
Abstract
OBJECTIVE:
This study aimed to evaluate the diagnostic and prognostic value of 13N–NH3·H2O positron emission tomography combined with computed tomography (PET/CT) for non-obstructive coronary microvascular disease (CMVD).
METHODS:
A retrospective analysis was conducted on 70 patients with clinically suspected non-obstructive CMVD (35 males, 35 females) between March 2017 and August 2019. The average age of the patients was 53.32±7.82 years. The patients underwent 13N–NH3·H2O PET/CT and were divided into two groups based on diagnostic criteria: a CMVD group and a non-CMVD group. They were then followed up for 180–1,095 days. Data were analyzed using an χ2 test, the logistic regression model, the multiple linear regression model, the Kaplan–Meier method, the Cox proportional hazards regression model, and a receiver operating characteristic (ROC) curve.
RESULTS:
(1) The incidence of cardiovascular family history and a high calcification score (11–400) was higher in the CMVD group than in the non-CMVD group (58.8% vs. 20.8% and 29.4% vs. 5.7%, respectively; P < 0.05 for all), stress myocardial blood flow (MBF) and coronary flow reserve (CFR) values were lower in the CMVD group than in the non-CMVD group (2.280±0.693 vs. 3.641±1.365 and 2.142±0.339 vs. 3.700±1.123, respectively), and calcification score was higher in the CMVD group than in the non-CMVD group (110.18±165.07 vs. 13.21±41.68, respectively; P < 0.05 for all). Gender and diabetes were risk factors for stress MBF reduction (β= 1.287 and β= –0.636, respectively), calcification score and hypertension were risk factors for CFR reduction (β= –0.004 and β= –0.654, respectively), and hypertension, family history, and calcification score were risk factors in the CMVD group (OR = 7.323, OR = 5.108, OR = 1.012, respectively; P < 0.05 for all). (2) The prognosis of patients with CFR < 2.5 was worse than that of patients with CFR≥2.5 (x2 value: 27.404, P < 0.001). The risk of adverse cardiovascular events in diabetic patients was also increased (β= 0.328, P < 0.001). When CFR was set to 2.595, the prognostic sensitivity was 94% and the specificity was 80%.
CONCLUSION:
The technology of 13N–NH3·H2O PET/CT can be used for the diagnosis and prognosis of non-obstructive CMVD. Cardiovascular risk factors are related to the occurrence and prognosis of CMVD.
Introduction
It was previously believed that the main cause of angina pectoris was obstructive lesions of the epicardial coronary arteries, which were identified by coronary angiography. However, clinical studies have revealed that the occurrence of angina pectoris in patients without obvious coronary atherosclerosis—especially female patients—is more closely related to coronary microvascular disease (CMVD) [1–3]. In recent years, studies have found that CMVD is associated with vulnerable plaque, coronary artery spasm, and coronary microvascular dysfunction, and that the prognosis of patients with CMVD is poor [4]. Compared with people without coronary heart disease (CHD), the risk and mortality of major cardiovascular adverse events are higher for these patients [5]. Therefore, it is of great clinical significance to diagnose CMVD and evaluate the patient’s prognosis as soon as possible, allowing lifestyle and drug therapy interventions to be implemented earlier, thereby reducing the risk of serious cardiovascular adverse events.
At present, clinically invasive examination can be used to evaluate coronary microvascular function, selective coronary angiography, thermodilution, and intracoronary Doppler flow guide wire, these three technologies are used alongside thrombolysis in myocardial infarction (TIMI) blood-flow frame counting, index of microvascular resistance (IMR), and coronary microvascular resistance (CMR), which implement information about the number of main coronary arteries, the WISE-CAD risk score, the (corrected) TIMI frame number, and the blood-flow reserve fraction (FFR) obtained through coronary angiography to assess the prognosis of patients with non-obstructive coronary artery diseases (CADs) [6]. However, the invasiveness of these technologies means that their practicability, cost, safety, and repeatability are limited, so they are not widely used in clinical practice. As such, non-invasive examinations [7] are the first choice for the evaluation of coronary microvascular function: they are less time and cost intensive and allow repeatable measurements.
One option for non-invasive examination is transthoracic coronary artery blood-flow ultrasound imaging; unfortunately, however, it can only obtain reliable data on the left anterior descending branch of the heart and therefore cannot fully evaluate the function of the capillaries. Another option is single-photon emission computed tomography (SPECT), but this technology cannot offer an absolute quantitative measurement of coronary blood flow, so it cannot fully evaluate microvascular function. Further, although cardiovascular magnetic resonance imaging (CMRI) technology has recently been shown to be promising, adverse reactions caused by contrast media limit its clinical use. As such, it is vital for effective evaluation methods and prognostic evaluation indicators to be selected based on clinical needs.
With the continuous development of molecular imaging technology, which can obtain a variety of cardiac function parameters in a single examination, positron emission tomography combined with computed tomography (PET/CT) has become the benchmark for the non-invasive absolute quantitative measurement of myocardial blood flow (MBF) and coronary flow reserve (CFR). Its accuracy has been confirmed in a number of studies [8], and it provides an important technical means for the diagnosis and prognosis evaluation of CMVD. As such, it has become a well-researched topic worldwide. Further, one study revealed that CFR has important predictive value for the long-term prognosis of patients with ischemic heart disease; in particular, its prediction value of major cardiovascular adverse events, such as cardiogenic death, is significantly higher than that of the left ventricular ejection fraction [9].
At present, there are few studies on the diagnosis of CMVD, assessment of its risk factors, and prognosis evaluation through PET/CT. The above-mentioned prognostic studies were based on data analysis of foreign populations, and it is not clear whether they are applicable to Chinese patients. We conducted the first batch of studies on the diagnosis and risk stratification of CMVD in Chinese patients using PET/CT. The present study aims to assess the diagnostic and prognostic value of 13N–NH3·H2O PET/CT for non-obstructive CMVD and to evaluate the role of cardiovascular risk factors in the pathogenesis of CMVD.
Materials and methods
Materials
Subjects
The data of 70 patients with newly diagnosed clinically suspected CMVD who underwent 13N–NH3·H2O PET/CT in the Department of Nuclear Medicine in our hospital between March 2017 and August 2019 were retrospectively analyzed. Of the patients, 35 were male and 35 female; the average age of the patients was 53.32±7.82 years.
Inclusion criteria: (1) suspected CADs and typical angina pectoris symptoms, such as chest tightness and chest pain; (2) recent (within 1 month) coronary angiography or coronary CT angiography showed negative results (negative standard = stenosis of left anterior descending, left circumflex, and right coronary arteries < 50%).
Exclusion criteria: (1) contraindications of 13N–NH3·H2O PET/CT (systolic blood pressure of < 90 mmHg, heartbeat < 40 bpm, grade II–III ventricular block, asthma with persistent wheezing, congenital heart disease, cardiomyopathy, myocarditis, valvular heart disease, heart failure after revascularization, and unexplained heart failure); (2) allergy or contraindicated to dipyridamole; (3) did not complete the examination due to inability to tolerate the load during the examination; (4) failure of imaging, such as patient moving during acquisition or the rapid injection of imaging agent; (5) congenital heart disease, cardiomyopathy, myocarditis, valvular heart disease, heart failure after revascularization, and unexplained heart failure.
Follow-up and survival criteria: The primary endpoint was the recurrence of adverse cardiovascular events after discharge (including recurrence of angina symptoms, such as chest pain and chest tightness, hospitalization for acute myocardial infarction, percutaneous coronary intervention (PCI) stenting, and death from CAD). The deadline for follow-up was March 1, 2020, and the follow-up time was 180–1,095 days. The study endpoint for clinical absence of adverse cardiovascular events was from the date of clinical diagnosis to the follow-up deadline. The study endpoint for clinical presence of adverse cardiovascular events was from the date of clinical diagnosis to the date of recurrence and progression or the date of death.
All subjects signed an informed consent form before undergoing 13N–NH3·H2O PET/CT.
The absolute quantitative examination of 13N–NH3·H2O PET/CT myocardial blood flow passed the ethical review of the Ethics Committee of the hospital ([2019] Ethics R. No. (054)).
Research methods
Preparation before examination
Patients fasted for at least four hours before 13N–NH3·H2O PET/CT and were forbidden from taking vasoactive drugs, calcium antagonists, dipyridamole, adenosine drugs, or theophylline drugs, or from consuming tea, coffee, or caffeine-containing beverages 48 hours before the examination.
Methods for 13N–NH3·H2O PET/CT and data acquisition
The imaging instrument used was Discovers VCT (GE, USA); 13N was produced by the HM-10 medical cyclotron of Sumitomo, Japan. The subject was supine on the PET/CT table with both hands raised. A venous access was established on the back of one hand and a gated monitoring device was connected to the other hand, allowing blood pressure, heart rate, and electrocardiogram to be monitored in real time. The scanning range was from the level of the bifurcation of the trachea to the level approximately 2 cm below the apex of the heart.
First, resting myocardial perfusion imaging was performed. After an attenuation correction CT scan, a bolus injection of 10–15 mCi (370–555 MBq) 13N-ammonia was given. The PET program was initiated during the injection, and the continuous acquisition of image data lasted for 12 minutes. After acquisition, there was a 30-minute rest while the 13N ammonia decay cleared the background of cardiac radioactivity. Dipyridamole stress myocardial perfusion imaging was then performed. The dosage of dipyridamole injection was 0.142 mg/kg; the total dose was injected into the vein within four minutes. Three minutes later, a bolus injection of 13N ammonia was given, and the load procedure was completed with the same method mentioned above.
Image post-processing: (1) ACQC software was used for displacement, correction and reconstruction; (2) quantitative data from 12 minutes of PET data collected at rest and load were categorized into two types: early phase (E, first 2 minutes) and late phase (L, latter 10 minutes); this generated four groups of data: rest-E, rest-L, stress-E, stress-L; (3) absolute quantitative analysis was performed using Heartsee software (developed by the K. Lance Gould team, Texas Medical University, USA).; (4) coronary artery calcium (CAC) score processing flow: select CAC or Rest Cine sequence, open the Smartscore 4.4 software, select the patient’s somatotype, enter the program, select Regions, Display, clear Auto Detect Lesions, close. For each layer within the scanning range, the calcified area was delineated and the corresponding coronary artery was indicated. After the delineation was complete, the system generated three calcification scores: CAC, AJ-300, Mass, and Volume). The results of the AJ-300 score were chosen for analysis, and the patients were divided into three groups based on their CAC score: a low-risk group (CAC score of 0–10), a moderate-risk group (CAC score of 11–400), and a high-risk group (CAC score > 400).
Diagnostic criteria
A reference value of CFR < 2.5, which is widely used in associated literature, was used as the diagnostic standard for CMVD [10].
Statistical analysis
Data were statistically analyzed using SPSS 26.0. Normally distributed measurement data were expressed as mean±standard deviation (x±SD), and the categorical variables were compared using a chi-squared test. Multivariate analysis was conducted using the logistic regression model and the multiple linear regression model. Univariate survival analysis was conducted using the Kaplan–Meier method, while multivariate survival analysis was conducted using the Cox proportional hazards regression model. Stress MBF and CFR were analyzed using a receiver operating characteristic (ROC) curve to identify the best cut-off value of prognosis. P < 0.05 was considered statistically significant.
Results
Comparison of general reference indexes of patients
The patients were divided into two groups based on their diagnostic criteria: a non-CMVD group (CFR≥2.5, n = 17) and a CMVD group (CFR < 2.5, n = 53). A comparison of the general data of these two groups is shown in Table 1. The proportion of patients with a family history of cardiovascular disease and patients with a CAC score of 11–400 was significantly higher in the CMVD group than in the non CMVD group (58.8% vs. 20.8%, P = 0.003 and 29.4% vs. 5.7%, P = 0.025, respectively). The differences in other indexes between these two groups were not statistically significant (P > 0.05 for all).
Comparison of general indexes between the non CMVD group and CMVD group
Comparison of general indexes between the non CMVD group and CMVD group
Notes: BMI is body mass index; CFR < 2.5 in CMVD group, and CFR≥2.5 in non CMVD group, * is expressed as the difference between the two groups is statistically significant (P < 0.05).
The absolute quantitative parameters (rest MBF, stress MBF, CFR, and CAC score), and semi-quantitative cardiac function parameters (ΔHR(the difference between the maximum heart rate at load and the heart rate at rest), EDV(end-diastolic volume), ESV(end-systolic volume), and EF(ejection fraction)) at rest and at drug loading were compared between the two groups (Table 2). The results revealed that stress MBF and CFR were significantly lower and CAC score significantly higher in the CMVD group than in the non-CMVD group; the differences were statistically significant (P < 0.001 for all). There was no significant difference between the two groups in rest MBF and semi-quantitative cardiac function parameters (P > 0.05 for all).
Comparison of absolute quantitative and semi quantitative cardiac function parameters between the non CMVD group and CMVD group
Comparison of absolute quantitative and semi quantitative cardiac function parameters between the non CMVD group and CMVD group
Notes: Rest MBF is the resting myocardial blood flow; stress MBF is the load myocardial blood flow; CFR is coronary blood flow reserve, CACS is calcification score, ΔHR is the difference between the maximum heart rate at load and the heart rate at rest, EDV is end-diastolic volume, ESV is the end-systolic volume, EF is the ejection fraction, * is expressed as the difference between the two groups is statistically significant (P < 0.05).
Multivariate analysis of rest MBF, stress MBF, and CFR was conducted in terms of cardiovascular risk factors (gender, age, BMI, diabetes, hypertension, dyslipidemia, smoking history, drinking history, family history, and CAC score).
The results of analysis using the multiple linear regression model revealed that gender (female) may be an influencing factor for increased rest MBF and stress MBF (β= 0.328, 95% CI 0.233–0.423; P < 0.001; β= 1.287, 95% CI 0.703–1.870; P < 0.001, respectively), diabetes mellitus may be a risk factor for decreased stress MBF (β= –0.636, 95% CI –1.239––0.033; P = 0.039), and CAC score and hypertension may be risk factors for decreased CFR (β= –0.004, 95% CI –0.007––0.002; P = 0.002; β= –0.654, 95% CI –1.185––0.122, P = 0.017).
The results of analysis using the logistic regression model revealed that hypertension, family history, and CAC score may be risk factors for CMVD (OR = 7.323, 95% CI 1.171–45.806; P = 0.033; OR = 5.108, 95% CI 1.125–23.192, P = 0.035; OR = 1.012, 95% CI 1.003–1.021, P = 0.012, respectively).
Survival analysis
Follow-up results
Adverse cardiovascular events occurred in 20 patients with non-obstructive CAD. The PET/CT results and prognosis of patients with non-obstructive CAD are shown in Table 3. According to the criteria for determining abnormality, 10 of these 20 patients had a stress MBF of < 2.4 ml/(min·gm), 10 had a stress MBF of≥2.4 ml/(min·gm), 14 had a CFR of < 2.5, and 6 had a CFR of≥2.5. Of these 20 patients, 13 patients were assigned to the low-risk group (CAC score 0–10), while 7 were assigned to the moderate-risk group (CAC score 11–400). Of the 20, 1 patient underwent PCI stenting due to vascular stenosis, 2 were re-hospitalized because of chest pain, 1 had radiation shoulder pain, 1 had chest tightness, and 15 had continuous chest pain. In this study, the time at which these symptoms appeared for the first time after discharge was set as the follow-up deadline.
PET/CT results and prognosis of 20 patients with non obstructive coronary artery disease with recurrent adverse cardiovascular events
PET/CT results and prognosis of 20 patients with non obstructive coronary artery disease with recurrent adverse cardiovascular events
Notes: stress MBF is the load myocardial blood flow; CFR is coronary blood flow reserve, CACS is calcification score, d is the number of days.
The correlation between the results of 13N–NH3·H2O PET/CT and prognosis in the patients with non-obstructive CAD is shown in Table 4. The study revealed that, in the stress MBF < 2.4 ml/(min·gm) group, 10 of 21 patients made progress (progress rate = 47.62%), in the stress MBF≥2.4 ml/(min·gm) group, 10 of 49 patients made progress (progress rate = 20.41%), in the CFR < 2.5 group, 14 of 17 patients made progress (progress rate = 82.35%), in the CFR≥2.5 group, 6 of 53 patients made progress (progress rate = 11.32%), in the low-risk group (CAC score 0–10), 13 of 56 patients made progress (progress rate = 23.21%), and in the moderate-risk group (CAC score 11–400), 7 of 14 patients made progress (progress rate = 50%).
The correlation between the results of 13N–NH3·H2O PET/CT and prognosis in 70 patients with non obstructive coronary artery disease
The correlation between the results of 13N–NH3·H2O PET/CT and prognosis in 70 patients with non obstructive coronary artery disease
Notes: stress MBF is the load myocardial blood flow; CFR is coronary blood flow reserve, CACS is calcification score, * is expressed as the difference between the two groups is statistically significant (P < 0.05).
The prognosis was significantly poorer in the stress MBF < 2.4 ml/(min·gm) group than in the stress MBF≥2.4 ml/(min·gm) group, and the difference between the two groups was statistically significant (χ2 = 5.593, P < 0.05). The prognosis was significantly poorer in the CFR < 2.5 group than in the CFR≥2.5 group, and the difference between the two groups was statistically significant (χ2 = 27.404, P < 0.001). There was no significant difference in prognosis between the low-risk group (CAC score 0–10) and the moderate-risk group (CAC score 11–400) (χ2 = 3.690; P > 0.05 for all). These results suggest that a stress MBF of < 2.4 ml/(min·gm) and a CFR of < 2.5 are independent predictors of adverse cardiovascular events.
The survival analyses of stress MBF and CFR are shown in Figs. 1 2. The results revealed that survival was significantly poorer in the stress MBF < 2.4 ml/(min·gm) group and the CFR < 2.5 group than in the stress MBF≥2.4 ml/(min·gm) group and CFR≥2.5 group.
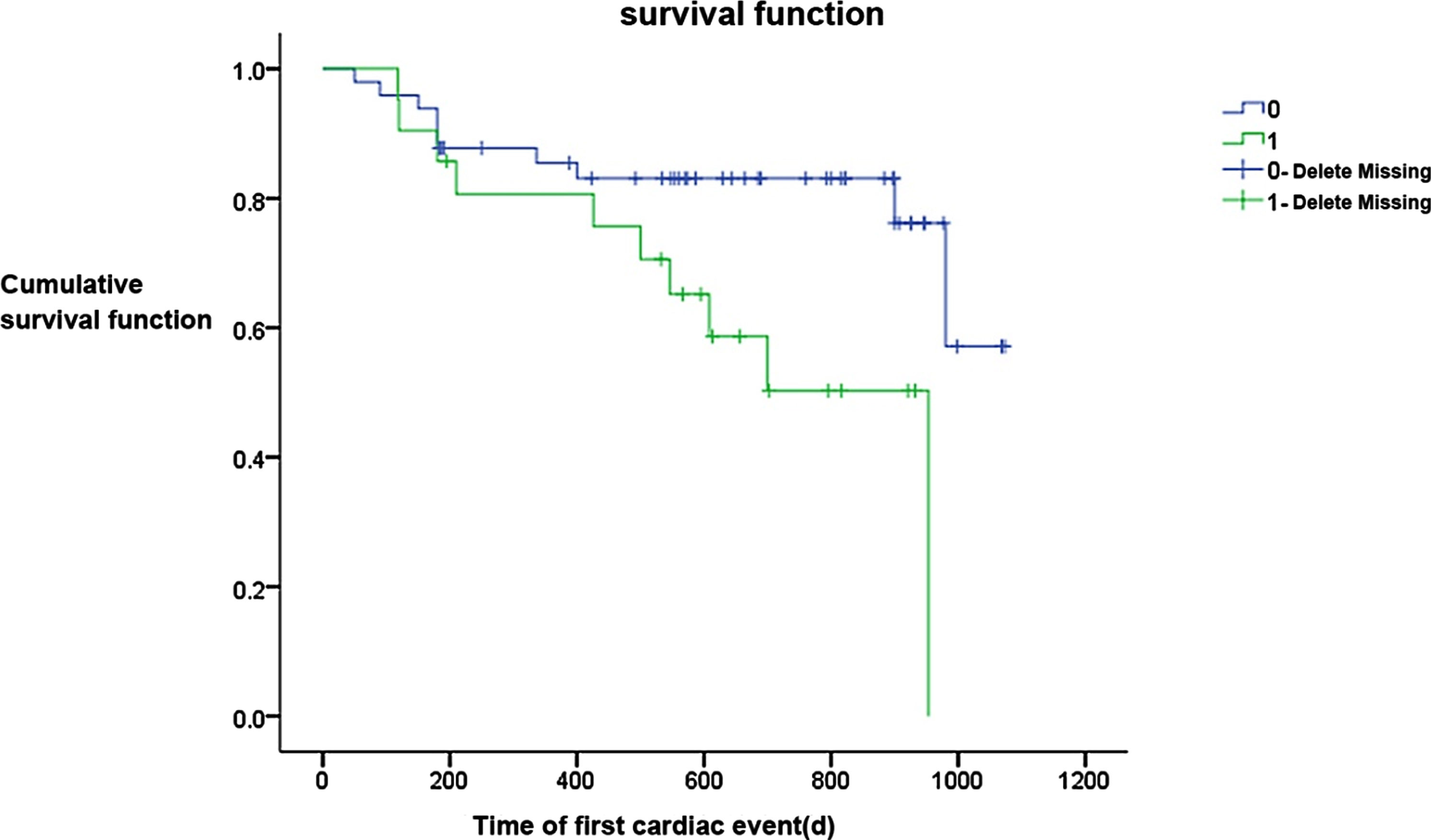
Comparison of Kaplan–Meier survival analysis between the stress MBF < 2.4 ml/(min·gm) group and the stress MBF≥2.4 ml/(min·gm) group.
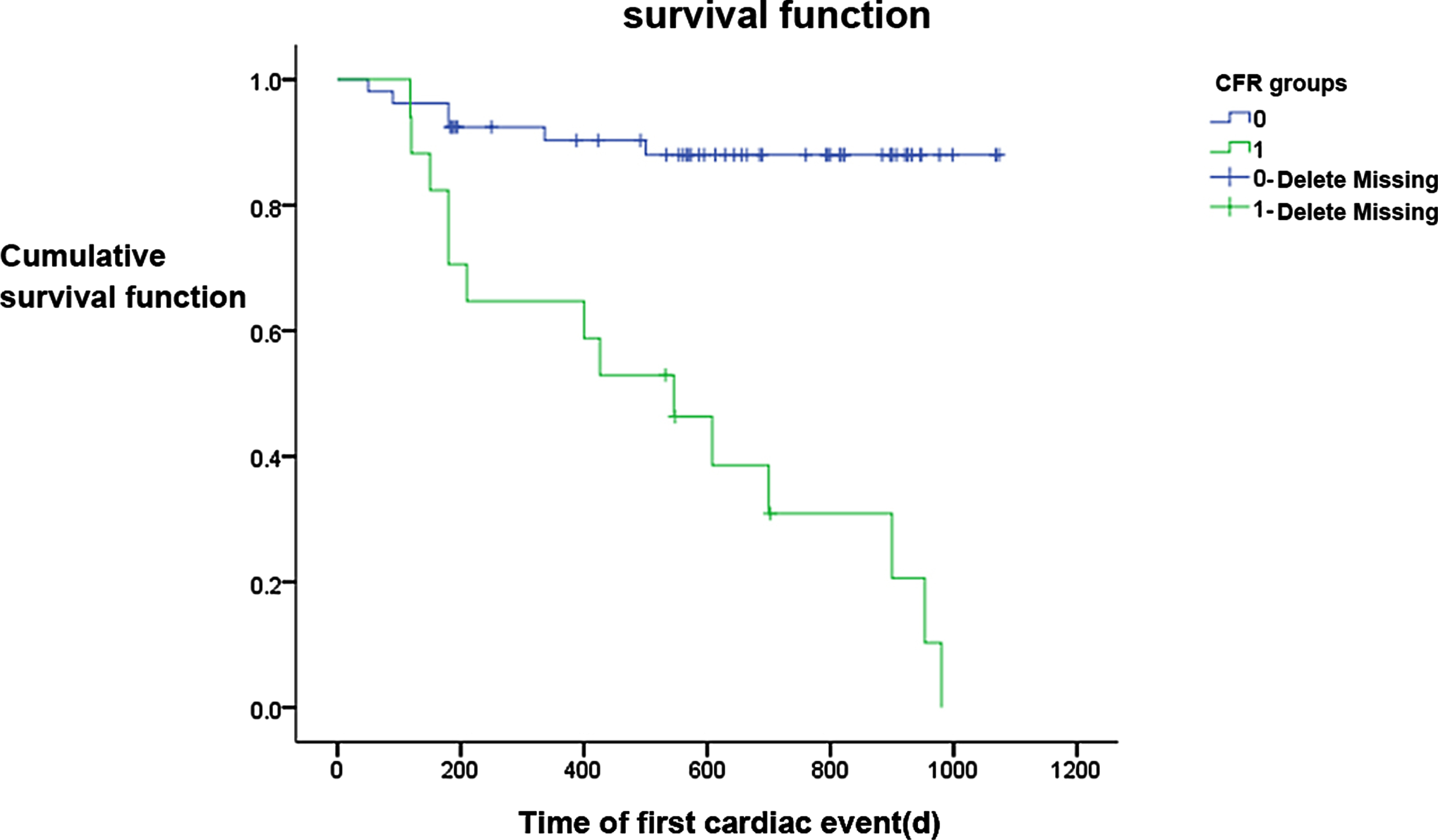
Comparison of Kaplan–Meier survival analysis between the CFR < 2.5 group and the CFR≥2.5 group.
The results of the Cox proportional hazard regression model revealed that gender (male, female), age (< 55 years, ≥55 years), BMI (< 25 kg/m2, ≥25 kg/m2), hypertension, dyslipidemia, smoking, drinking, and family history were not the main influencing factors for adverse cardiovascular events—diabetes was the main influencing factor. When other variables remained unchanged, the risk of adverse cardiovascular events in patients with diabetes was 0.326 times higher than in patients without diabetes (Table 5).
Cox regression analysis of survival time of patients
Cox regression analysis of survival time of patients
Notes: BMI is body mass index, * is expressed as the difference is statistically significant (P < 0.05).
The ROC curve analysis revealed that, when stress MBF was set to 2.535, the prognostic sensitivity was 78%, the specificity was 65%, and the area under the curve (AUC) was 0.782; when CFR was set to 2.595, the prognostic sensitivity was 94%, the specificity was 80%, and the AUC was 0.890 (Table 6). The AUC between 1.0 and 0.5 is of diagnostic value: the higher the value, the better the diagnosis effect.
Analysis of the best cut-off value of stress MBF and CFR
Analysis of the best cut-off value of stress MBF and CFR
Notes: stress MBF is the load myocardial blood flow; CFR is coronary blood flow reserve, AUC is the area under the ROC curve.
In 2013, the European Society of Cardiology (ESC) issued guidelines for the management of stable coronary artery disease (SCAD), which included angina caused by microvascular dysfunction into the coverage of stable angina [11]. In patients with suspected or confirmed CAD, CMVD caused by reduced coronary blood-flow reserve is very common; it is also the main reason a person is at high risk of major adverse cardiac events, such as myocardial infarction and cardiac death [12–15]. However, in patients with CAD without obstructive epicardium or a population with high cardiovascular risk (such as diabetes), some may also develop CMVD, resulting in adverse outcomes like repeated angina attacks and myocardial infarction [16, 17]. Therefore, it is of great clinical significance to effectively diagnose and evaluate CMVD at an early stage in order to intervene quickly and improve prognosis. Coronary blood-flow reserve provides a quantitative evaluation of the combined effects of epicardial coronary stenosis, diffuse atherosclerosis, and microvascular dysfunction; therefore, it has become an important index for the diagnosis of CMVD.
In the present study, the proportion of patients with a family history of cardiovascular disease was significantly higher in the CMVD group than in the non-CMVD group (58.8% vs. 20.8%, P < 0.05). This suggests that, for populations with a family history of cardiovascular disease, early screening, early prevention, and early intervention for cardiovascular risk factors can effectively reduce the incidence of cardiovascular disease. The present study also revealed that the proportion of patients with a CAC score of 11–400 was significantly higher in the CMVD group than in the non-CMVD group (29.4% vs. 5.7%, P < 0.05). One possible reason for this is that CAC score reflects the situation of coronary atherosclerosis: the higher the score, the more severe the degree of atherosclerosis of lumen, which reduces vasodilation function, resulting in the occurrence of CMVD.
The diagnostic and prognostic values of PET/CT in CMVD
At present, there is no uniform standard for PET/CT diagnosis of CMVD, although an index of CFR < 2.5 as reported in foreign studies is often used for diagnosis. The results of the present study revealed that stress MBF and CFR were significantly lower and CAC score significantly higher in the CMVD group than in the non-CMVD group, and all the differences were statistically significant (P < 0.05). The difference between the two groups in rest MBF was not statistically significant (P > 0.05). This shows that PET/CT can be used clinically for the early diagnosis of CMVD.
The present study also found no significant difference between the two groups in ΔHR, DBP(diastolic blood pressure), SBP(systolic blood pressure), EDV, ESV, and EF in rest and load state (P > 0.05 for all). The above results revealed that, compared with the absolute quantitative indexes of stress MBF and CFR, the semi-quantitative indexes of myocardial perfusion imaging have limited diagnostic value for CMVD.
One study has confirmed that a decreased response of MBF to diastolic blood pressure measured by PET can independently predict the development of CAD. Because PET can identify abnormal coronary microvascular function before vascular morphological changes, individuals with asymptomatic cardiovascular diseases who are at moderate and low risk can be further stratified and their prognosis understood early, allowing them to benefit from early prevention and treatment intervention [18, 19]. For 13N ammonia and 82Rb tracers, CFR < 2 is considered an independent prognostic cut-off value: when CFR is higher than this cut-off value, the prognosis is better [20]. In the present study, the univariate survival analysis of stress MBF and CFR of 13N–NH3·H2O PET/CT imaging of 70 patients with non-obstructive CAD was performed, the results of which showed that these two indexes are independent predictors of adverse cardiovascular events. This finding is inconsistent with those reported worldwide. The stress MBF and CFR were analyzed using an ROC curve, the results of which revealed that, when the cut-off values were 2.535 and 2.595, they had the highest sensitivity and specificity in predicting prognosis, all of them were slightly higher than those in previous studies. The reason for this may be that, (1) different characteristics of the study population led to different disease composition: most of the reported values were from foreign populations; (2) the adverse cardiovascular events in this study were mainly the recurrence of angina pectoris with chest pain as the main symptom, which is milder than the adverse cardiovascular events reported in the study on myocardial infarction or death, so the value was slightly higher than other research results. However, stress MBF and CFR can better predict prognosis.
Impact of cardiovascular risk factors
This study revealed that rest MBF and stress MBF were higher in women than in men, which is consistent with the results of several studies [21, 22]. Analysis suggests that premenopausal estrogens, especially 17 β-estradiol, reduces the incidence of CAD and the progression of CAD [23]. The potential coronary artery protection mechanisms of estrogens include effective regulation of plasma lipid changes (lowering plasma lipoprotein and low density lipoprotein (LDL) cholesterol, increasing high density lipoprotein (HDL) cholesterol), inhibition of cholesterol deposition in the arterial wall, and delay of the progression of coronary atherosclerosis. In addition, through the antagonistic effect of calcium and hormone-induced release of endothelium-derived relaxing factor and inhibiting contractile factor, it maintains vasodilation response to stimulation, increases cardiac output, reverses the vasoconstriction caused by acetylcholine, and improves myocardial ischemia induced by exercise in women [24–26].
The present study revealed that the average stress MBF of diabetic patients was 0.636 times lower than that of non-diabetic patients and the risk of adverse cardiac events was 0.326 times higher than that of non-diabetic patients; these differences were statistically significant. The results of many studies have shown that abnormal coronary artery microvascular function is common in diabetic patients with non-obstructive CAD [27–29]. Hyperglycemia and insulin resistance in diabetic patients can lead to the activation of multiple signaling pathways, an increase in inflammation and oxidative stress, damage to the coronary microvascular structure and function, an increase in coronary microvascular resistance, and a decrease in blood-flow perfusion under hyperemia; this leads to a decrease of coronary blood-flow reserve [30]. In addition, because of the impairment of monocyte function, the density of myocardial capillaries in diabetic patients is decreased, as a result of which the collateral circulation of the coronary artery is reduced and the blood supply is lowered. Compared with patients without diabetes, the risk of cardiovascular disease in patients with diabetes is significantly increased [31, 32]. Therefore, early detection, early intervention, and early treatment to ensure normal coronary microvascular function is vital for diabetic patients.
The present study also found that a history of hypertension was closely related to the decrease of CFR. The main reason for this may be changes to the microvascular structure of the coronary artery. Hypertension can thicken the intima media of the coronary artery microvascular wall and reconstruct the structure, reducing the distribution of the microvascular bed, increasing coronary microcirculation resistance, and decreasing microvascular relaxation capacity and CFR [33].
CAC score is often used to evaluate coronary atherosclerosis, which is closely related to the possibility of future adverse cardiovascular events. One study has found a negative correlation between circulating anticoagulant content and coronary artery diastolic function in patients without CAD [34]. The increase in CAC score was related to the occurrence of CMVD [35]. The results of the present study revealed that an increase in CAC score could lead to a decrease in CFR, which increases the risk of CMVD.
Although the present study found no significant difference in stress MBF between the age≥55 years old group and the control group, between the overweight/obese group and the control group, between the smoking history group and the control group, between the family history group and the control group, and between the moderate-risk (CAC score 11–400) group and the control group, stress MBF decreased in all groups.
Limitations of the study
The present study has three limitations. Firstly, a control group was not included and compared with the non-CMVD group, so it is not clear whether there was any difference between the two groups. Secondly, the study was a single-center population study in China, and it used a single-sample structure and a small sample size; therefore, its representation was poor and the influencing factors of MBF and CFR may be different in other populations. Lastly, because of the limited follow-up time, no cardiogenic death occurred, so the study mainly analyzed adverse cardiovascular events, such as the recurrence of angina pectoris.
Conclusion
The absolute quantitative MBF and CFR values of 13N–NH3·H2O PET/CT were more effective than semi-quantitative indexes in the diagnosis of CMVD. Female patients were found to have a higher rest MBF and stress MBF than male patients. Diabetes was identified as the main factor affecting stress MBF, while hypertension, family history, and CAC score were important factors influencing CFR.
In summary, CFR measured by 13N–NH3·H2O PET/CT can more effectively diagnose CMVD and evaluate the prognosis of adverse cardiovascular events. CFR’s prediction value is most accurate when it is set to 2.595. Gender, diabetes, hypertension, family history of cardiovascular diseases, and CAC score are important factors influencing CMVD.
Future studies should expand the sample size, extend the follow-up time, and conduct more in-depth research.
Funding
This study was supported by grants from the Natural Science Foundation of China (81671724 to Dr Li Sijin).