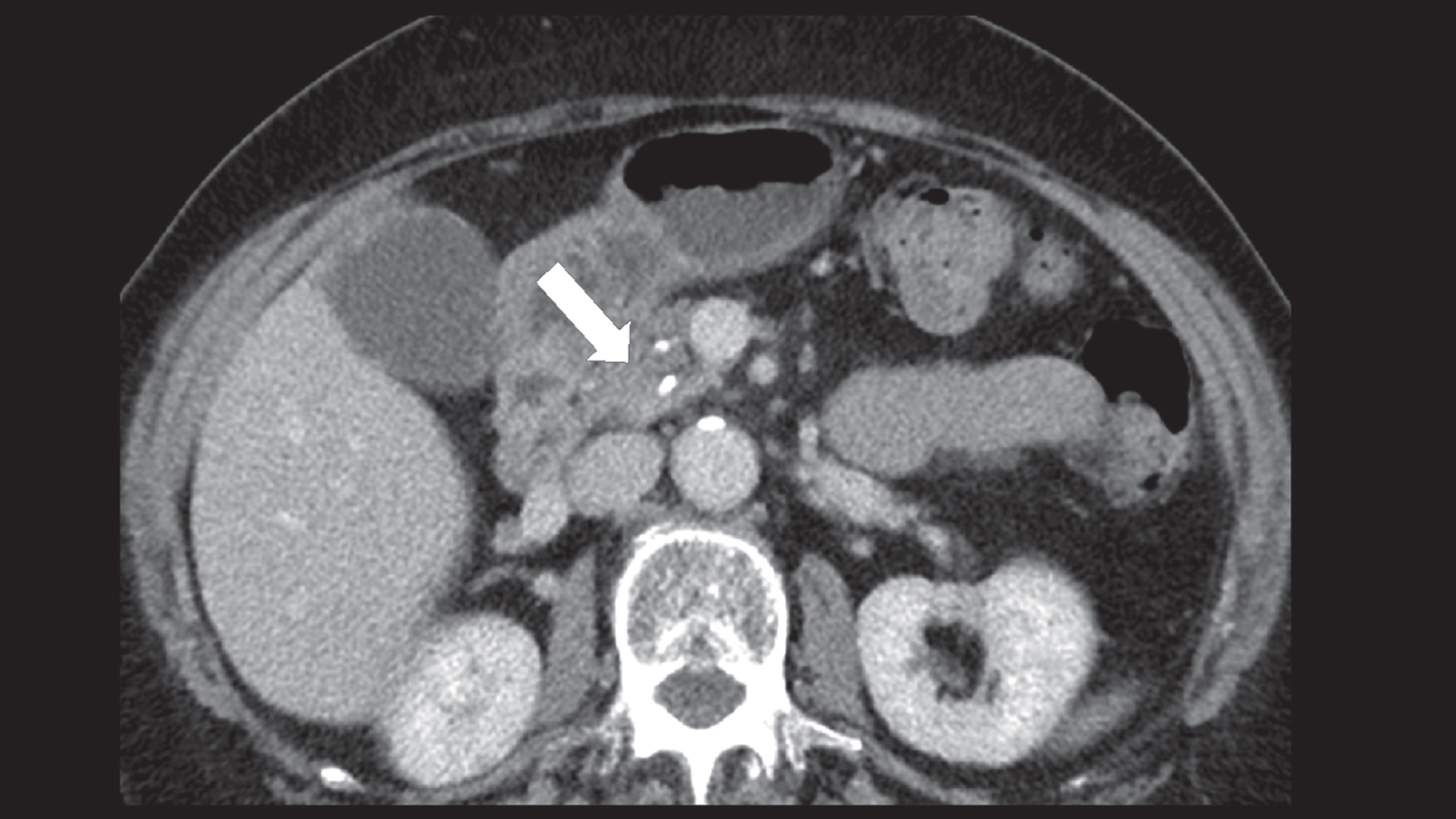
CT of patient B, a 78 year old female patient with an approx. 3 cm large tumor in the pancreatic head (arrow). The tumor shows contact to the portal vein.
A CT of the same patient in the coronary layer with the extension of the pancreatic head tumor measuring about 3 cm.
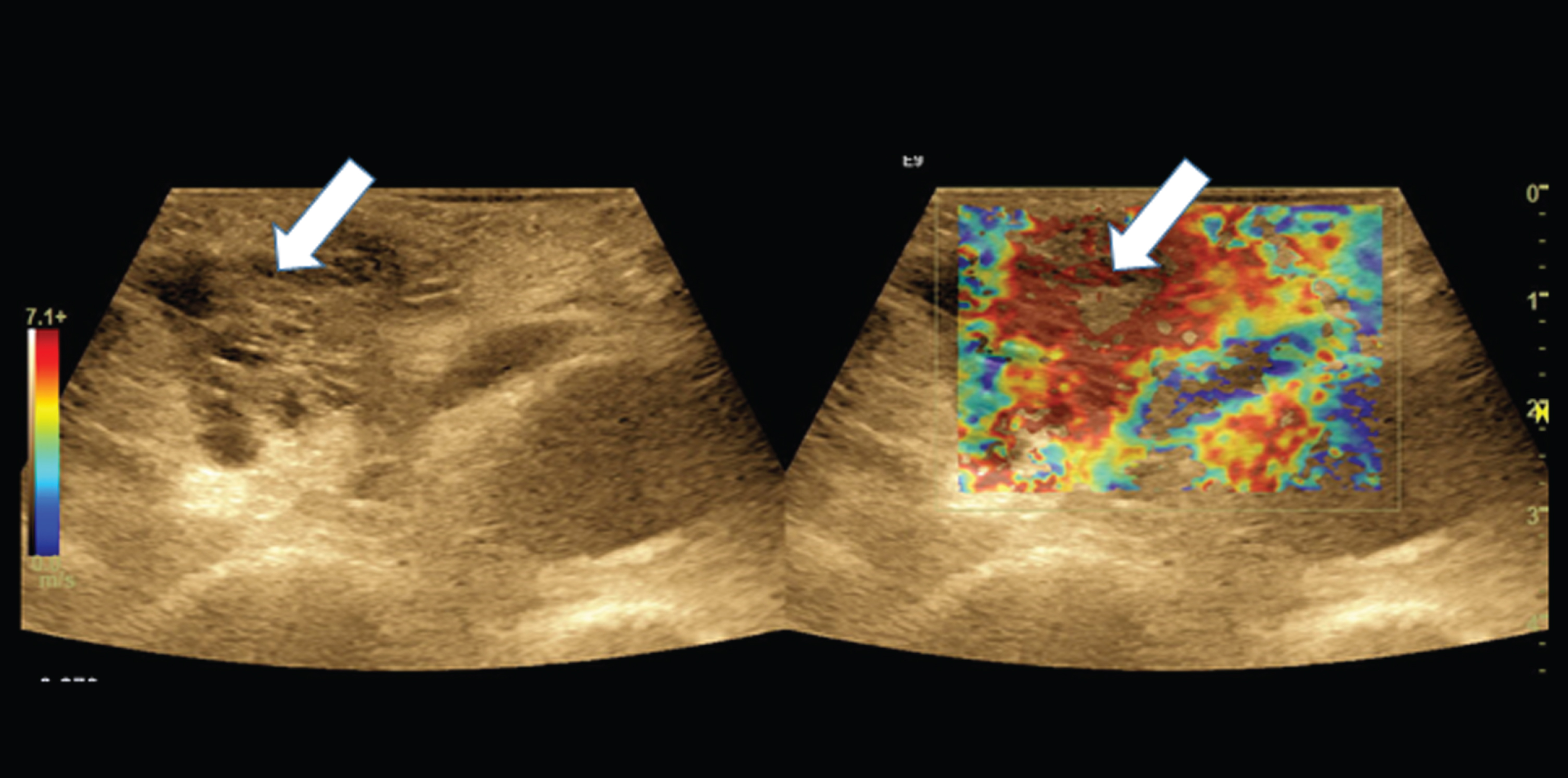
Intraoperatively, we performed a shear wave elastography which shows a distinct inhomogeneous mass in the pancreatic head with values up to 7 kPa (red colored).
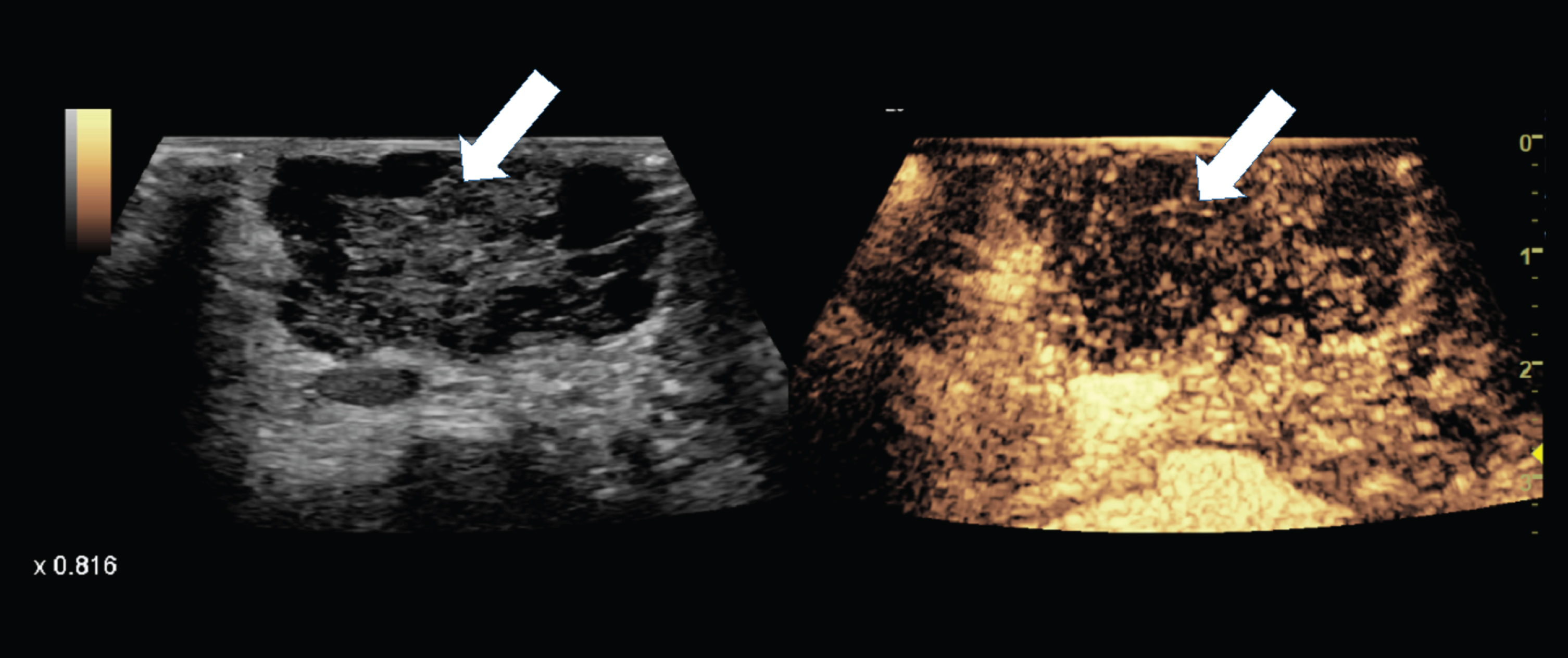
We also conducted a CEUS intraoperatively. For this purpose, 5 ml SonoVue® was administered intravenously to the female patient via a central venous catheter. Here a complicated cystic process with irregularly wall-thickened tumor cysts (arrow) is shown.

In the intraoperatively CEUS a wash out of the irregularly wall-thickened tumor cysts in the pancreatic head (arrow) is visible after about 3 minutes. This is to be regarded as a malignancy criterion.
In order to perform CEUS, the anesthesiologist administered centrally 2.4–5 ml of sulphur hexafluoride microbubbles (SonoVue®, Bracco, Italy) to perform the CEUS. The ultrasound contrast agent (UCA) consists of gas micro-bubbles (stabilized by a shell), that strongly increased the backscatter of ultrasound. Due to their small physical size (<10 μm) and ability to stay in intravascular space, the microvascularization as well as dynamic microvasculature of lesions could be displayed during all vascular phases (arterial, portal venous, late and post-vascular phases). First, the CEUS was used to localize and characterize the lesion already seen in preoperative imaging. Then, a scan of the complete organ was performed to detect additional lesions and mark their resection margins [1]. Because of the fact that the contrast agent was almost completely washed off the tissue after a few minutes, this phase generally lasted up to 5 minutes. If necessary, re-administration of the contrast agent could take place. In some cases, RFA was performed intraoperatively under ultrasound control which implied additional time for the examiner. RFA was performed with ultrasound guidance using a RITA probe (Angiodynmic), with flexible diameter from 1 up to 5 cm.
In the last phase, the ultrasound probes were unpacked, cleaned and the device was returned to the ultrasound center. Time was recorded via mobile phone timer to assess the time demand of each step of the whole process.
Accuracy of IOUS
Data of 50 consecutive patients, who underwent liver or pancreas surgery from 04/2018 to 07/2018 were prospectively collected for this study. The patient group consisted of 31 males and 19 females, aged between 30 and 85 years (65 years±12 years). The postoperative histology showed 43 malignant findings, including 16 primary liver tumors, 12 secondary liver tumors, 11 pancreatic adenocarcinomas, 4 other malignancies, and 7 benign findings (Table 1).
Summary of postoperative histopathological findings
Summary of postoperative histopathological findings
First, we wanted to assess the accuracy of the IOUS examination by comparison with the postoperative histopathology report. The IOUS correctly identified 42 malignant tumors and 4 benign lesions. In three cases, the examination provided false positive results (identifying 3 benign lesions as malign) and in one case a malignant lesion was incorrectly assessed as benign. Thus, the sensitivity of IOUS examination using combination of CEUS and elastography was 97,7%, the specificity was 57,1%, and the overall accuracy 92%. The PPV was 93,3% and the NPV was 80% (Table 2). The false positive findings were histo-pathologically described as chronic fibrosing cholangitis (2 cases) and intraductal papillary mucinous neoplasm (1 case). In all these cases, there was a partial washout of microbubbles contrast agent during the venous phase of intraoperative CEUS and the elastography showed tissue stiffening in the region of interest. The only false negative finding was histologically assed as cholangiocarcinoma. Here, the intraoperative elastography correctly identified an increased tissue stiffness, but without a significant wash out during CEUS. Thus, the lesion was incorrectly identified as chronic fibrosing cholangitis. Regarding the liver malignancies, in nine patients IOUS identified 12 previously unknown malignant focal liver lesions (size up to 12 mm), which were not recognized in preoperative imaging with CT or MRI.
Comparison of IOUS findings and the results from histopathology
Next, we wanted to determine if the IOUS has an impact on surgical decision making during the procedure. The surgeon’s questioning could be answered successfully in 98% of the examinations. Furthermore, a significant impact of the IOUS on the surgical procedure and the decision making has been observed, resulting in a partial modification of the surgical procedure in 42% of cases and even a fundamental change of the surgical procedure in 34% of cases (Fig. 11). Within this last group, the IOUS examination had a major impact on therapy outcome (Fig. 12). In 41% of these patients, a further tumor resection was required whereas in 29% the IOUS examination led to identifying inoperability (mostly due to tumor infiltration of large vessels) and therefore to discontinuation of surgery. If the detected tumor lesions could not be resected, additional intraoperative radiofrequency ablation (RFA) was required in 24% of the cases.

Modification of the surgical procedure based on IOUC. The impact of IOUS was categorized as none, partial, or fundamental.
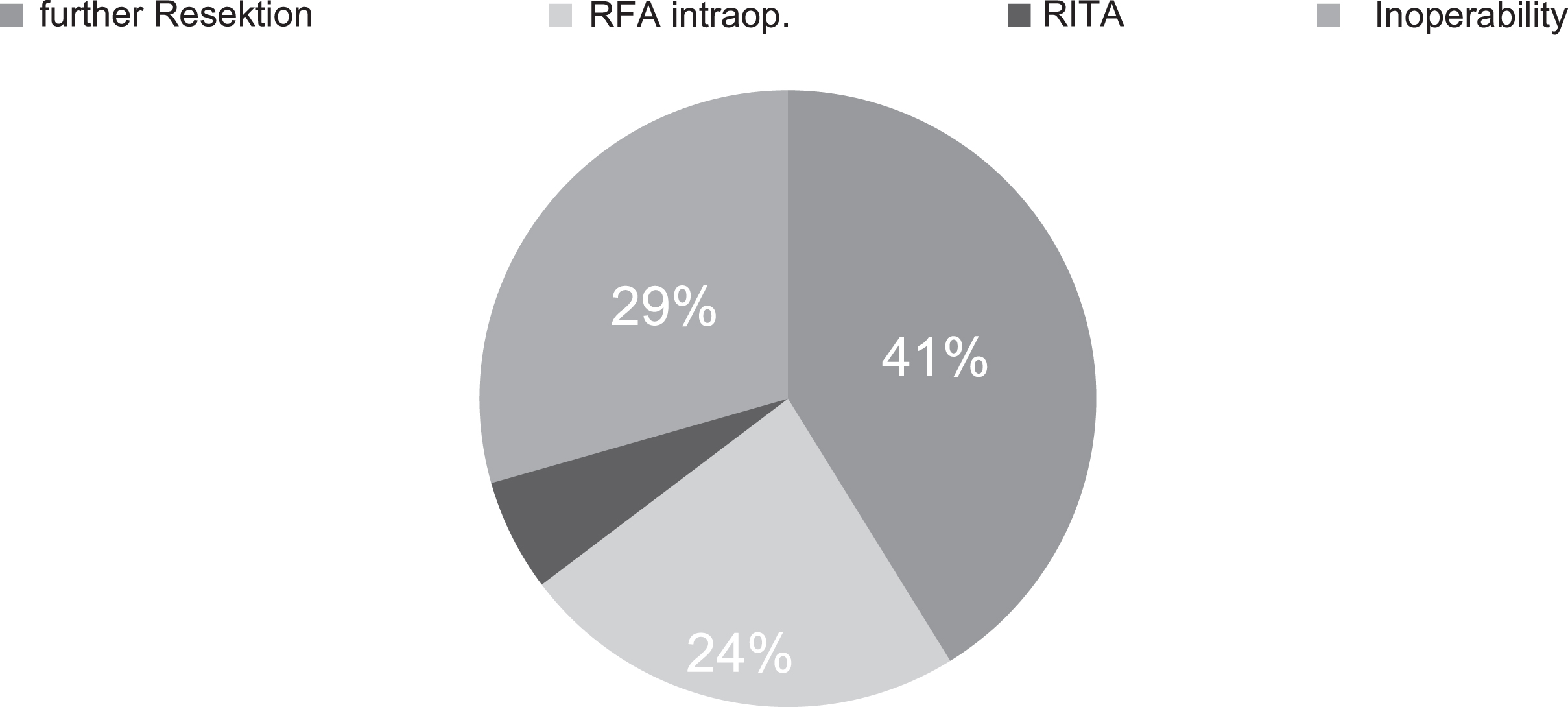
Subgroup analysis of the group with a fundamental modification in the surgical procedure.
Since nowadays due to huge economic pressure within modern health systems every new technique has to justify time and costs in relation to the medical benefit, we then wanted to analyze the procedural input. As shown in Fig. 13, there was slight but significant difference between the transport and set-up time before the intraoperative use (14 min 22 s±3 min 19 s) and the return transport (13 min 6 s±3 min 35 s, p = 0,038).
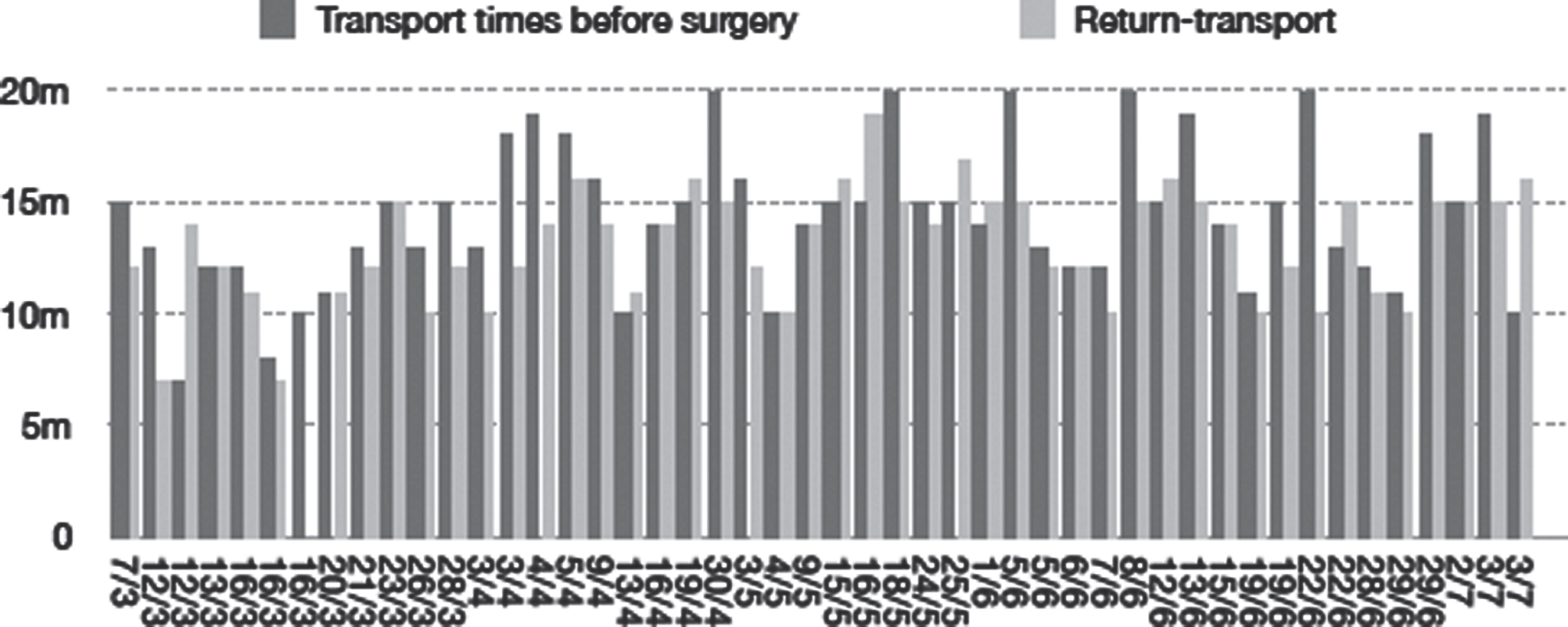
Transport of the ultrasound device. Black columns represent the transport and set-up times before the surgery, grey columns show the return transport times.
The set-up process with patient registration, probes preparation with the appropriate sterile coating, and preparation of the ultrasound contrast agent for injection usually took about 10 minutes. A bolus injection of up to five ml of the ultrasound contrast agent (UCA) consisting of three components, gas, liquid and dry substances, is administered via a central access by anesthesiologist. Ideally, these components should be mixed together just before the intravenous injection. Within five to ten minutes, high-resolution linear probe with transmission frequencies of 6–9 MHz was used to examine the tumors, first in fundamental B-mode and then in color Doppler. Ultrasonic elastography with compound and shear wave technology were used. The contrast injection was administered by anesthesiologist which took a maximum of five minutes. Then, all tumor sites were localized by CEUS, characterized as benign or malignant, and the malignant tumors were marked for resection in the wash out phase (of UCA) after one to five minutes. This tumor resection planning phase took up to 20 minutes in some cases if additional advanced mobilization of the liver or pancreas were required (Fig. 14). If a RFA was necessary, it took up to 45 minutes, since the RFA was performed ultrasound-guided [15, 16]. The required time factor depended on the preparation for RFA by providing the patient with neutral electrodes and on the availability of ablation device that was not stored in the operation unit, which could lead to additional transport time.
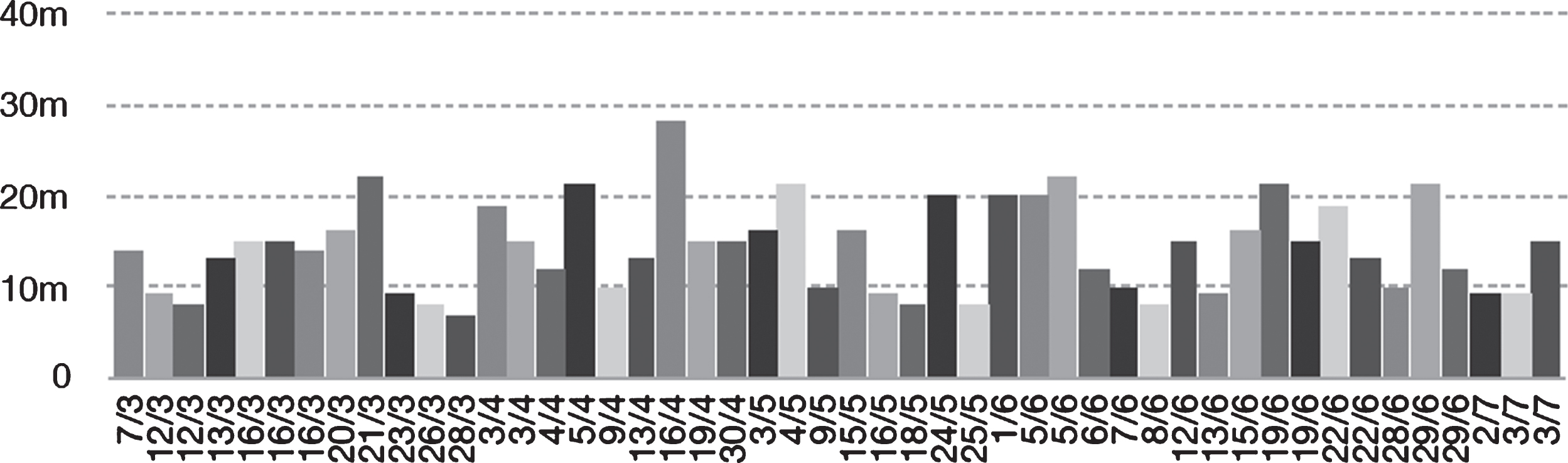
Duration of the IOUS examination. The columns show duration of each measured examination. The time demand of IOUS varies from 8 to 21 minutes, depending on examined organ, complexity of situs or need for repeated administration of contrast agent.
CEUS significantly increases the diagnostic certainty for the localization of even small tumor lesions <10 mm, which otherwise could only be detected by MRI or CT. However, it should be noted that SonoVue® is a strictly intravascular contrast agent. In the case of small lesions <10 mm, no wash out is required in the late phase, which is considered as a malignancy criterion. However, marginal hypervascularization may [9]. Elastography can determine the density of the tissue surrounding the tumor and facilitate the surgeon’s decision as to the extent to which the adjacent tissue should be resected to the tumor.
The sensitivity of IOUS using combination of CEUS and elastography was 97,7% in our study. There are various reports about use of percutaneous CEUS in liver [17–19] and pancreas [20] imaging, suggesting a sensitivity of 92-93,5 % and 89% respectively. Regarding the intraoperative use of CEUS, similar sensitivity rates as in this study were published recently [12, 22]. According to our experience, CEUS is superior to elastography in detection and characterization of malignant lesions. However, the elastography can be useful in some cases and the combination of both CEUS and elastography should be recommended to improve the overall accuracy [1, 3]. The IOUS correctly identified 4 of 7 benign lesions. Thus, the specificity was only 57%. This can be explained by limitations in design of this study - mainly by small group of patients with benign lesions. In 76% of the cases, there was a modification (42%) or a fundamental change (34%) of the surgical procedure due to the information provided by the IOUS. It has been already established that IOUS provides additional information compared to the preoperative imaging with CT or MRI [1, 24]. Considering the improved accuracy of the ultrasound imaging and the impact of IOUS on the surgical procedure showed in our study, we expect an increasing importance of this technique in the future. It can also be assumed that more frequent use of this method in tumor surgery could lead to better therapy outcome and lower complications rate due to improvement of the surgical procedure. Regarding liver tumor imaging, intraoperative ultrasound has proved to be beneficial by experienced examiners, because it is possible to detect tumors quickly and reliably and then mark them for resection [11, 24]. For tumors of the pancreas, a final rating is still pending. Especially, IOUS can safely detect small tumors, which cannot reliable be palpated. This improves the surgical approach and contributes to the overall therapy outcome [25]. It may also turn out that such extensive tumor infiltration is detected by the intraoperative high-performance ultrasound that no surgical resection is possible. This may then require neoadjuvant or palliative chemotherapy.
To obtain similar results presented in our study, however, we find it is essential to maintain the benefits of using a high-resolution ultrasound device, together with CEUS and elastography. The sensitivity and specificity of CEUS vs. CEUS combined with elastography has been reported to be 86.4% and 93.2% vs. 97.7% and 94.6% for BI-RADS 4 breast lesions [26] as well as 77.1% and 78.3% vs. 91.7% and 95.7% for TI-RADS category 4a and 4b thyroid nodules [27].
The average time needed for the transportation of ultrasound device into operating room (together with introduction and preparation for intraoperative use) and transportation back from operating theatre was about 14 minutes and 13 minutes, respectively. Compared to the average time needed for the IOUS examination, the overall transport time makes two thirds of the overall time devoted to the whole process. This could be avoided by centralization of ultrasound device into operating rooms area. The time recording performed for the first time within this work can form the basis, to what extent a scheduling and central stationing of multifunctional ultrasound devices could reduce the transport and set-up times and allow intraoperative ultrasound examinations to be carried out in a time-opti-mized manner.
Finally, comparing our results to findings with different ultrasound contrast agents (UCA), Sonazoid is a 2nd generation UCA, composed of microbubbles of perfluorobutane gas coated with hydrogenated egg phosphatidylserine sodium (H-EPSNa) with a mean size of 2.6 μm. While Sonazoid is not allowed to use in Europe at this time, it is a liver-specific UCA and allows imaging in the postvascular phase (Kupffer phase) as well as the dynamic vascular phases. In contrast to other UCAs, Sonazoid has a unique potential to be used for the detection of HCC lesions in various settings, including disease surveillance [28]. While there are no reports about the combined intraoperative application of CEUS with Sonazoid (S-CEUS) and elastography, it has been shown that S-CEUS is useful especially for detecting small metastatic liver lesions for instance after chemotherapy [29]. For the diagnosis of HCC lesions, a benefit of intraoperative S-CEUS has been shown with a sensitivity of 98%, a specificity of 83% and an accuracy of 97% [30]. Furthermore, a few retrospective studies have reported the use of S-CEUS in diagnosis of pancreatobiliary disease. Three-dimensional contrast-enhanced patterns are useful for the differential diagnosis of solid pancreatic lesions, with a reported diagnostic accuracy of 90.5% [31].
Conclusion
Combination of IOUS with CEUS and elastography in oncological liver and pancreas surgery provides valuable information that affects surgical decision-making. This leads to improvement of surgical procedure and also to a significant modification of the overall therapy approach. Time-optimization could be achieved by centralization of the equipment, as the transportation of the device represents a significant time demand.