
Abstract
BACKGROUND:
Although the number of vascular surgeries performed is increasing, the incidence of complications associated with this surgery has not improved and re-operations are frequently required. Thrombosis in a vessel is the most hazardous postoperative complication.
OBJECTIVE:
The aim of this study was to evaluate the anti-thrombotic and anti-inflammatory effects of sulodexide compared to aspirin in a rat model.
METHODS:
We divided the animals into three groups (sham (saline), aspirin, and sulodexide). The abdominal aorta was surgically opened and closed, primarily with 8/0 Prolene sutures. Postoperatively, saline, aspirin, or sulodexide was administered by oral gavage for 14 days to the rats. The degree of neovascularization, thrombus, calcification, inflammatory infiltrates, and fibrosis were analyzed histopathologically by hematoxylin and eosin staining.
RESULTS:
There was no significant difference in the incidence of postoperative thrombogenesis, but less calcification and inflammatory infiltrates were observed in the sulodexide group compared to the aspirin group. Histopathologic score revealed less infiltration of inflammatory cells and mild calcification for the sulodexide group (0.17±0.41 and 1.33±0.52, respectively) compared to the aspirin group (0.67±0.52 and 1.67±0.52, respectively) at days 14.
CONCLUSIONS:
This study offers the possibility that sulodexide could be used as an aspirin substitute for the postoperative management of vascular patients, with low gastrointestinal discomfort. In addition, it may also offer reduced postoperative calcification and inflammation.
Introduction
The mortality due to cerebrovascular and cardiovascular disease has increased to more than 1.68 million deaths per year in the European Union. In 2018, the number of inpatients with diseases of the circulatory system discharged from hospitals across the EU was 10.4 million [1, 2]. These diseases often require revascularization accomplished through vascular and endovascular surgery with various types of devices and grafts. Almost all patients who undergo vascular surgery using any type of graft need postoperative anti-thrombotic therapy using antiplatelet agents. Although anticoagulants have been used to inhibit intrinsic thrombogenicity in patients with implanted vascular grafts [3–6], unfortunately, thrombotic complications causing graft failure have not improved. Therefore, the choice of good antiplatelet agents is one of the most important postoperative issues worldwide.
Vascular thrombosis can be caused by the synergistic interaction of endothelial damage, hypercoagulability, and the rheologic modification of blood flow [7]. Currently, heparin and aspirin are used to prevent vascular thrombosis immediately after surgery. After that, aspirin is used for long-term administration in many patients because heparin is difficult to use continuously [8–10]. However, aspirin also has the disadvantages of inducing gastrointestinal mucosal injury, ulcers or erosion, and bleeding complications [11–13].
Recently, antithrombotic combination therapy, which has a more diverse mechanism than monotherapy, has been the preferred therapy for thrombotic complications. Although dual antiplatelet therapy with aspirin and clopidogrel has shown no increased risk of major bleeding in patients with ST-segment elevation myocardial infarction [14], an increase in the risk of major bleeding in patients with ischemic stroke or atrial fibrillation has been reported [15, 16]. In addition, this dual antiplatelet therapy demonstrated inferior clinical outcomes against warfarin monotherapy, but without an increased risk of major hemorrhage [16]. The combination of warfarin plus aspirin-treated patients showed a reduction in death, nonfatal reinfarction, coronary artery reocclusions, or thromboembolic stroke compared to aspirin alone [17, 18]. While efficacious, the combination of warfarin plus aspirin is less commonly recommended because it is associated with an increased risk of bleeding [19]. The combination of cilostazol plus aspirin could also inhibit platelet aggregation [20], but has not been shown to be more effective than aspirin monotherapy. Clopidogrel, warfarin, and cilostazol, and warfarin monotherapy are more effective than aspirin. Warfarin can reduce the risk of venous thromboembolism recurrence, but also has been shown to increase bleeding risk [21]. Therefore, new drug candidates for patients with vascular ischemic events need to be identified. Sulodexide has a prolonged half-life and a systemic anticoagulant effect, which is less potent but also less likely to cause hemorrhage [22]. In addition, sulodexide treatment was more effective than aspirin in reducing venous thromboembolism recurrence [23].
This study investigated sulodexide as an aspirin substitute with low gastrointestinal effects for the postoperative management of vascular patients by evaluating the effect of sulodexide compared to aspirin in a thrombotic rat model.
Methods
Animals
All experiments and animal handling procedures were approved by the Animal Experimental Ethics Committee of Korea University (IACUC No. KOREA-2019-0061). All protocols were performed in accordance with the relevant guidelines and regulations. In total, 18 Sprague-Dawley male rats (4 to 6 weeks old, 200–300 g) were housed in cages and maintained at 23°C with 12h light/dark cycles under specific pathogen-free conditions.
Experimental design
Arterial sutures are widely used in vascular surgeries, but they may be bleeding problems in the needle hole in patients who are currently using anticoagulants. So we used the abdominal aorta incision and simple closure as a rat model of our syudy [24]. Each rat was anesthetized with isoflurane or alfaxalone 30 mg/kg + xylazine 10 mg/kg intra-peritoneally. A midline abdominal incision was made and the infrarenal abdominal aorta was exposed under standard sterile conditions. Heparin (50 IU/kg) was injected intravenously. After 3 minutes of heparin injection, the abdominal aorta was cross-clamped and opened longitudinally by an incision about 3 cm long. Then, the aortic diameter was checked and the opened aorta was closed again as a manner of continuous suture with 8/0 prolene. After confirming blood flow through the abdominal aorta, meticulous bleeding control was performed in the post-de-clamping period. The wound was closed layer by layer. The animals were divided into three groups: sham (saline, n = 6), aspirin (aspirin 10 mg/kg/day, n = 6), and sulodexide (sulodexide 0.4 mg/kg/day, n = 6). The animals recovered from surgery and were treated with saline, aspirin, or sulodexide as anticoagulants for up to 14 days postoperatively. These dosages which are applied to the rats are the same dosages we have administered to the patients. After 14 days, the aorta and surrounding tissues were harvested for histopathologic examination after euthanization of the operated rats. A schematic diagram of the experimental design is shown in Fig. 1.

Schematic diagram of the experimental design.
The aorta and surrounding tissues were fixed in 4%paraformaldehyde and then embedded in paraffin for hematoxylin and eosin (H&E) staining. The aorta and surrounding tissue sections (4μm thick) were stained sequentially with H&E. After staining, the slides were mounted with Canada balsam (Show Chemical Co. Ltd., Tokyo, Japan).
Histopathology
Histologic examinations were performed by a pathologist in a blinded manner. The analysis and measurements were performed around the sutured area. The sections for histopathologic analysis were stained with H&E. Histopathologic assessment of the aorta and surrounding tissues included an estimation of the luminal thrombus, intimal hyperplasia, neovascularization, vascular smooth muscle cell proliferation, inflammatory infiltrates, and aortic wall fibrosis.
Histopathology scoring
Histopathology grading of neovascularization, thrombi, calcification, inflammatory, and fibrosis was evaluated by a pathologist in a blinded manner. Although these were relative evaluations, the grades for each individual aorta and surrounding tissue were classified as 0 for none; 1 for mild; 2 for moderate; and 3 for severe findings on the H&E stained sections. Then, the histopathology grade for each cross-section was calculated as the sum of the individual histopathology scores in the examined sections divided by the number of rats.
Statistical analysis
The data were statistically analyzed using Prism 5 software (GraphPad Software). All values are presented as the mean±standard deviation. Statistical significance was determined using the Mann-Whitney test. A P-value of < 0.05 indicated statistical significance.
Results
Histopathological analysis
To evaluate the postoperative effects of sulodexide on the operated aorta and the surrounding tissue, the histopathologic findings of neovascularization, thrombus, calcification, inflammatory, and fibrosis were compared to those of aspirin for 14 days postoperatively. At the end of the experiment, there was no significant difference in body weight among each group of animals (data not shown).
The sham group revealed higher calcification and inflammatory infiltrates compared to the aspirin and sulodexide-administered rats (Fig. 2, 3). Among these three groups, only the rats in the sham group had fibrosis (data not shown).
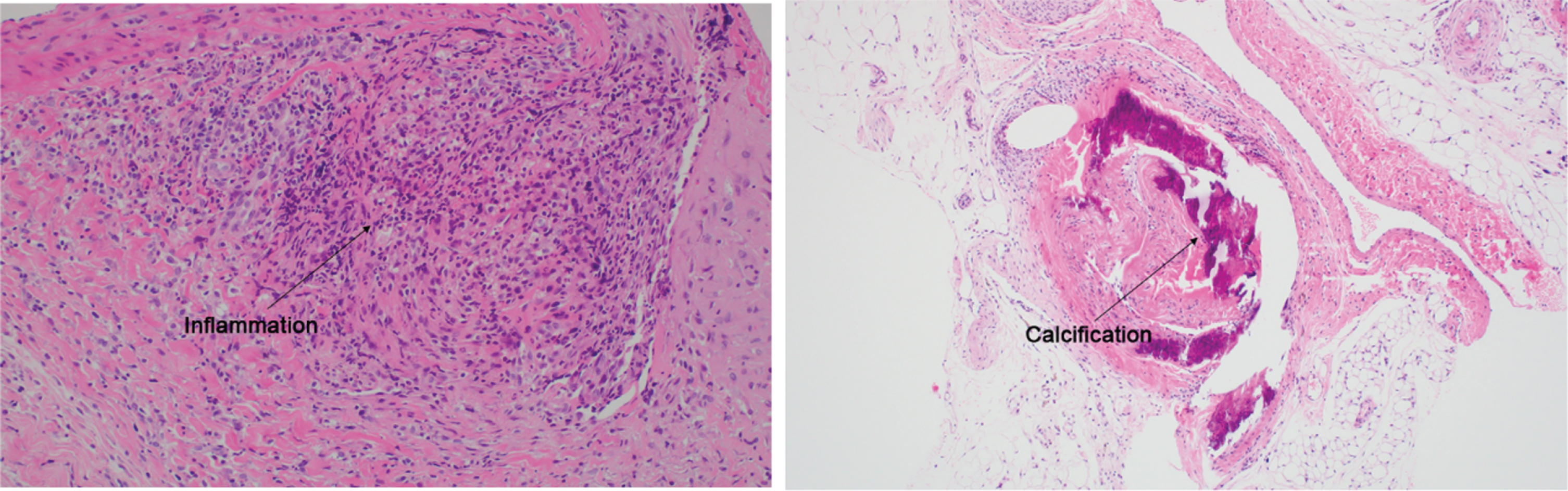
Histopathological observations in the sham group. Representative images of H&E stained aorta and surrounding tissue after 14 postoperative days. Original magnification, 100x.
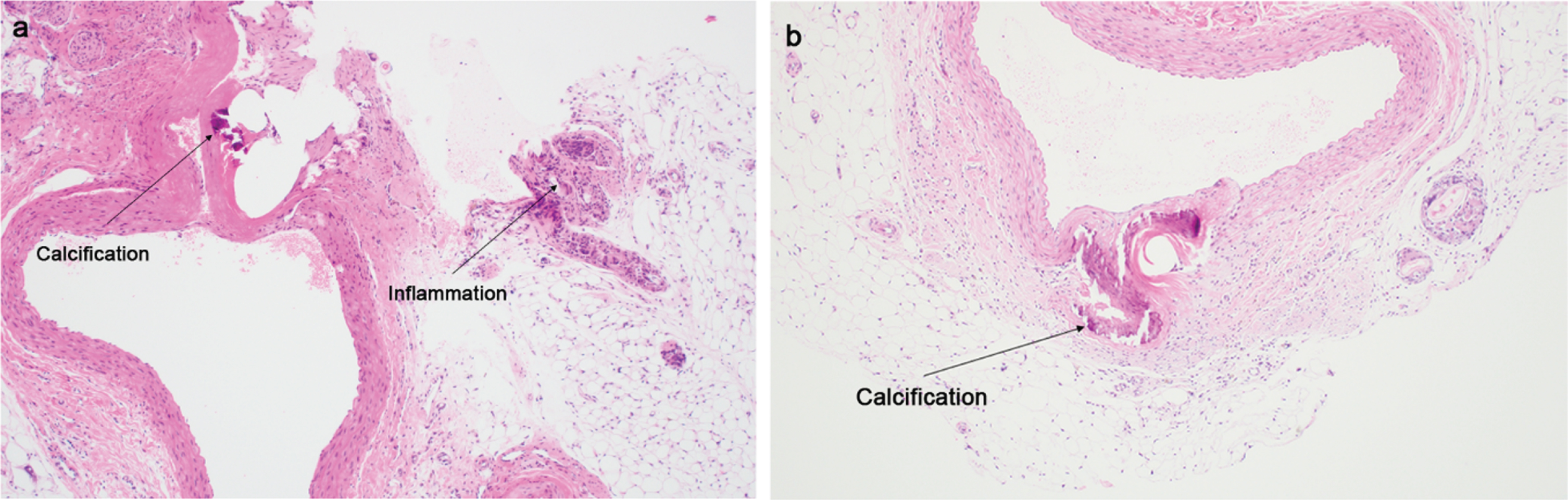
Histopathological observations in the (a) aspirin and (b) sulodexide groups. Representative images of H&E stained aorta and surrounding tissue after 14 postoperative days. Original magnification, 100x.
The histopathologic analysis did not show any evidence of neovascularization and thrombus formation in the aspirin and sulodexide groups. Aortic calcifications appear as violet deposits in histological preparations stained with H&E. Large calcifications may ulcerate the intima and protrude into the lumen, eventually becoming occluding polypoid masses. Furthermore, these lesions are starting points for the development of thrombi [25]. Calcification was seen less in the aspirin and sulodexide groups than in the sham group (Fig. 2, 3). Calcification was seen less in the sulodexide group than in the aspirin group (Fig. 3, 4).
Inflammation could be involved in the pathogenesis of chronic thrombogenesis [26]. Lymphocytes, macrophages, and neutrophils were observed in the sham group (Fig. 2). Inflammatory cell infiltration was less in the aspirin and sulodexide groups compared to the sham group (Fig. 2, 3). The inflammatory infiltrates were less in the sulodexide group compared with the aspirin group (Figs 3, 4). However, there was no statistical difference in the sulodexide group compared to the aspirin group (Fig. 4).
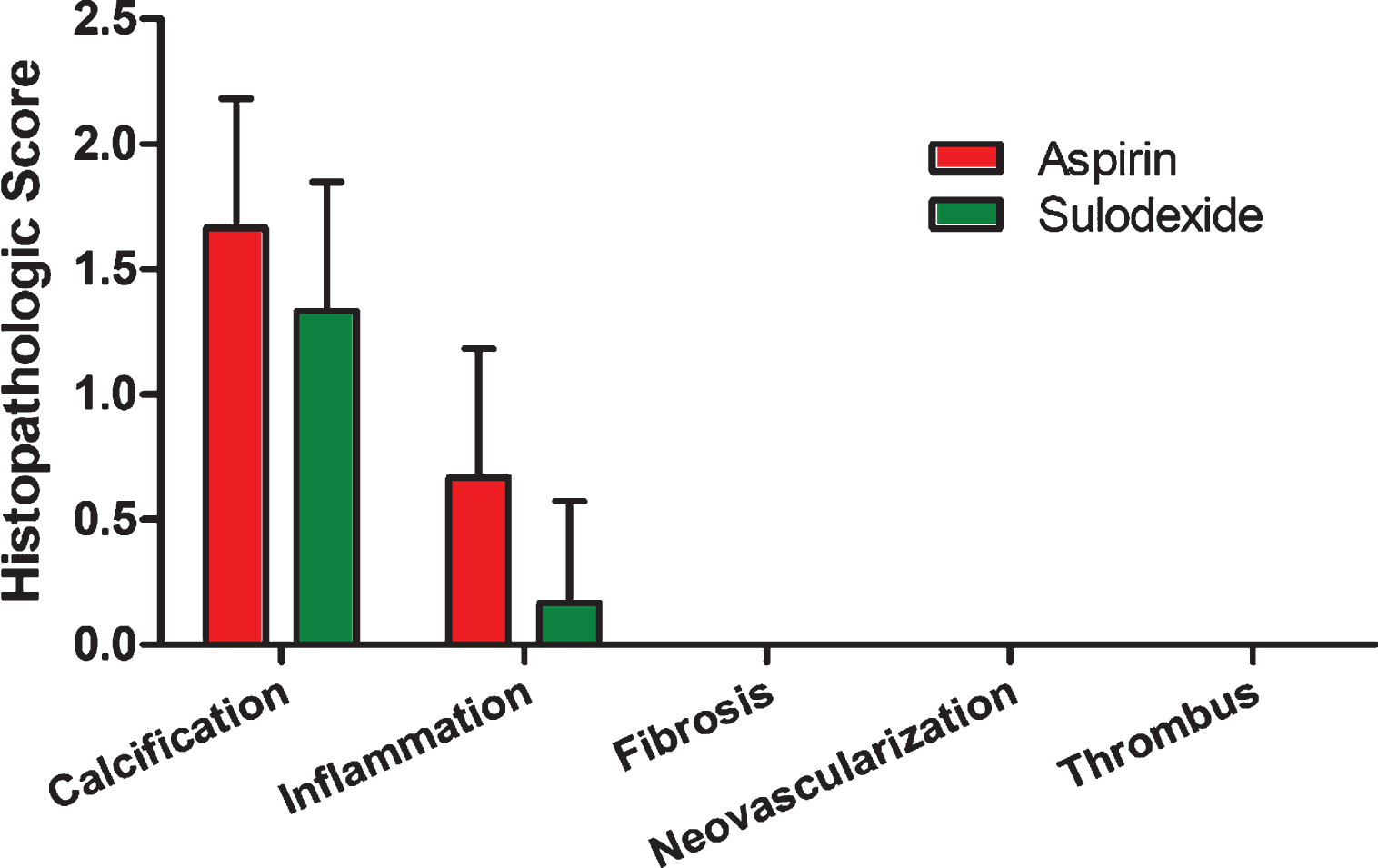
Histopathologic scores in the aspirin and sulodexide groups. The data are expressed as the mean±standard deviation.
Antiplatelet drugs have been used clinically for the treatment and prevention of vascular ischemic events in various manners such as aspirin monotherapy or dual combination therapy. However, antiplatelet drugs have the advantage of suppressing blood clots in blood vessels, but they also have side effects that increase bleeding complications [27]. To overcome these limitations, antiplatelet drugs with a low but sustained antithrombotic activity with negligible hemorrhagic risk, and endothelial-protecting and profibrinolytic effects are needed. The present study evaluated the anti-thrombotic and anti-inflammatory activity of sulodexide compared to aspirin in a rat model. Coagulation and immune system between rats and humans are difference. The blood coagulation system is extremely rapid in the rat [28]. However, maintaining blood pressure and homeostasis were similar in rats and humans [29]. Therefore, vascular disease rat model has long been investigated.
Sulodexide is comprised of 20%dermatan sulfate with an affinity for heparin cofactor II, in combination with 80%heparan sulfate with an affinity for antithrombin III, both of which exert antithrombotic and antithrombin activity [30–32]. Sulodexide inhibits thrombin activity by affecting heparin cofactor II and antithrombin III. A lower dose of sulodexide was shown to achieve an equivalent antithrombotic effect as a higher dose of heparin [33, 34]. Moreover, sulodexide is very different from heparin due to its prolonged half-life and systemic anticoagulant effect, which is less potent but associated with a lower risk of hemorrhage, making sulodexide a drug with great pharmacologic interest and suitable for the prophylaxis and treatment of vascular disease [22, 35]. A study by Buchanan et al. [34] reported that the incorporation of fibrin into the thrombus was significantly less after the injection of sulodexide. In this study, the aspirin and sulodexide-treated groups did not show evidence of neovascularization and thrombus in the rat thrombotic model.
Inflammatory cell infiltration in thrombotic lesions was involved in the development and progression of chronic thrombogenesis [26]. Sulodexide showed anti-inflammatory and endothelial protective properties in patients with chronic venous disease [36, 37]. Aspirin was associated with severe bleeding complications in rare cases (1 in 1,000 patients/year) and poor gastric tolerance to low-dose aspirin has been reported [35, 38]. However, sulodexide has less gastrointestinal disorders than aspirin. In this study, the inflammatory cell infiltration was less in the sulodexide group than in the aspirin group. However, there was no statistical difference between the sulodexide group and the aspirin group.
Thrombus and fibrosis may be factors that induce structural degeneration including calcification [39]. Vascular calcification occurs pathologically in atherosclerosis, diabetes, and chronic renal disease as well as in the normal aging process [40–42]. In this study, less calcification was observed in the sulodexide group compared to the aspirin group. Therefore, treatment with sulodexide may improve the clinical symptoms associated with calcification, inflammatory infiltrates, and fibrosis in patients with vascular disease.
Although general homeostasis was similar in rats and humans, we know there’s differences in coagulation and immune system between rats and humans, which undoubtedly limit the transferability of the study results to humans. This is a limitation in our study.
Conclusions
Our study revealed that sulodexide had acceptable and relatively superior anti-thrombotic and anti-inflammatory effects in the early postoperative stages of vascular surgery compared to aspirin. Considering the lower gastrointestinal side effects and bleeding tendency of sulodexide, sulodexide may be a safe and effective aspirin substitute for postoperative antiplatelet therapy in vascular patients.
Footnotes
Acknowledgments
This work was partly supported by Institute of Information & communications Technology Planning & Evaluation (IITP) grant funded by the Korea government (MSIT) (No. 2020-0-00228, Development of design software and 3D printing based manufacturing process for customized freeform artificial vascular graft) and the Aju Pharm Corporation fund. No funding body had any role in the study design, data collection, analysis, interpretation, or writing of the manuscript.
Author contribution
SHS performed molecular experiments, analyzed data, and drafted the article. TSK, JWK, and SMY performed the experiments. TSK had played the leading role in operations for rats. WMJ supervised the study, obtained funding, guided the analyses of data, and edited the manuscript and critically revised the manuscript for important intellectual content. All authors have read and agreed to the published version of the manuscript.