
Abstract
A 33 years’ old male complained of excessive salivation with frequent swallowing and spitting, which resulted in communication disturbance, reduced quality of life, and social embarrassment for 19 years. He had been diagnosed as sialorrhea and submandibular gland hyperfunction by stomatologist, then had unilateral submandibular gland resection 13 years ago, but the symptom relief was not satisfactory. After that, he had been treated with glycopyrrolate for less than a year, which was withdrawn because of the short duration of symptomatic control after each tablet take-in and intolerable side effects. With the wish to receive a new treatment with long term effectiveness, low re-operation risk and normal preserved saliva secretion function, the patient was subject to MWA for the right submandibular gland. After systematic clinical evaluation, US-guided percutaneous MWA was successfully performed with an uneventful post-operative course. The volume of the right submandibular gland and ablated area were measured precisely by an ablation planning software system with automatic volume measurement function based on three-dimensional reconstruction of the pre-operative and post-operative enhanced magnetic resonance imaging (MRI) raw data. Finally, the ablated volume was calculated as 62.2% of the whole right submandibular gland. The patient was discharged 1 day after the operation, with symptoms relieved significantly, the mean value of whole saliva flow rate (SFR) decreased from 11 ml to 7.5 ml per 15 minutes. During the follow up by phone three months after operation, the patient reported that the treatment effect was satisfactory, whereas the SFR value became stable as 7 ml per 15 minutes, drooling frequency and drooling severity (DFDS) score decreased from 6 to 5, drooling impact scale (DIS) score decreased from 43 to 26. US-guided percutaneous MWA of submandibular gland seems to be an alternative, minimal invasive, and effective treatment for refractory sialorrhea.
We described a patient with refractory sialorrhea treated successfully with ultrasound (US) guided percutaneous microwave ablation (MWA).
Introduction
Sialorrhea or drooling refers to unintentional saliva spillage, mainly caused by dysphagia and saliva excessive secretion. For patients with good swallowing function, it refers to frequently swallowing or spitting due to true or hysterical excessive saliva [1]. Sialorrhea may cause peri-oral dermatitis, peculiar smell, hydration, communication and sleep disturbance, embarrassment, and social withdrawal, therefore the quality of life can be seriously affected [2]. Many treatment options have been proposed for sialorrhea in previous studies, including medication, botulinum toxin injection, pharmacological intervention, surgery, radiotherapy, and most importantly, treatment of the primary disease [1, 3–7]. Microwave ablation (MWA) has been proposed in recent years as a safe, feasible and effective treatment for many malignancies, such as hepatic malignant tumor, kidney malignancy, thyroid malignancy, breast malignancy, and so on [8, 9]. MWA has also been used for volume reduction in some patients with organ hypertrophy. Yu et al. firstly reported the use of MWA for treatment of sialorrhea with a satisfactory effect [10]. However, no report has been seen about the application of MWA for refractory sialorrhea after surgical resection and treatment response evaluation with contrast-enhanced imaging techniques. Herein we described a patient with primary refractory sialorrhea treated with US-guided percutaneous MWA successfully with satisfactory outcome.
Case report
A 33 year old male complained of excessive salivation with frequent swallowing and spitting, which resulted in communication disturbance, reduced quality of life, and social embarrassment for 19 years. He was diagnosed as submandibular gland hyperfunction and sialorrhea in 2007, which was based on symptoms, increased unstimulated whole saliva flow rate (SFR), and mild submandibular gland duct dilation revealed on sialography. The medical history included surgery and medication treatment history after that. First, he was referred to left submandibular gland resection in a stomatological hospital. The frequency of saliva swallowing decreased slightly after surgery, but still unsatisfied. Then the patient was treated with glycopyrrolate (take-in orally 10 mg three times per day) for less than a year, which was terminated due to short duration of symptom relief (3–4 hours after each tablet take-in) and intolerable side effects (constipation and dysuria). In order to exclude possible underlying psychogenic factors, the patient also visited psychology clinic, found no special result in the psychological assessment. After that, he visited the stomatology clinic again, consulted about other alternative treatments. Parasympathetic nerve blockade and other oral surgery were rejected for possible complications, botulinum toxin injection was also rejected for inconvenience of repeated injection because the patient was in military service. The patient wished to receive a treatment with long term effectiveness, low risk of re-operation and normal salivary secretion function preserved. After learning of MWA as a new method of submandibular gland partial destruction in literature, the patient visited our institution and asked for MWA in August 2020. Physical examination showed a 3 cm long skin scar in the left submandibular region; palpation found that the right submandibular gland was soft without swelling and tenderness, and the bilateral parotid glands and bilateral cervical lymph nodes were not enlarged. The mean pre-operative SFR was 11 ml per 15 minutes, which was measured by the patient at 7am for 5 days under the guidance of stomatologist, which indicated excessive saliva secretion. The severity of symptoms was evaluated by drooling frequency and drooling severity (DFDS) score and a modified drooling impact scale (DIS) for adult sialorrhea patients, which scored as 6 and 43. The initial laboratory tests revealed no special finding, including blood routine test, blood coagulation function, liver and kidney function, thyroid function test.
Pre-operative US and contrast enhanced ultrasound (CEUS) imaging examination were both performed on an ultrasound scanning equipped with a 4–10 MHz probe (Sequoia; Siemens, Germany). The right submandibular gland was scanned under the thyroid preset with high resolution priority parameter setting. The conventional T1 and T2 weighted imaging (WI) of three sections were obtained on a 3.0-T MRI scanner with minimal slice thickness of 3 mm, a gradient strength of 40 mT/m, a gradient slew rate of 200 mT/ms (Magnetom Verio; Siemens; Germany). The enhance contrast agent was gadopentetate dimeglumine (Magnevist; Bayer Schering; Germany). T1WI, T2WI and enhanced T1WI imaging of three sections were all collected, to prepare enough raw data for precise volume measurement of the original gland volume and ablation area. Herein a third-party software system named as Demetics Ablation Surgery Planning & Evaluation System (Demetics Medical Technology Co. Ltd, China) with automatic volume measurement function was used. Based on the imported three sequencies of MRI raw data in DI-COM format, the system can trace the margin of target lesion after setting several markers on the images of three sections, then show the accurate volume.
Pre-operative US imaging (Fig. 1 C&D) and enhanced MR (Fig. 3 A&B) demonstrated a homogeneous isoechoic gland with normal size. With the original measured volume of the right submandibular gland as 6.17 ml, the target ablation area was determined (Fig. 1 B). avoiding potential damage to the branches of facial artery (Fig. 1 C) and submandibular gland duct inside. Then 3 puncture paths (Fig. 1 D) were planned to obtain the predetermined ablation rate, more than 50%.

MWA plan: A. Normal anatomical location of parotid, submandibular and sublingual glands. B. Percutaneous MWA was planed in order to reduce the volume of the gland and salivary secretion. C. Pre-operative B mode ultrasound imaging (longitudinal section) showed a well-defined isoechoic gland (3.7×1.9 ×3.0 cm, estimated volume about 11.4 ml). The target ablation area was determined as the superficial side of the submandibular gland (white loop), avoiding the branches of facial artery (the solid arrow) and submandibular gland duct inside. D. Pre-operative B mode ultrasound imaging (transverse section) showed 3 puncture paths for MWA (marked with star) needed to get ablation rate more than 50%.
After the contraindications of ablation were excluded, real-time US guided percutaneous MWA under conscious sedation and local anesthesia was scheduled on the second day after admission to the hospital. The MWA generator (Microwave Ablation system MTI-5A; Nan Jing Great Wall Medical Equipment Co. Ltd, China) with a water cooled circulating MWA antenna (Microwave antenna XR-A1610W; Nan Jing Great Wall Medical Equipment Co. Ltd, China) was used.
The main procedure plan was: 1. pre-operative CEUS examination to evaluate the blood perfusion in the gland, 2. intravenous sedative anesthesia, 3. percutaneous puncture and injection of isolation fluid to avoid damage to adjacent structures, 4. MWA of the target area, 5. Intra-operative CEUS to assess the size of ablated area. During the sedative anesthesia procedure, 1 mg midazolam was slowly injected through a peripheral vein of left upper limb to ease tension of the patient; then 0.1 mg fentanyl (recommended dosage 0.02 mg/kg) was slowly pumped into the vein to relief intraoperative pain. Then, normal saline of 8–10 ml was precisely injected into the space between targeted ablation area and surrounding tissue under real-time US guidance (Fig. 2 A), to protect the surrounding tissue.

US guided percutaneous MWA procedure: A. Isolating before MWA: lidocaine was diluted to 0.005 g/ml and then injected between platysma muscle and submandibular gland (white loop) to separate the upper and lateral side of the target area from the surrounding tissue. B. The microwave antenna (solid arrow) was placed in the target area under ultrasound imaging guidance. C. Remarkable hyperechoic gas formation (dotted arrow) was observed around the antenna 1 minute after activating the microwave ablation device. D. Intra-operative CEUS imaging showed non-enhancement in the target area, with the longest diameter of the ablated area being 2.15 cm on the transverse section. E. Pre-operative SWE displayed the whole gland as homogeneous soft tissue, the mean young’s modulus (Emean) is 4.4–5.1 KPa. F. Post-operative SWE showed the stiffness of the ablated area increased significantly, Emean > 20 KPa.

Pre-operative and post-operative three-dimensional reconstruction of MRI with the ablation surgery planning and evaluation system. A. Pre-operative contrast enhanced MRI demonstrated a well-defined submandibular gland with homogeneous enhancement, which was traced with yellow line automatically. B. The three-dimensional reconstruction image based on three sections of pre-operative MR displayed the whole lateral submandibular gland vividly, and the measured volume was 6.17 ml. C. Post-operative contrast enhanced MRI showed no significant enhancement in the central area of the gland, which was traced with green line. D. The volume of ablated area was measured as 3.84 ml, the general ablation rate was up to 62.2%.
Next step, we inserted the microwave antenna into the target area (Fig. 2 B), started the dynamic MWA procedure till gasification reaction of hyperechoic cloud (Fig. 2 C) was observed in all the puncture path; then sequentially performed MWA on the second and third puncture path; finally, intraoperative CEUS was performed to evaluate the local treatment response after injecting sonovue™ 2.0 ml (Fig. 2 D). During the supplementary ablation of residual area, intra-operative CEUS was used to monitor the ablation. The output power of the MWA generator was set as 35 w. When the whole target area showed no enhancement on CEUS, we ended the ablation procedure. The whole ablation time was 8 minutes 42 seconds.
Two-dimensional shear wave elastography (SWE) was performed on the second day after operation, showed that the stiffness of ablated area was significantly harder than that before ablation. The whole submandibular gland displayed homogeneous stiffness with mean young’s modulus (Emean) of 4.4–5.1 KPa on pre-operative SWE (Fig. 2 E), and the ablated area showed heterogeneous higher stiffness, Emean > 20 KPa (Fig. 2 F). Post-operative enhanced MRI showed no significant enhancement in the central area of the gland (Fig. 3 C). The volume of ablated area measured by automatic volume measurement system was 3.84 ml (Fig. 3 D), therefore the general ablation rate was up to 62.2%.
The course after procedure was uneventful, except mild swelling on the ablated area which disappeared in 2 days. The SFR measured on the first day after operation was 7.5 ml per 15 minutes. Then the patient was discharged 1 day after operation.
The value of SFR was unstable, ranging from 7.5 ml per 15 minutes to 10.5 ml per minutes in the first week after operation, then became stable and kept decreasing slightly from two weeks after operation (Fig. 4A). During the follow up three months after operation, the previous symptom was significantly relieved, with the mean value of whole SFR decreased from 11 ml to 7 ml per 15 minutes, DFDS score decreased from 6 to 5, DIS score decreased from 43 to 26 (Fig. 4B).
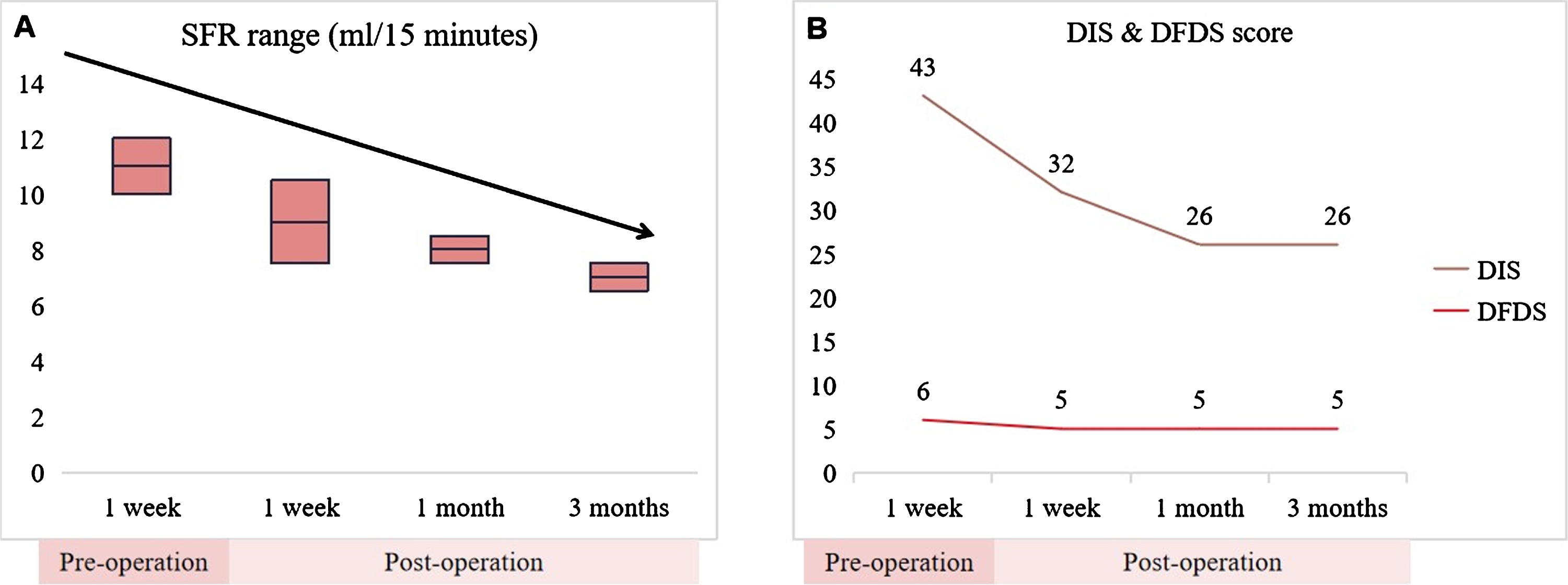
The quantification assessment results of sialorrhea before and after operation: A. The SFR value kept decreasing and became stable from two weeks after the operation; B. The DFDS score decreased slightly from 6 to 5 after the operation, while the DIS score decreased significantly from 43 to 26.
The definition of sialorrhea
Sialorrhea is equivalent to drooling in a broad sense in many previous reports, which refers to unintentional saliva spillage out of mouth, mainly caused by dysphagia and saliva excessive secretion. However, strictly speaking, it only refers to sensation of abundant saliva, caused by salivary hypersecretion, can be a syndrome of a variety of pathological factors [1]. It is considered as physiological sialorrhea in infants during deciduous tooth eruption, the structures of oral cavity and orofacial neurological control development, which usually disappears before 4 years’ old. Otherwise, pathological sialorrhea should be considered [7].
The prevalence of sialorrhea varies greatly by different etiology, whereas the prevalence of severe drooling is relatively high, up to 75% in children with cerebral palsy [11], and 60% in adults with Parkinson’s disease [12, 13].
The etiology of sialorrhea
In term of etiology, sialorrhea can be caused by neuromuscular dysfunction, sensory impairment, excessive saliva secretion, abnormal orofacial structure or head position, mental disorder and several rare syndromes [4]. One of the mechanisms of neurological deficit related sialorrhea is motor dysfunction of oral-facial muscles, resulting in dysphagia or delayed swallowing reflex, which can be seen in patients with cerebral palsy, Parkinson’s disease, cerebrovascular events, amyotrophic lateral sclerosis, family dysautonomia, drug reaction, and so on. The other one is sensory dysfunction, mainly seen in children with mental retardation and old people with Alzheimer’s disease who were not aware of saliva spillage then can’t swallow initiatively. Patients with abnormal oral structure or head posture can’t store saliva in the mouth, also lead to sialorrhea. Sialorrhea caused by the above three pathogenies usually has normal SFR. Excessive saliva secretion can be caused by oral inflammation, gastroesophageal disease, poisoning, cholinesterase inhibitor or other drugs, and parasympathetic hyperfunction. The influence of mental factors on salivation can’t be ignored either, especially hysterical salivation. Hysteria can cause various sensory and motor dysfunction, but lack of corresponding organic lesion, is often manifested as pharyngeal foreign body sensation or subjective excessive saliva secretion difficult to swallow, resulting in frequently splitting out. However, whole SFR is usually normal and no foreign body can be found in laryngoscope and imaging examination.
The clinical assessment and management of sialorrhea
It’s a common consensus that sialorrhea can be induced and influenced by various factors. In addition to definite diagnosis and disease severity assessment, clearance of etiology and identification of the underlying factors for each individual case is important to determine the adequate treatment strategy adapted to each patient’s needs.
Therefore, the diagnosis and treatment strategy should be made by a multidiscipline sialorrhea team, including stomatologist, maxillofacial surgeon, neurologist, psychiatrist and behavioral intervention therapist.
In this case, systematic examination and evaluation was carried out in the department of stomatology and psychology with only one positive result, that was, the stimulated SFR significantly increased. No special founding in oral examination, head and neck MRI, sialography, ultrasonography of salivary gland, and psychological evaluation. The patient was diagnosed as refractory primary sialorrhea and salivary gland hyperfunction.
The most commonly used quantification assessment of drooling or sialorrhea were drooling quotient, DFDS and DIS, all of them were mainly designed and validated in children [14, 15]. No appropriate quantification assessment was reported for adult patients with primary salivary hyperfunction. In order to assess the severity of symptoms and the impact of quality of life as precisely as possible before treatment, we developed a new DFDS (Table 1) and DIS (Table 2) scale suitable for adult patients with good swallowing function. The former one was modified from Thomas-Stonell and Greenberg version [16], the latter one was modified from Susan and Hilary version for children with drooling [17].
Drooling frequency and drooling severity scale for adult sialorrhea
Drooling frequency and drooling severity scale for adult sialorrhea
Based on Thomas DFDS scale. Three treatment approaches and clinical factors in the reduction of drooling. Dysphagia 1988;3:75.
Drooling impact scale for adult sialorrhea and salivary gland hyperfunction

The three common approaches treating sialorrhea aim at reducing saliva secretion include medication (glycopyrrolate, scopolamine and atropine), pharmacological intervention (botulinum toxin or other drugs injection), surgery (neurectomy, salivary duct relocation or ligation, salivary gland removal). Other treatments are aimed at promoting the development of swallowing reflex and improving the orofacial neuromuscular function, such as oral-motor or behavior therapy, tongue acupuncture, muscle vibration, which have also been reported to be effective for neurological impairment resulted sialorrhea [18, 19]. However, none of them is effective for all patients.
Anticholinergic agents were used to indirectly control of drooling. The mechanism of medication treatment is blocking acetylcholine transmission to inhibit the parasympathetic stimulation, thus reducing saliva secretion. But the side effects can be more distressing than the original problems for the patient, thus it is not suitable for long-term treatment. On the other hand, only limited evidence was found to support these drugs as effective intervention [4, 21].
Several surgical approaches have been proposed for the control of drooling aimed at reducing saliva secretion, including gland removal, resection or blockage of parasympathetic innervation of the gland and salivary duct ligation or relocation. The former two can cause extreme dry mouth, taste sensation loss and movement impairment of the tongue. The latter one is the most widely used method in children with neurological disorders, which has the risk of gland swelling and aspiration pneumonia [22, 23].
Botulinum toxin can inhibit the release of acetylcholine from the cholinergic nerve ending and is currently one of the most widely accepted treatment options for both adult and children. The effectiveness rate was reported as 42%–61.5%, with response rate decreased from 69% at 2 weeks to 49% at 24 weeks after injection [24]. The procedure of botulinum toxin injection includes anesthesia and US imaging guided injection at 2–3 sites of the parotid and submandibular glands, the effect was reported to occur at 1–8 weeks and last for 2–6 months post-injection, then the other injection is needed [25]. The side effects include bruising, branches of facial artery and submaxillary artery embolization, facial nerve damage [26–30].
The patient selection of intervention treatment
For patients failed on the treatment of medication and surgery, intervention treatment can be considered. Appropriate patient selection is crucial to successful treatment.
The indication of salivary gland MWA for volume reduction should include: 1. patients have been clearly diagnosed as primary sialorrhea mainly caused by salivary gland hyperfunction, without neuromuscular dysfunction, sensory impairment, abnormal orofacial structure, or mental disorder. 2. Imaging examination demonstrated a normal or enlarged salivary gland without tumors or other diseases. 3. Pre-operative US showed safe puncture path for the ablation.
As the etiology of sialorrhea is various and many factors can lead to relapse or aggravation of the symptoms, second intervention might be needed during the follow up. The patient must reach a consensus with the therapist about the ablation rate goal, and accept the possibility of need for second ablation.
The contraindication of salivary gland MWA are as follow: 1. Patients with suspected malignant lesion of salivary gland; 2. Patient with severe bleeding and coagulation dysfunction; 3. Patient with server systematic diseases and intolerance of surgery.
In this case, the patient preferred a minimal invasive treatment with long-term efficacy, low re-operation risk and preserved normal saliva secretion function. Therefore, he rejected surgery for potential complication of facial nerve injury and secondary xerostomia. Botulinum toxin injection was also given up due to potential damage of facial nerve and pharyngeal muscles, inconvenience for repeated injection per 4–6 months.
The application of CEUS in the diagnosis and treatment of salivary gland disease
Quantitative CEUS was reported helpful in the discriminate malignant focal lesion of parotid gland from benign one, but can’t be recommended for clinical use for limited supportive studies [31]. However, intra-operative CEUS plays an important role in the evaluation of ablation area size to get ideal ablation range, which was proven to be an effective and practical treatment response evaluation method during the intervention procedure [32–34]. As the perfusion imaging is available only for 2 to 3 minutes in the CEUS examination of superficial organs using sonovue™, it is not applicable to monitor long ablation procedure, especially duration more than 5 minutes. But it can be very useful in monitoring the supplementary ablation of residual lesion found in intraoperative CEUS.
Image-guided thermal ablation has been applied for tumors of many organs for many years, and has been reported to be as effective as resection in both radiological and clinical response, which has the advantages such as less blood lose, less pain, less analgesia use, shorter operation duration, shorter hospital stay, less cost than conventional surgical resection [35–37]. MWA is a kind of minimal invasive thermal ablation therapy, which can be performed precisely under imaging guidance to produce localized permanent tissue coagulation and necrosis and destruction of micro-vascular net in the target area without damage of surrounding tissue, nerve and vascular [38].
Ablation has been recommended as the first line treatment of small hepatic malignant tumor < 3 cm in clinical practice guideline of hepatic cell carcinoma (HCC) (9), and proved as an effective treatment for hypersplenism [39, 40]. This is the first report of MWA applied on the treatment of refractory sialorrhea, with feasibility efficacy and safety validated. However, the required proper ablation output power and duration for symptom remission is unknown, and further prospective studies are needed.
In summary, US-guided percutaneous MWA is an effective, safe, minimal invasive procedure for salivary hyperfunction and refractory sialorrhea, which is promising to become an alternative treatment in the future.
Conflict of interest
The authors declare that there are no conflicts of interest regarding the publication of this article.
Footnotes
Acknowledgments
This work was supported in part by the National Natural Science Foundation of China (Grants 81671695, 81725008 and 81927801), Fundamental Research Funds for the Central Universities (Grants 22120190213), Shanghai Municipal Health Commission (Grants 2019LJ21 and SHSLCZDZK03502), and the Science and Technology Commission of Shanghai Municipality (Grant 19DZ2251100).