
Abstract
BACKGROUND:
Transesophageal echocardiography (TEE) as a guiding tool for edge-to-edge transcatheter tricuspid valve repair (EETVr) using MitraClip (Abbott Vascular, Santa Clara, USA) may not offer sufficient image quality in a significant proportion of patients.
OBJECTIVES:
Intracardiac echocardiography (ICE) as additional guiding tool in EETVr with the MitraClip device.
METHODS:
Appropriate angulations of the ICE catheter to visualize each commissure of the tricuspid valve were established in 3D printed heart models. In a single tertiary-care center ICE was used to support EETVr as additional guidance when TEE image quality was insufficient. Procedural safety and outcomes up to 30-days were compared between ICE/TEE and TEE only guided patients.
RESULTS:
In 6 of 11 patients (54.5%) undergoing EETVr with MitraClip TEE alone was unsatisfactory, necessitating additional ICE guidance. In 4 of these 6 patients ICE enabled a successful completion of the procedure. The steering maneuvers identified in the 3D models were well applicable in all patients, providing examples for potential future ICE implementation in EETVr. Under both TEE alone (n = 5) and ICE (n = 6) guidance the rate of procedural complications was 0%. According to vena contracta values at discharge significant TR reduction was achievable in the treated cohort (p = 0.011). At 30-days follow-up one patient (ICE guided) died following global heart failure, not associated with the procedure itself.
CONCLUSIONS:
ICE guidance may offer an additional tool to guide EETVr with the MitraClip device in patients with poor TEE quality, as it enables successful results without impairing procedural safety.
Keywords
Introduction
Transcatheter treatment of severe tricuspid regurgitation (TR) is rapidly evolving as it may offer a potential solution for high surgical risk patients currently lacking other options [1]. Promising results have been reported for the MitraClip device (Abbott Vascular, Santa Clara, USA), originally designed for edge-to-edge repair of mitral regurgitation [2–4]. According to the early results of the TRILUMINATE clinical trial, edge-to-edge tricuspid valve repair (EETVr) is able to significantly reduce TR and can improve quality of life as well as patients’ symptoms [5].
In order to allow safe and precise clip delivery, imaging-based guidance offering high temporal and spatial resolution is required. Transesophageal echocardiography (TEE) is well established in mitral interventions but due to the anatomical location of the valve it may be less reliable in terms of image quality in percutaneous tricuspid repair [6–8]. Transthoracic echocardiography (TTE) may be an alternative, but image quality can still be limited and increased radiation exposure for the echocardiographer has to be taken into account [9]. Intracardiac echocardiography (ICE) is an additional option to guide structural heart procedures and may be promising in EETVr as the ICE probe can be placed in close anatomical relation to the valve [10–12].
Thus, with this study we aimed to assess the feasibility and effectiveness of ICE in guiding EETVr, especially in patients where TEE guidance alone does not allow a safe and successful completion of the procedure.
Methods
Patient population
The present study is a single-center experience of patients undergoing EETVr with the MitraClip device (Abbott Vascular, Santa Clara, USA) using ICE/TEE or TEE alone guidance.
All patients underwent TTE, TEE as well as left and right heart catheterization as a routine workup.
In general, percutaneous TR repair was considered in patients with severe TR, associated with symptoms of right heart failure. The presence of severe pulmonary hypertension (systolic pulmonary artery pressure >60 mmHg) was predefined as a contraindication. All patients were discussed in an interdisciplinary heart team meeting and deemed inoperable or at a very high surgical risk. EETVr was offered as an experimental treatment option in all patients. Clinical outcomes of all patients were followed-up for at least 30 days after the procedure.
Ethical approval for data collection was obtained from the local institutional review board (EA4/079/17) and the study was conducted in accordance with the Declaration of Helsinki. All patients gave written informed consent to the procedure.
Baseline echocardiography
All patients underwent TTE and TEE using commercially available equipment (Philips iE33 and EPIQ 7, Philips Healthcare, Andover, MA, USA; GE Vivid 7, GE Healthcare, Milwaukee, WI, USA) with detailed screening of the tricuspid valve apparatus. Tricuspid valve anatomy including the underlying TR pathology was carefully evaluated. Semiquantitative methods as well as vena contracta were used to quantify TR before and after clip implantation [13].
Procedure
All procedures were performed under general anesthesia and access was gained from the right femoral vein in all patients. Combined mitral- and tricuspid-repair using the MitraClip device (Abbott Vascular, Santa Clara, USA) was performed in 5 patients whereas 6 patients underwent tricuspid repair only. In patients who underwent a double valve intervention, mitral-valve repair was performed first as previously described [14].
For tricuspid-repair the 24F guiding catheter was placed in the right atrial cavity, pointing towards the superior vena cava. Heparin was administered to achieve a clotting time between 250 and 350 seconds and was maintained throughout the procedure. The clip delivery system (CDS) was introduced and aligned according to the targeted commissure, using fluoroscopy and TEE irrespective of the visibility of the tricuspid valve. In patients where TEE showed significant limitations the CDS/clip was oriented according to the anticipated location of the commissure of interest. Furthermore, ICE was used as an additional imaging tool with the primary intention to support controlled and safe grasping of the leaflets.
Intracardiac echocardiography
Intracardiac echocardiography was used in patients where TEE image quality was insufficient to support a safe procedure. The ICE Catheter (View Flex™, St. Jude Medical/Abbott Vascular, Santa Clara, USA; used with an ACUSON X700 ultrasound machine [Siemens Healthineers, Erlangen, Germany]), which features intuitive four-way directional control, was introduced from the left femoral vein. The four-way directional control has the option of either left-right (L/R knob) or posterior-anterior (P/A knob) deflection. 3D imaging modalities were not available with the used device. After advancing the probe into the right atrium under fluoroscopic guidance, the position was carefully adjusted until the grasping area was displayed (Fig. 1).

Fluoroscopic orientation of the intracardiac echocardiography (ICE) probe in an anteroposterior fluoroscopy projection. Orientation of the ICE probe to visualize the anteroseptal commissure in a patient with previous transcatheter aortic valve implantation, sternal cerclages following cardiac surgery and transesophageal echocardiography probe in place (a). Orientation of the ICE probe to visualize the posteroseptal commissure in a patient with pacemaker leads in place, following implantation of a first clip in the anteroseptal position (b). Black arrows are pointing at the ICE probe.
To identify the appropriate steering maneuvers of the ICE probe with respect to the commissure, 3D heart models were fabricated in three of the patients, who underwent ICE guided TR repair (screening transoesophageal echocardiograms showed poor image resolution in these individuals). A modified Makerbot Replicator 2X (MakerBot Industries, New York, USA) was used to print the models. The Standard triangulation language (STL) files were generated from cardiac computed tomography datasets using Osirix lite (Pixmeo SARL, Bernex, Switzerland) and Autodesk Meshmixer (Autodesk, San Rafael, California, USA) to edit the DICOM files. Images were selected at end systole defined by the smallest right ventricular dimensions during the recorded cardiac cycle. All 3D Models were fabricated with Acrylnitril-butadien-styrol (ABS). The tricuspid leaflets were manufactured by silicone molding, whereat the mold was fabricated by 3D printing, using TEE based measurements.
Results
Patient population
A total of 11 patients were considered suitable to undergo percutaneous EETVr with the MitraClip device. All patients were at high surgical risk and suffered from at least moderate pulmonary hypertension. In 6 of these patients ICE was used to support the implantation, as visibility of the tricuspid valve using TEE was not sufficient.
Baseline characteristics of all treated patients are depicted in Table 1. Mean age of the patient cohort was 79.5 years and 6 (54.5%) of the patients were female. All 11 patients suffered from functional TR. Two patients had right ventricular pacing leads traversing the tricuspid valve, without being the predominant cause of TR.
Baseline characteristics
Baseline characteristics
Data are presented as mean±standard deviation or number (%). LVEF left ventricular ejection fraction, PAP pulmonary artery pressure, RV right ventricular, TAPSE tricuspid annular plane systolic excursion, TR tricuspid regurgitation, VC vena contracta.
Apart from distribution between the sexes, baseline characteristics were without significant differences, comparing patients in whom the procedure additionally was guided by ICE with those in whom TEE guidance alone was used.
The 3D printed models were used to find appropriate angulations of the ICE probe in accordance to the targeted commissures (Fig. 2, Supplemental Figures 1–3).
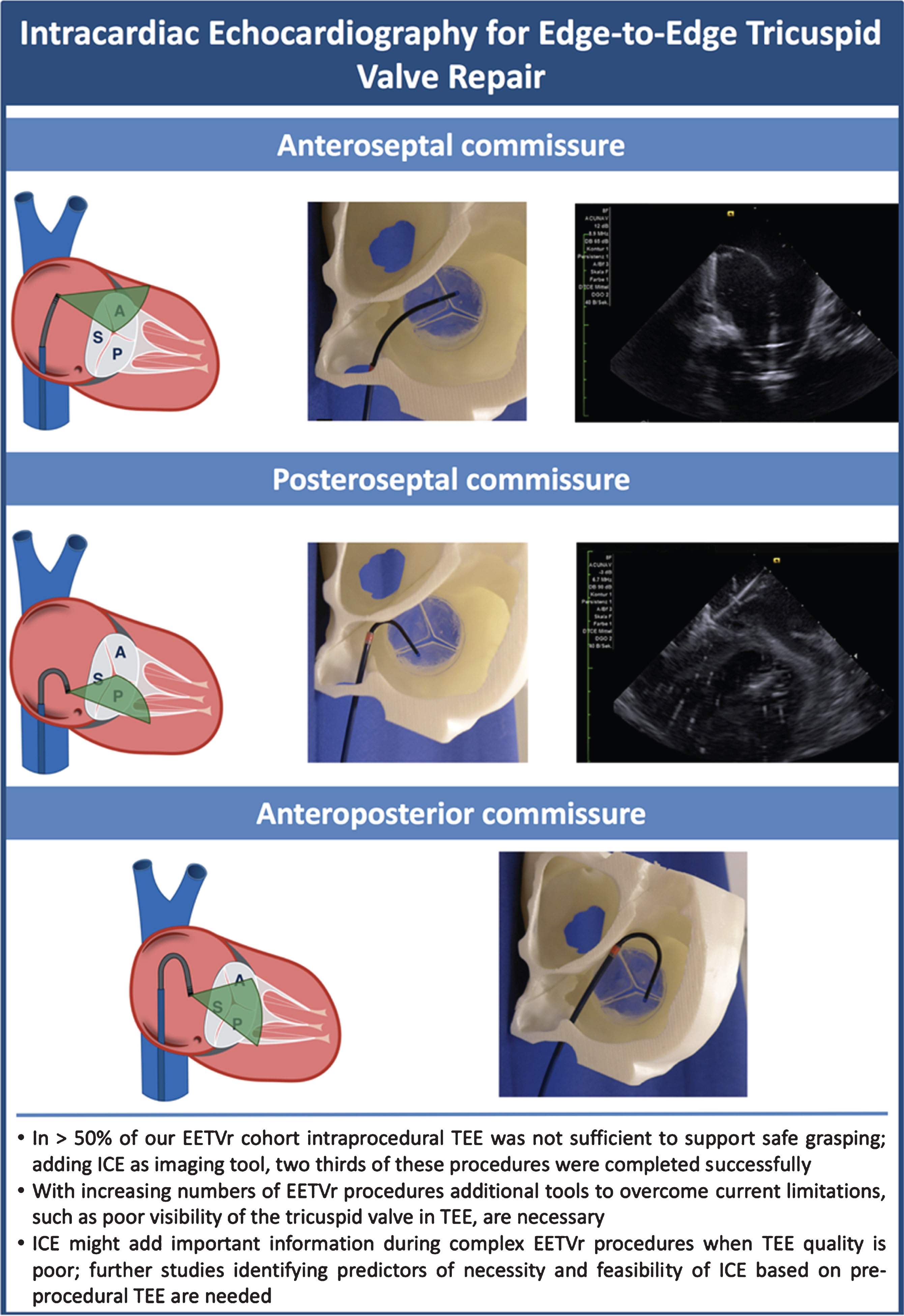
Illustration of intracardiac echocardiography (ICE) for edge-to-edge tricuspid valve repair. Graphics depicting different catheter angulations to visualize respective commissures are presented along with according images of the ICE catheter inside the 3D printed heart model and actual ICE images. ICE images of the anterioposterior commissure are not available since all patients in our study underwent treatment of the anteroseptal and posteroseptal commissures.
Different positions and angulations of the ICE catheter were identified: To visualize the anteroseptal commissure the probe was advanced into the superior portion of the right atrium, angulated slightly anterior (P/A knob) and towards the right atrial free wall (L/R knob) until the clip arms and the leaflets were visualized. Great care needs to be taken not to enter the right atrial appendage (Fig. 3, Supplemental Figure 1, Supplemental Video 1). To display the posteroseptal commissure, the L/R deflection was further increased from position (a) and the probe was slowly retracted until the posterior and the septal leaflets were visualized in an upside-down position (Fig. 4, Supplemental Figure 2, Supplemental Video 2). To visualize the anteroposterior commissure the probe was placed higher in the RA compared to (a), with increased flection on the P/A and the L/R knob (Fig. 2, Supplemental Figure 3).
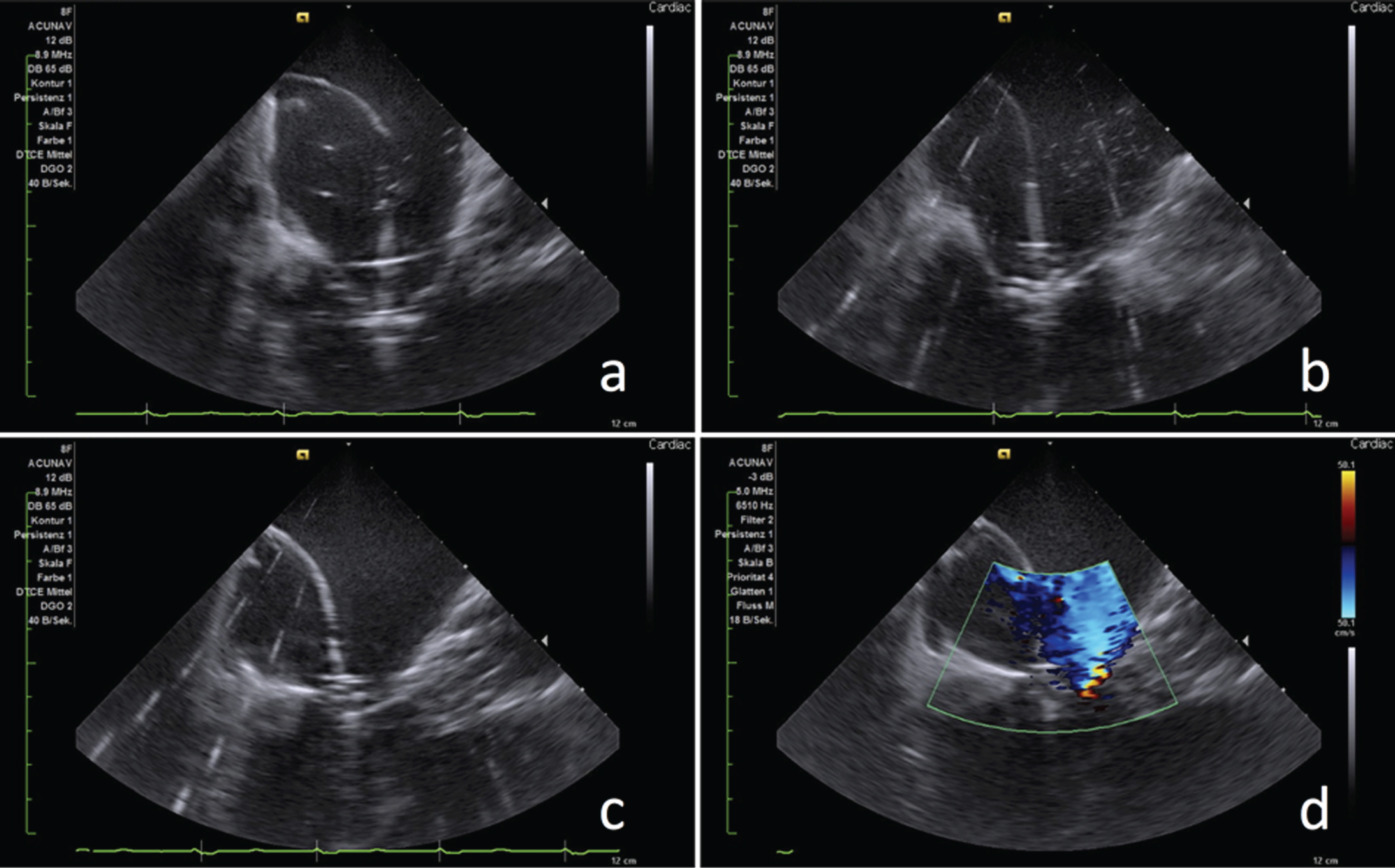
ICE guided grasping maneuver at the anteroseptal commissure. The anterior and the septal leaflets in relation to the MitraClip device as well as a previously implanted TAVR prosthesis are clearly visible. Both leaflets resting on the clip arms (a) and after lowerig the grippers with sufficient leaflet material inside the clip are displayed (b). Cinching of the annulus is clearly visible after closing the clip (c). Color doppler can assess the situation before the clip is released (d). (For moving images also see Supplemental Video 1).
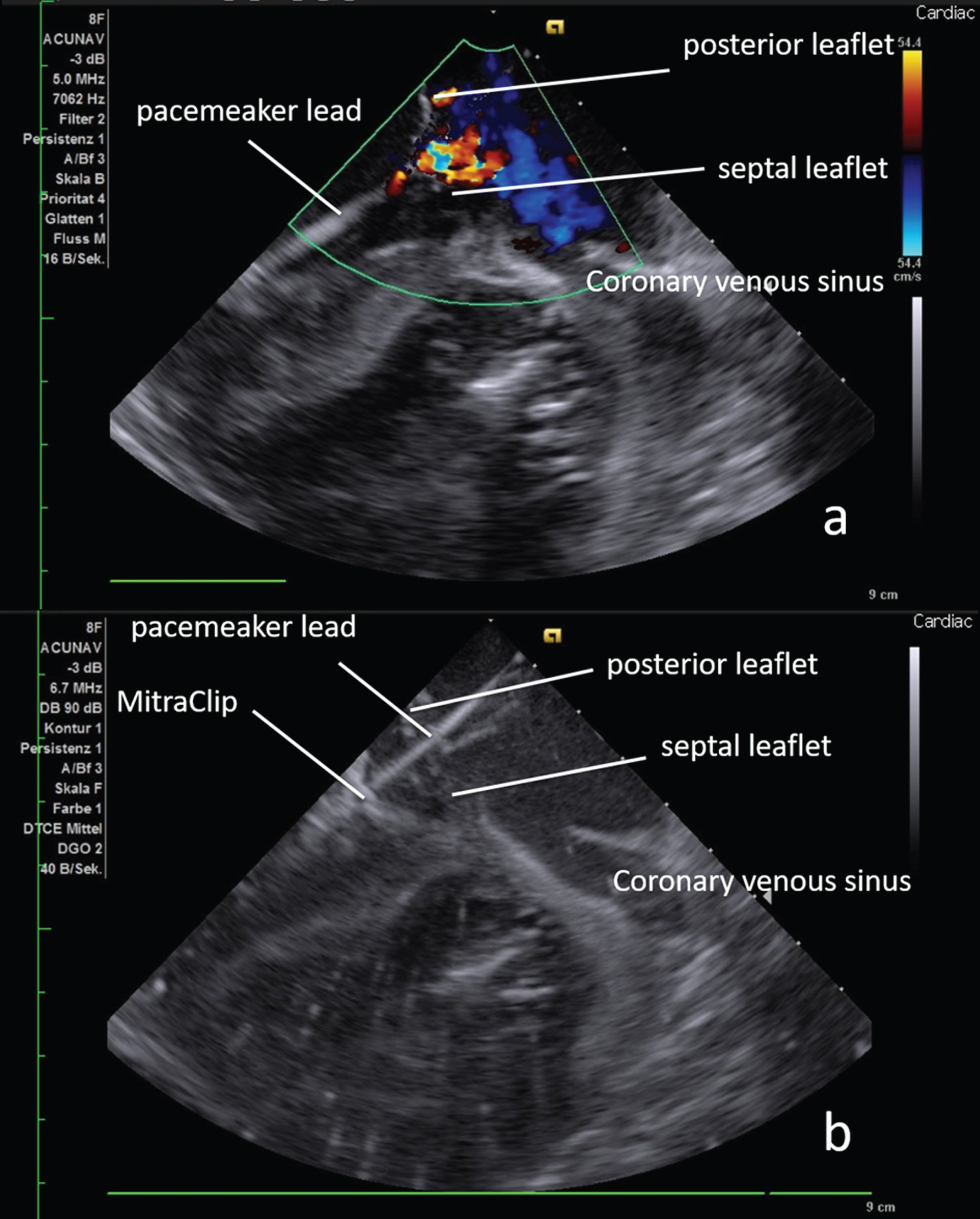
ICE guided grasping maneuver at the posteroseptal commissure. Posteroseptal commissure with a pacemaker cable crossing the valve. The coronary sinus and a transversal view of the mitral valve with a MitraClip in place are also displayed (a). Image (b) is taken after advancing the MitraClip just below the targeted leaflets in preparation for grasping. (For moving images also see Supplemental Video 2).
In each position careful clockwise and counterclockwise rotation may be necessary to improve the probe position for optimal image acquisition of the targeted commissure.
During the procedures, the probe positions correlated well with the angulations found in our 3D printed heart models. None of our patients required treatment of the antero-posterior commissure, which is why we cannot provide any images in this regard. In one patient the ICE probe entered an inferior phrenic vein, when it was advanced from the femoral vein, which was immediately noticed and corrected without any further problems.
Procedural success was achieved in 8 (72.7%) of the 11 patients, in whom EETVr was attempted. In 2 procedures clip implantation failed due to severe tricuspid annulus dilatation and lack of leaflet coaptation hindering successful grasping. In 1 patient the procedure was aborted as neither TEE and ICE nor TTE offered sufficient imaging quality.
Out of the 8 successful procedures, in 6 (75.0%) only 1 clip was implanted, while in 2 (25.0%) procedures two clips were deemed necessary to sufficiently reduce TR. Irrespective of the number of implanted clips, in none of the patients tricuspid stenosis (i.e., trans-tricuspid gradient>3 mmHg) after clip implantation was noted. In total, 7 NTR/NT and 3 XTR MitraClip devices were implanted. However, it is important to note that the XTR version of the clip only became available during the study period, which is why initial procedures had to be performed solely with the NTR/NT clips. According to the largest vena contracta, tricuspid regurgitation was significantly reduced at the time of discharge (p = 0.011). In none of the procedures complications, such as major and minor bleeding, emergency surgery, procedural mortality, stroke, cardiac tamponade, hemodynamic instability or technical failure of the device, occurred.
In 6 patients ICE was used in addition to TEE guidance to improve visualization of the targeted commissures. In 2 patients ICE image quality was too poor to support safe guidance, resulting in abortion of the procedure in one patient. TTE was successfully used in another patient. Mean procedural time tended to be longer in cases with ICE guidance. However, also an increased number of combined mitral and tricuspid procedures in these patients (50% vs. 40%) has to be noted. Other procedural characteristics were comparable in patients with and without additional ICE guidance. Detailed description of procedural characteristics and outcomes of patients treated with or without additional ICE can be found in Table 2 and individual baseline and procedural characteristics of each patient who underwent ICE guided EETVr are depicted in Table 3.
Procedural characteristics and outcomes
Procedural characteristics and outcomes
Data are presented as mean±standard deviation or number (%). VC vena contracta, ∗only patients with successful clip deployment are included in this analysis.
Procedures with Intracardiac Echocardiography (ICE) guidance
aIn this patient transthoracic echocardiography was used to finish the procedure. antsep anteroseptal commissure, ICE intracardiac echocardiography, PAP pulmonary artery pressure, postsep posteroseptal, RV right ventricular, TAPSE tricuspid annular plane systolic excursion, TR tricuspid regurgitation.
In one patient (TEE only guided) a clip detachment was noted the day after the procedure. One patient in our cohort (ICE guided group) died within 30 days following the procedure. Death was considered as a consequence of global heart failure and was not associated with the procedure.
The main findings of our study were: 1) ICE was a useful tool in EETVr procedures where TEE offered poor visibility of the tricuspid valve. 2) The steering maneuvers of the ICE catheter found in the 3D models were well applicable in all of the treated patients. 3) According to our experience, ICE guidance was safe and resulted in comparable technical results as found in TEE guided procedures with sufficient image quality.
It is, however, important to mention that in this study ICE was used as an additional tool to allow a safe and effective grasping maneuver when TEE image quality alone was considered not sufficient. TEE was still required to maneuver the CDS within the right heart and to align the clip according to the targeted commissure before starting the actual grasping.
Performance of intracardiac echocardiography in EETVr
TEE currently is the most widely accepted imaging modality for EETVr [15]. It allows evaluation of all aspects of the patient’s individual cardiac anatomy, including 2D and 3D visualization. Thus, as a procedural imaging tool it can be used to maneuver the CDS in the right atrium/ventricle, orient and align the clip according to the targeted commissure and may also offer sufficient image resolution to allow safe grasping of the leaflets.
However, due to the anatomical distance between the TEE probe - located in the esophagus - and structures of the right heart, TEE may be of limited value in terms of visualization of the tricuspid valve. Shadowing during the grasping maneuver, caused by the CDS may additionally aggravate the performance of TEE and is therefore another aspect where ICE may offer a potential solution.
To date only case reports exist for ICE and other alternative imaging techniques in EETVr [10]. However, in our high-risk patient population additional imaging was felt to be necessary in more than fifty percent of the procedures. In two thirds of these patients EETVr was completed successfully by implementing ICE.
As demonstrated in our 3D printed model, the multidirectional steerability of the ICE catheter may allow visualization of all three commissures. Operators, however, should keep in mind that great variation of the tricuspid valve anatomy may be found between patients and our proposed angulations may not be suitable in every patient [16–19]. Furthermore, none of our patients required treatment of the anteroposterior commissure, which is why we did not validate the probe position regarding this target.
It is important to note that ICE was only available as a 2D imaging modality in our study. According to our experience 2D ICE is helpful during the grasping maneuver and to determine the amount of entrapped leaflet material within the clip (leaflet insertion). It appears to be less useful in terms of orienting the clip. Furthermore, we found that the closest possible approximation between the transducer of the ICE catheter and the targeted area may be necessary to achieve the best possible image resolution.
In our non-ICE guided population one patient was found to have clip detachment one day after the procedure. Future studies should therefore also clarify whether the use of ICE positively effects leaflet insertion in EETVr as a consequence of improved visibility of the valve.
Despite the mentioned advantages, ICE is still an invasive procedure and therefore not useful as a screening tool. Generally, 2D and 3D TTE and TEE are the most important tools to assess the patient’s individual anatomy and suitability for EETVr. In patients where screening echocardiograms already suggest limited value of TEE as a guiding tool, the suitability for ICE should ideally be confirmed before the procedure. Unfortunately, due to the limited number of patients we were not able to investigate patient characteristics predicting the feasibility of intraprocedural ICE imaging. This may be important, as tricuspid visibility using ICE was poor in 2 patients, corresponding to one third of the patients where TEE was felt incapable of guiding the procedure. However, ICE guided procedures require a learning curve implying that increased experience with this technology may further improve the results.
Intraprocedural TTE has also been reported as an alternative guiding option, and has successfully been used in one of our patients [20, 21]. To reduce excessive radiation exposure for the echocardiographer, fluoroscopy should not be used during TTE image acquisition.
Potential future of intracardiac echocardiography in EETVr
Since prognostic implications have been shown for severe tricuspid regurgitation, potential treatment strategies are highly warranted in this patient population [22, 23]. Furthermore, the vast majority of patients who present with clinically apparent TR suffer from significant co-morbidities, prohibiting any surgical treatment option [24]. These individuals may benefit from transcatheter interventions such as EETVr. In this context, following the promising first results of the single-arm TRILUMINATE clinical trial (NCT03227757) the randomized TRILUMINATE pivotal trial (NCT03904147), comparing EETVr with medical treatment alone, is underway [5]. With increasing numbers of EETVr procedures there will also be an increased need for alternative imaging modalities for patients who are not suitable for TEE guidance. Pozzoli et al. described a case, which was performed in conscious sedation, under ICE and fluoroscopy guidance only [10]. This may be relevant for patients who cannot undergo endotracheal intubation or individuals with cardiac cirrhosis and associated esophagus varices, a frequent comorbidity of long-standing severe TR. Furthermore, 3D capable ICE catheters are already available and may further enhance the potential options of this imaging modality. This technology is likely to allow commissural alignment and orientation of the EETVr device in the right atrium, which is a major limitation of 2D ICE.
Limitations
The present investigation can offer only limited experience in terms of ICE in percutaneous tricuspid repair with the MitraClip device. We can therefore not finally conclude that ICE as an additional imaging modality in patients where TEE performs poorly justifies the potential disadvantages. It is important to keep in mind that ICE is still an invasive and therefore potentially harmful procedure, although we have not observed any ICE related complications in our cohort. Furthermore, we included only late stage TR patients with significantly dilated TR annuli. The propagated ICE angulations may be different in patients with smaller right heart chambers.
However, despite the mentioned limitations, this study demonstrates that ICE may offer an additional, or even alternative imaging modality in patients with limited TEE performance during transcatheter tricuspid repair.
Conclusions
In conclusion, since TEE guidance may show significant limitations in a significant proportion of patients undergoing transcatheter tricuspid valve repair, additional imaging techniques are highly warranted. As demonstrated in this initial evaluation, the ICE probe could be maneuvered precisely to the targeted commissure and ICE, thus, could be applied as a useful additional imaging tool in most of these patients. The technical results of the procedure were comparable to conventional TEE guidance (TEE with sufficient image quality). Larger studies evaluating the role of ICE in EETVr, including the identification of patient characteristics predicting the necessity and also the feasibility of ICE based on pre-procedural TEE assessment, are needed.
Funding
This work was financially supported by the Helmholtz Association through programme-oriented funding.
Conflicts of interest
Alexander Lauten is an advisor for SJM/Abbott and TricValve, he received research support from Edwards and SJM/Abbott outside the submitted work. Ulf Landmesser reports personal fees from Abbott outside the submitted work. The other authors have nothing to declare.
Ethics approval
Ethical approval for data collection was obtained from the local institutional review board (EA4/079/17).
Consent to participate
All patients gave written informed consent to the procedure.